

another open letter on the potential risks
23 February 2023
Response to the RCOG position statement on COVID-19 vaccine safety in pregnancy and breastfeeding
We refer to our appeal sent to you on 31 October 2022 and the subsequent letter to the president dated 2 December 2022, to which regrettably we have not received a reply. In the appeal, we outlined in detail scientific evidence highlighting the need for caution regarding the administration of COVID-19 vaccines to pregnant women.
We are dismayed that your latest position statement on this issue does not appear to have taken any of our concerns into account. It only cites a single publication, in which the evidence is insufficient to support your position. Below, we refer to sections of your statement that are clearly based on incomplete and / or incorrect information. Once again, we appeal to you in the strongest possible terms to reconsider the ethical and scientific grounds of your advocacy for these experimental products to be given to pregnant women.
1) Benefits of COVID-19 vaccines to pregnant women
You claim unequivocally that “vaccination is the best way to protect” pregnant women and their babies against the risks of COVID-19. This implies evidence not only for effectiveness but also proven superiority compared to other measures. Below, we outline data to challenge this claim.
a) Effectiveness of COVID-19 vaccines
A recently (Jan 2023) published study led by Dr Anthony Fauci, who had oversight of the pandemic response in the US, states in its summary that viruses including SARS-CoV-2 “have not to date been effectively controlled by licensed or experimental vaccines”.
It is now commonly acknowledged that COVID-19 vaccines do not prevent infection or transmission, and their sole benefit is claimed to be a reduction in risk of hospitalisation and death. However, observational, real-world data do not support this claim.
Data from UK
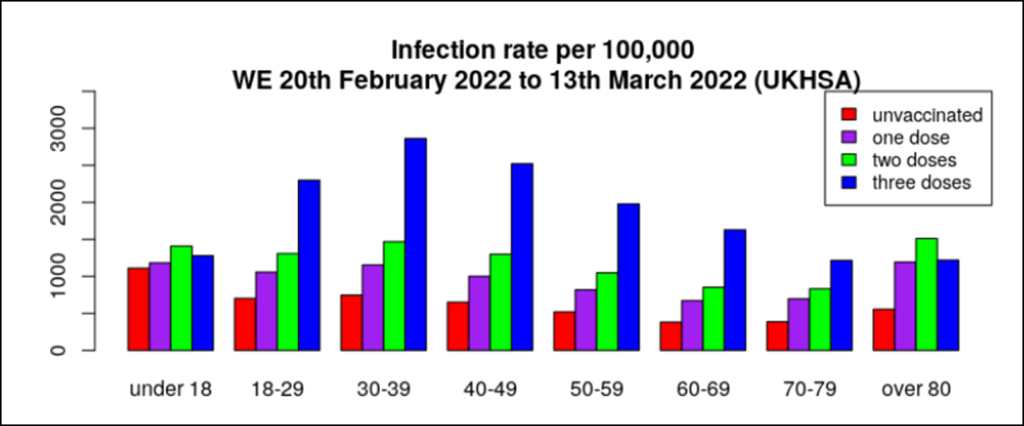
Data from England in March 2022 did not indicate that vaccination and specifically the booster doses had a beneficial effect on COVID-19 infection (Figure 1). In fact, vaccine effectiveness compared to the unvaccinated was as low as -300% in certain age groups.
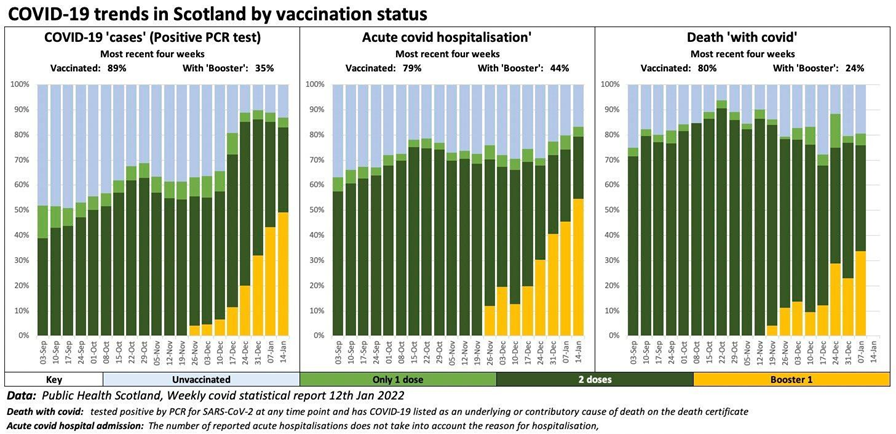
Scottish data indicated similar trends regarding COVID-19 infections, as well as hospitalisations and deaths (Figure 2). Subsequently, both the UKHSA and Public Health Scotland (PHS) stopped publishing relevant data.
