HPV vaccine strategy part 1
The vaccine strategy part 1
HART has made a clear evidence based stance on covid vaccines. Our remit is to educate the public on medical harms and there is another vaccine which deserves close scrutiny in this regard. In order to give it the attention it deserves we will be publishing three articles on the subject:
Part 1: Efficacy
Part 2: Safety
Part 3: Ethics
Background to HPV and cervical cancer
The HPV (Human Papilloma Virus) vaccine is intended to prevent women dying from cervical cancer. HPV is so widespread that almost any sexual contact will result in exposure. Usually the immune system clears any problems, but when chronic infection persists, it can cause cellular abnormalities and precancerous lesions that can ultimately progress to cancer. Prevention approaches previously comprised regular smear testing for precancerous cellular abnormalities, with local treatment by either cryotherapy or laser therapy. This programme has changed in recent years to include HPV vaccination of girls to prevent infection and screening to detect presence of HPV. Because of the widespread occurrence of this virus in the adult genital tract, the vaccine programme is aimed at girls before their first sexual contact. There are over 200 strains of Human Papilloma Virus which are numbered, with types 16 and 18 responsible for around 75% of cervical cancers in Europe. The time between infection and precancerous lesions ranges from 1 to 10 years. For further information, see The Green Book, Chapter 18a, HPV.
Nearly all cervical cancer deaths are preventable by a simple Pap screen with appropriate follow up. Cervical smears used as a screening test have certainly reduced cervical cancer levels but the programme is expensive and results in overtreatment and psychological harm, all of which could be reduced by reducing the burden of HPV infection and treatments. (Please see appendix for more details of the history and recent changes to the UK cervical cancer screening programme).
Vaccination
HPV vaccination for adolescent girls was introduced in the UK in 2008 and the programme extended to boys from 2019. HPV vaccine choices were until recently, Cervarix (Glaxo Smith Klein – GSK), against 2 strains and Gardasil (Merck), against 4 strains. In the UK these have now been replaced by the newer Gardasil-9. Globally, HPV vaccine coverage in 2023, showed 27% of girls aged 9–14 years received an initial vaccination. In Australia, Denmark, and New Zealand, the vaccine coverage was extremely high (90%); in the UK it was around 50–70%, in the USA ~60% whereas in Asia, Africa and parts of northern Europe, the vaccination uptake was low.
From 2019, vaccines have also been offered to UK boys. Their chance of benefit from cervical cancer reduction is not zero – in that their partners might be affected – but it comes close. They may benefit from a reduction in oral, penile and anal cancers but these are significantly rarer risks so any benefit in a reduction will be significantly smaller.
The aims are two fold – a reduction in mortality from cervical cancer and a reduction in the need for screening for pre-cancerous lesions.
Cancer deaths
One difficulty for demonstrating efficacy of the HPV vaccines in eliminating deaths from cervical cancer is that, certainly in the UK, overall death rates were already falling steadily over four decades prior to the 2008 introduction of HPV vaccination.
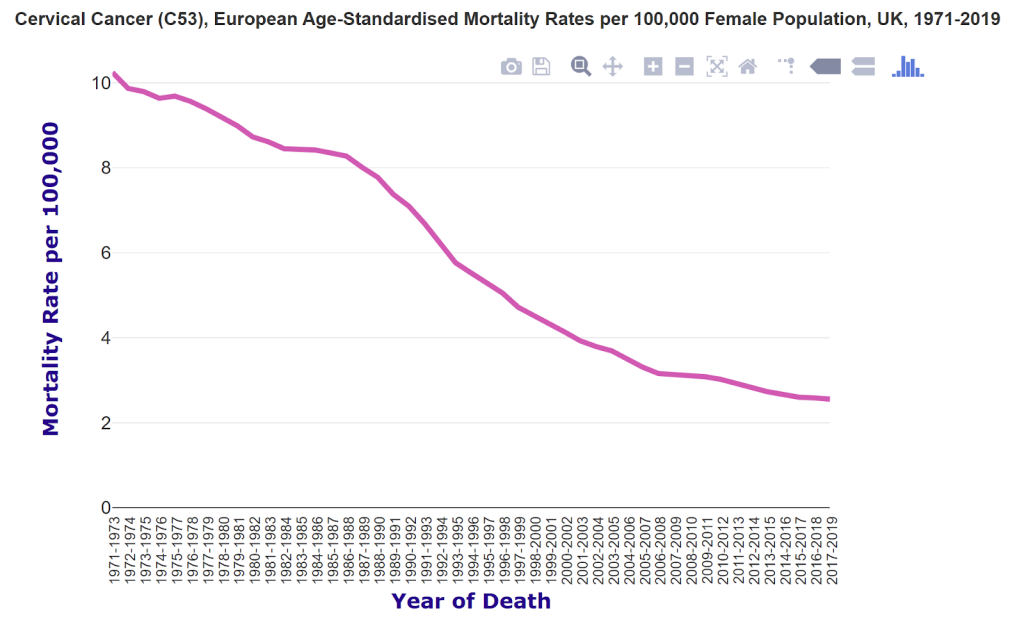
Figure 1: Death rates in the UK from cervical cancer falling steadily prior to the launch of the HPV vaccine.