Data from New South Wales (NSW) Australia
New South Wales (NSW) Australia has continued to publish relevant data, which do not indicate a favourable effect of COVID-19 vaccination on hospitalisations (Figure 3).
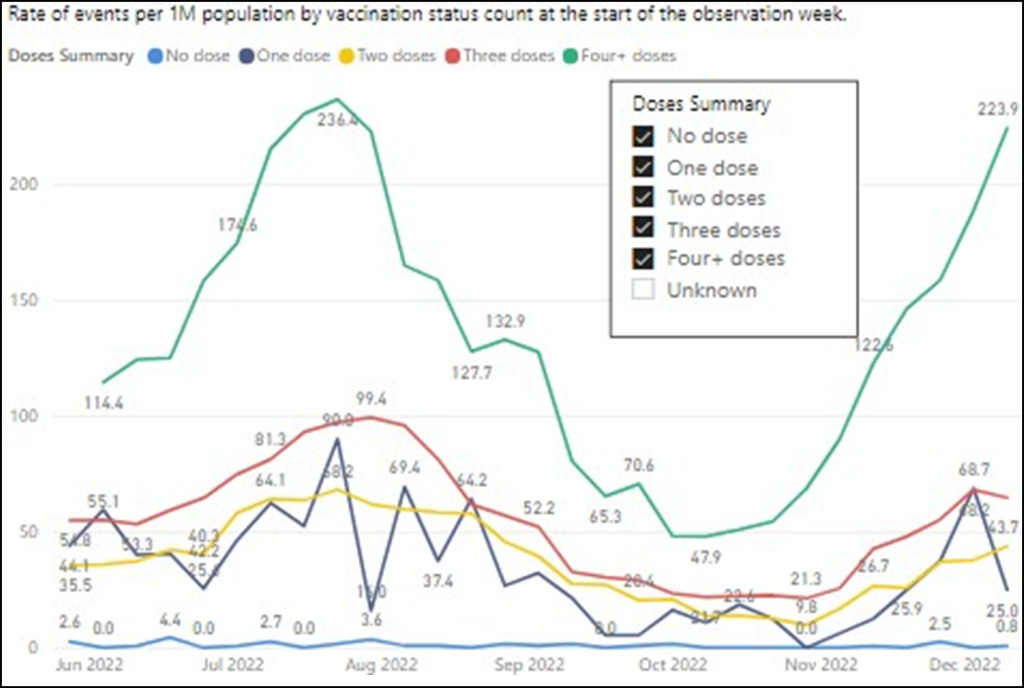
by vaccination status (not necessarily because of COVID)
Data from Cleveland, USA
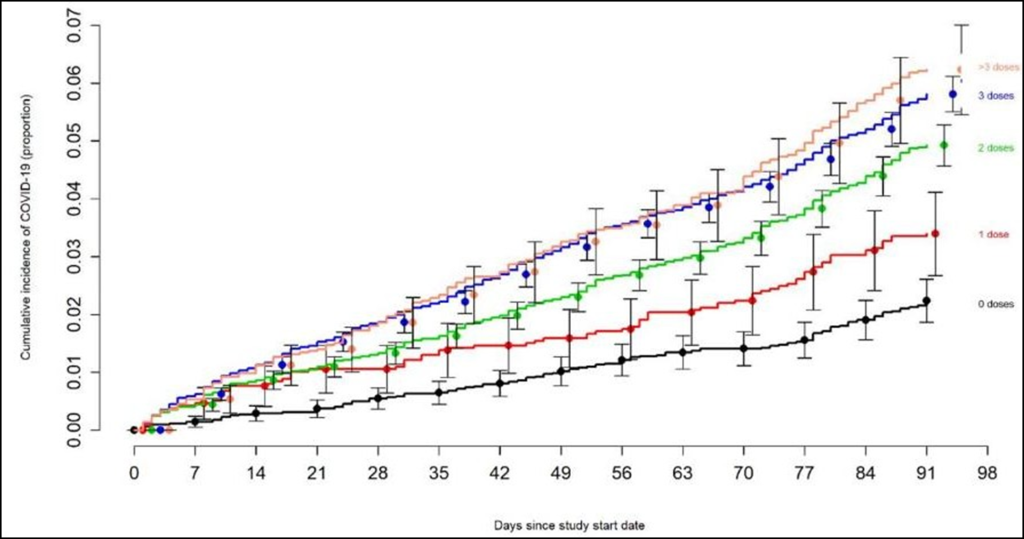
A study from the Cleveland Clinic, USA into the effectiveness of the bivalent COVID-19 vaccine recently published on the preprint server indicated increasing susceptibility to COVID-19 with increasing numbers of booster doses in over 51,000 employees, thereby challenging the claim that repeated vaccination improves protection (Figure 4).
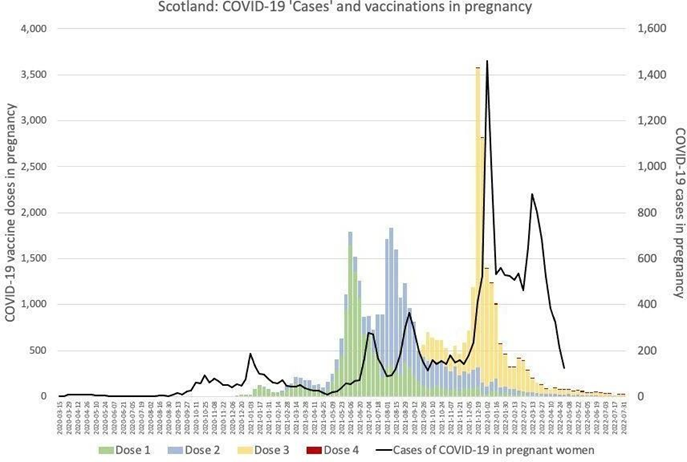
b) Effectiveness of COVID-19 vaccines in pregnancy
Once again we refer to data from Scotland included in our previous appeal, which do not indicate that COVID-19 vaccines have been successful in reducing COVID-19 infections during pregnancy. Conversely, infections appear to spike following vaccinations (Figure 5).
It has been postulated that SARS-CoV-2 placentitis may increase the risks of adverse pregnancy outcomes but may occur without causing any maternal symptoms at all. As COVID-19 vaccines do not prevent infection, we propose that any hypothesis that they reduce adverse pregnancy outcomes would need to be thoroughly investigated and include a plausible mechanism of action.
c) Protection against adverse outcomes of COVID-19
Claiming that COVID-19 vaccination is the “best way” to protect against adverse outcomes suggests evidence of favourable comparison to other interventions, not referenced in your statement.
Below we refer to just a few studies showing effectiveness of other measures that COVID-19 vaccines need to be compared to before making the categorical claim of superiority.
Early Treatment
As with any infectious disease, any opportunity to treat symptoms as early as possible will ameliorate the course of illness and reduce the risk of adverse outcomes. Multiple protocols here, here and here have been developed and applied successfully.
Natural immunity
Naturally developed immunity is long-lasting and broad with protection against more than one variant. A recent study has demonstrated that protection from previous infection against severe, critical and fatal COVID-19 disease is 76% superior to vaccination. At a point in time when most of the population has already had multiple exposures to SARS-CoV-2, this data must be considered in any statement recommending further vaccination.
Vitamin D3
A systematic review and meta-analysis indicated an inverse correlation between COVID-19 mortality risk and Vitamin D3 status, suggesting fatal outcomes may be reduced by normalizing Vitamin D3 levels.
Physical activity
A recently published retrospective cohort study of over 194,000 adults with COVID-19 infection concluded that “there were protective associations of physical activity for adverse COVID-19 outcomes across demographic and clinical characteristics”.
2) Safety of COVID-19 vaccines in pregnancy
a) Safety data
Your claim of COVID-19 vaccine safety rests largely on the fact that a substantial number of pregnant women have received them without any apparent concerns. Retrospective observational analysis is the lowest level of research evidence, especially when observations are neither structured nor comprehensive. This level of evidence is not sufficient for reassurance about the safety of a product based on a completely novel technology. Voluntary registries such as the V-safe COVID-19 Vaccine Pregnancy Registry are not equivalent to well-designed prospective clinical trials: follow-up is inconsistent and incomplete, with no standardisation or systematisation and no tracking of participants.
Data collection is largely dependent on self-reporting, and in view of the incessant insistence that COVID- 19 vaccines are unequivocally safe it is reasonable to assume that many may not appreciate any association between adverse events and their vaccination status, leading to significant under-reporting. Well-designed clinical trials with robust and meticulous follow-up, for the duration of a pregnancy and at least the post- partum period, would be required to investigate safety in pregnancy. Data regarding safety for the infant would require an even longer follow-up period. These studies have not been done.
b) Reports of adverse pregnancy outcomes
The claim that “no serious adverse events” have been recorded following COVID-19 vaccination in pregnancy is incorrect. The MHRA has received around 700 reports in the category “Pregnancy, puerperium and perinatal conditions” for the monovalent Pfizer/BioNTech COVID-19 vaccine alone, the majority of these serious. The reporting system in the US (VAERS) lists 1,301 cases of spontaneous abortions and 54 stillbirths, each having occurred within 7 days of COVID-19 vaccination. The possibility of a causative association has not been investigated by regulators, but instead appears to have been summarily dismissed without any further scrutiny.