Data on deaths in younger age groups is encouraging however and there were no deaths under 25 years since 2020 and there has been a significant decrease in the 25-29 year old age group. The cohort of the first 13 year old vaccinated girls reached 25 years in 2019, however, older women aged 13-18 were offered catch up vaccines from 2009-2010.
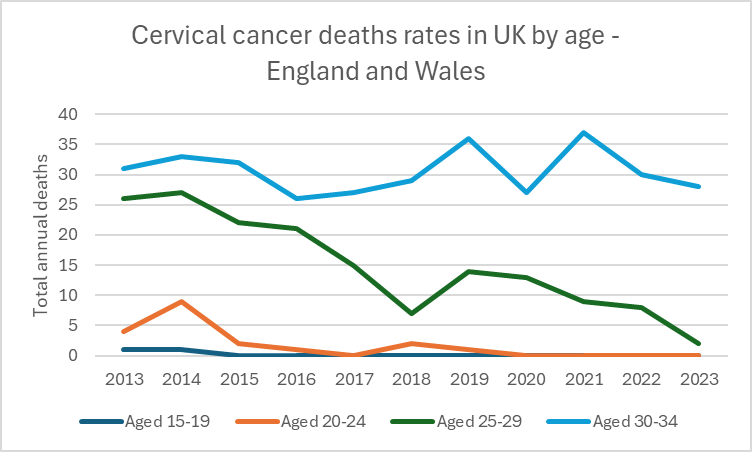
Figure 2: Death rates in England and Wales by age for cervical cancer diagnoses
If we assume the fall in mortality since 2014 in the younger age groups is all due to vaccines then the total cancers prevented over that nine year period comes to 185. (It is impossible to know what the would have happened in the absence of vaccines so other factors and a continuation of the declining trend are totally excluded from the sum). If any reduction continues into older age groups over time the size of the benefit will increase.
For the USA, making the same assumptions about mortality since 2014 would lead to an estimate of only 140 lives having been saved since 2014. Clearly, despite the lower uptake in the US, there would be an expectation of more saved lives if the UK data were extrapolated, suggesting other factors are indeed contributing to the decline.
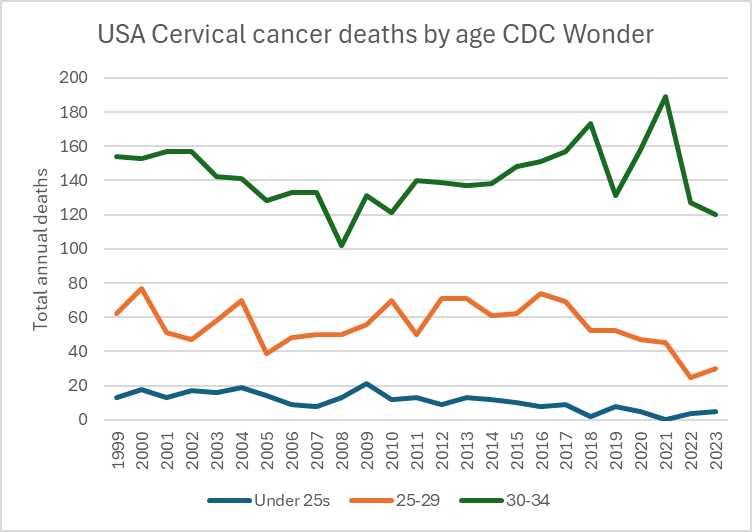
Figure 3: Cervical cancer death rates in US by age
Impact on cancer cases
The clinical trials that led to rollout did show a reduction in infections with HPV but they were too small and of too short duration to measure the impact on deaths. The rollout was begun regardless and so any impact on death must be assessed on the whole population which is always problematic given there is no control group.
Australia began vaccinating 12 year olds in 2007 against HPV 6, 11, 16 and 18 in 2006. The prevalence of HPV infections has reduced since in both the unvaccinated and vaccinated populations.
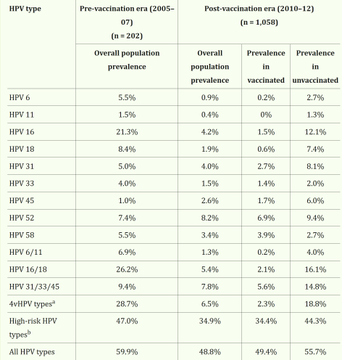
Figure 4: Australian prevalence of HPV infection by type (N.B. vaccines were against HPV 6, 11, 16 and 18)
There was a dramatic fall in high grade (pre cancerous) lesions in 20-24 year olds. The trouble is – it started too early to be from vaccination. (The 12-13 year olds first vaccinees reached 20 in 2014 at the earliest).
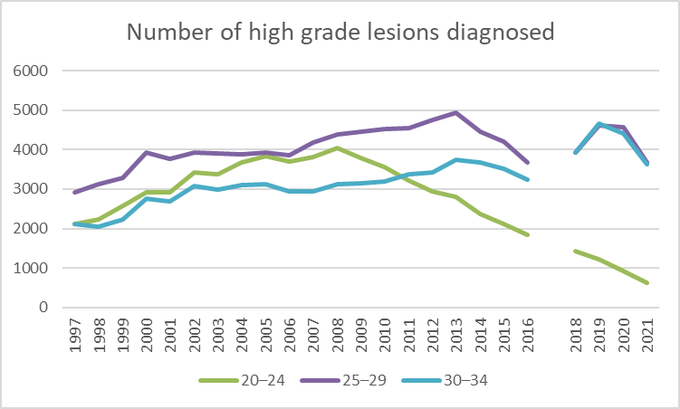
Figure 5: High grade (pre-cancerous) cervical lesions by age in Australia.
The cancer rate in this age group has not changed.
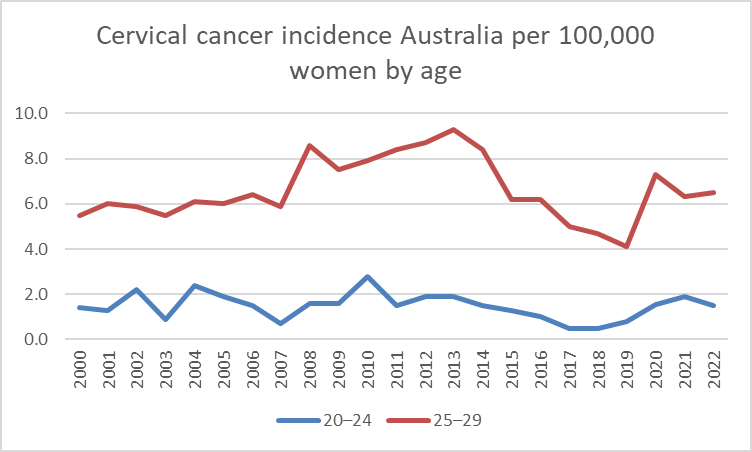
Figure 6: Cancer diagnoses by age in Australia
The same story can be seen in the USA. The three graphs below are from a CDC publication and show rates of squamous cell carcinoma (SCC) and the far rarer adenocarcinoma (AC) in three age bands. In each graph, the dotted “predicted line” gives the expected rates and the solid line is a “modeled” line through the observed rates.
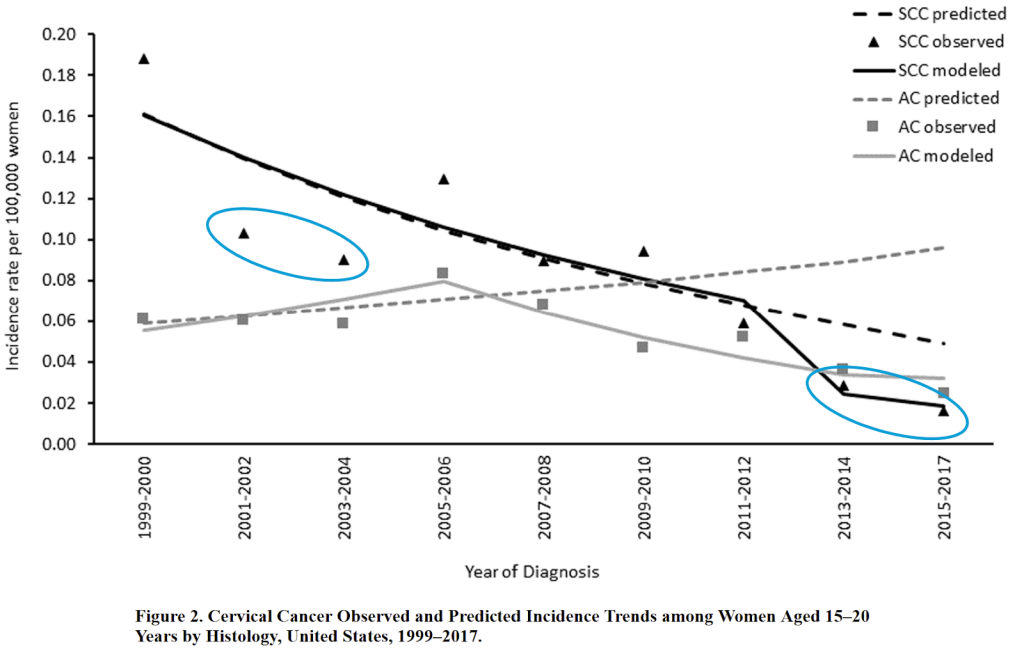
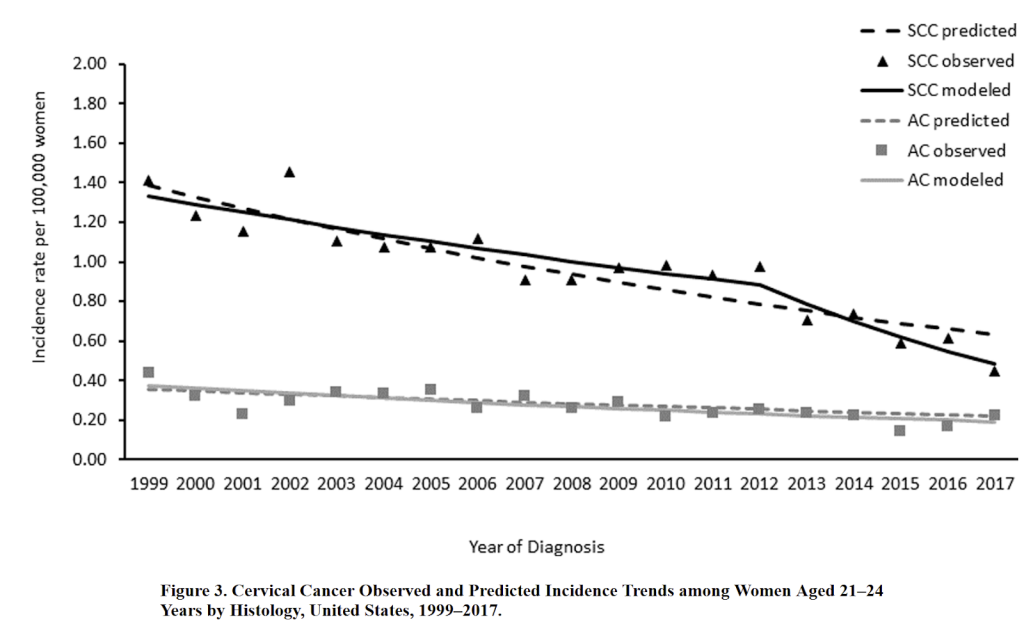
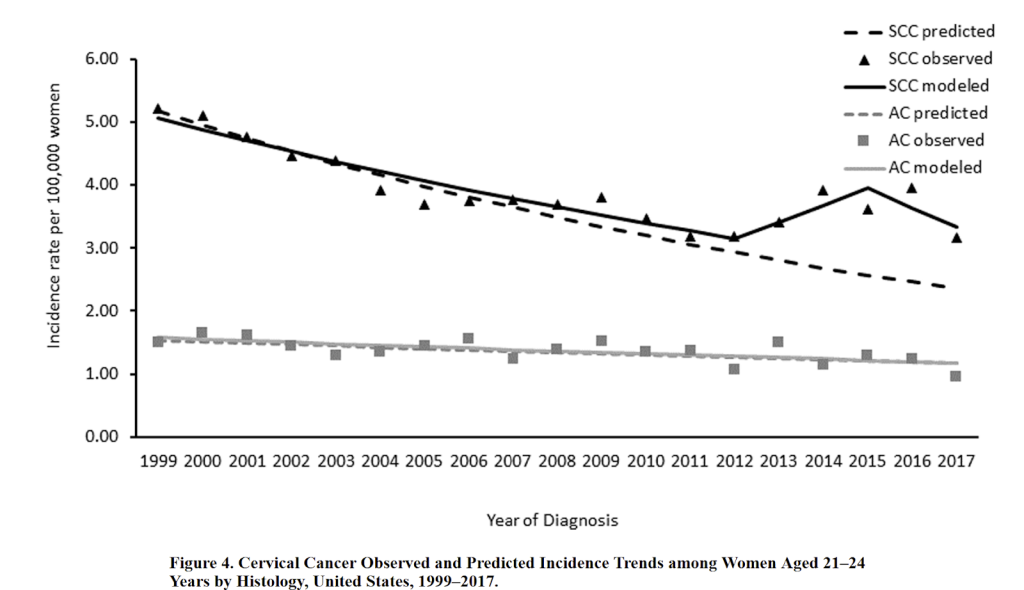
Figures 7: Rates of squamous cell carcinoma (SCC) and adenocarcinoma (AC) in young women –
As shown in the top graph, the ‘modeled’ line has ignored earlier dips in 2001-2004 (circled in blue) but then makes a massive deviation after similar dips later on in 2013-2017. This could be described as ‘cherry picking’. The bottom graph was mislabelled and is for women aged 25-29 years. There has been minimal change in cancer rates in under 25 year olds and a rise in those over 25.
And in the UK? The graph below is from Cancer Research UK. The red arrows show when women aged 20-25 years stopped being invited for screening. However, the subsequent increased cancer cases among 25-34 year olds matches what was seen in the USA where screening was not stopped.
The green arrows show when the first cohort of vaccine receipts reached that age group. There is no sign of a benefit in terms of cancer diagnoses.
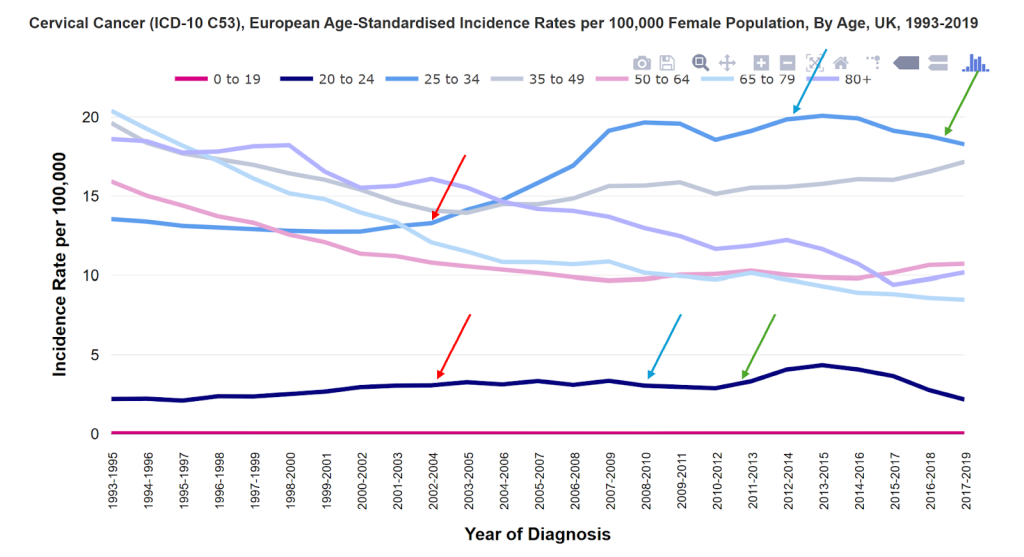
Figure 8: Cancer research data on cervical cancer incidence by age UK
Conclusion
HPV vaccines were rolled out after trials that were too small and too short to show any mortality benefit. Therefore there has been a global experiment to see if there would be a mortality benefit if the population were vaccinated. Early evidence shows a reduced mortality despite similar levels of cancer in the young female population. The mortality benefit thus far works out at 27000 girls needing to be vaccinated to have prevented one cancer death. However, projecting into the future it is estimated that only 94 girls would need to be vaccinated to prevent a life long risk of dying of cervical cancer.
Concerns have however been raised, that along with a fall in the HPV strains targeted by the vaccines, there has been a concomitant rise in non-vaccine strains instead. The empirical evidence to date shows no sign of this risk emerging. However, the full impact of all these changes for each age group and stage of life will need time to be seen as we measure cancer rates and mortality rates over time.
The benefit must be balanced against any risk, especially as the benefit is seen at a median age of 60 years whereas any harm is potentially seen from the age of 13. Part 2 will address the safety issues.
Appendix: Background on cervical cancer screening:
UK Cervical Screening – background
In the UK, Pap screening was used on its own for decades with HPV testing introduced in 2012 alongside it. From 2016 an HPV test has become the primary screening tool with Pap smears only carried out where an HPV test is positive. Screening is offered every 3 years for women aged 25–49 years. Screening intervals increase to every 5 years in women aged 50–64 years. From 2025 the screening interval was extended to every 5 years for 25-49 year olds who are either vaccinated or have a negative HPV test. If screening is positive further interventions follow from a follow up smear if the results are low risk to a clinic appointment at colposcopy where the cervix can be directly assessed and sampled. In the UK, this is an organized programme with invitations and reminders sent by post with some text message reminders. Over the past 20 years, there has been a slow, but steady, decline in screening uptake across the age brackets with a slightly lower screening uptake in 25 to 49 year-olds (66%) versus women aged 50–64 years (74%).
Public Health backlash
When Public Health Wales extended cervical screening to 5 years a petition was begun on change.org gathering over 1.3 million signatures to retain 3-year cervical screening intervals. Public Health Wales had to issue an apology explaining the change from 3 years to 5 years was not well communicated, but is ‘evidence-based’ for HPV screening that is more effective at detecting early abnormalities. In a paper published in the BMJ Open, the acceptability of extending HPV cervical screening intervals from 3 to 5 years was assessed in England. When communicating about longer screening intervals, they found that explaining the relationship between HPV, abnormal cells and cancer with the longer intervals being safe is impactful, as is receiving information from ‘trusted’ sources. Unsurprisingly, those with a history of abnormal cytology are less accepting of the change despite their negligible risk if they are HPV negative.
Self-Sampling Approaches
The acceptability of HPV screening using self sampling (particularly among non attenders) is quite high, but little research has been done to assess the basis behind the choice of either a clinician-collected sample versus self-sampling. The psychological impact of a positive test result from HPV screen was associated with a greater level of anxiety. Text responses from 381 women showed there were information needs about HPV causes, epidemiology, prevention, treatment, and questions about cervical cancer risk and implications relating to clinical, fertility, clearance, and partners, if positive for HPV. The concerns raised from the survey meant the policy makers worked with PHE to include FAQs on the HPV positive test result letter.