A significant safety signal has been identified in a retrospective cohort study which reported a three times higher incidence of postpartum haemorrhage in triple-vaccinated women compared to double-vaccinated and to unvaccinated patients.
Your statement cites only a single cohort study on COVID-19 vaccination in pregnancy with data from March 2020 to July 2021. Notably, during the majority of this period, COVID-19 vaccines were either not available or not recommended for pregnant women. This study includes only 140 vaccinated women, most of whom (85.7%) received their vaccine in the third trimester, and is therefore not sufficiently comprehensive as a source of evidence to infer safety for all pregnant women.
c) Adverse events following COVID-19 vaccination
Secondary analysis of serious adverse events reported in the placebo-controlled Phase III randomized clinical trials of Pfizer/BioNTech and Moderna COVID-19 vaccines in adults led by Prof Peter Doshi (BMJ associate editor), showed an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated (1:800). For both vaccines, this risk was higher than the risk reduction for COVID-19 hospitalisation relative to the placebo group.
The UK government recently published an estimation of the numbers needed to vaccinate to prevent a COVID-19 hospitalisation. This showed that for those aged 20-39 in a risk group, between 10,700 and 59,500 need to be vaccinated with any dose to prevent a severe hospitalization, and this assumed vaccine effectiveness of at least 70% for at least six months. These numbers are orders of magnitude higher than the risk of a serious adverse event following vaccination. There is therefore an urgent need to reconsider the risk-benefit analysis, especially in view of evidence cited above showing high and durable protection following previous infection. This would be particularly critical in respect of young adults, including women of childbearing age.
Risk of thromboembolic events
The only serious adverse event that your statement refers to is rare blood clots following Astra-Zeneca COVID-19 vaccines. This was the standard of knowledge almost two years ago in March 2021 and informed UK government advice in June 2021. Evidence has rapidly evolved since then, showing that the risk of thromboembolic events and bleeding disorders is not limited to the Astra-Zeneca COVID-19 vaccine.
The MHRA Yellow card analysis of the monovalent Pfizer/BioNTech COVID-19 vaccine alone has over 23,000 reports in the combined categories of “Blood and lymphatic system disorders” and “Vascular disorders”. Over 78% of these were from females and over 62% were from people under the age of 50. The vast majority of these events were reported as serious. The US reporting system (VAERS), which allows for more transparency of data that the public has access to includes 13,334 reports of pulmonary embolism following COVID-19 vaccinations. 4,988 (37%) of these occurred within 7 days and 2,894 (21%) within 48 hours of vaccine administration. Whilst these reports do not prove causality, it must be questioned why the vaccine rollout has not been halted pending further investigations of these disturbing safety signals, especially in view in mounting evidence regarding waning effectiveness.
There is evidence that S glycoprotein (spike protein), the part of SARS-CoV-2 that the synthetic mRNA in the vaccines codes for, has significant pathogenicity on its own and may therefore be instrumental in causing endothelial and lung damage and inducing haemagglutination.
Your statement that “this side effect is so rare, we can’t know the exact risk” is outdated and misleading as it suggests that the risk is negligible when there are now multiple studies and real-life data indicating concern and the need for urgent further investigations. Two years following the rollout of COVID-19 vaccines to billions of people it is not acceptable to claim that risks cannot be known or quantified whilst it is clear that huge number of serious safety signals have not been adequately investigated.
Serious adverse events of special interest
It is essential to note that thromboembolic events are only one of several serious adverse events observed and described in association with COVID-19 vaccinations. These specifically include acute cardiac events and myocarditis, but also neurological conditions and death. Referring to myocarditis / pericarditis, it is now stated in the summary of Yellow Card reporting by the MHRA that “There has been a consistent pattern of higher reporting of these suspected events with both the monovalent COVID-19 Vaccine Pfizer/BioNTech and COVID-19 Vaccine Moderna”. We suggest that it is misleading, if not negligent, to omit these concerns raised in multiple studies, from any advice given to pregnant women.
3) COVID-19 vaccine technology
Your reference to the technology used in COVID-19 vaccines bears several inaccuracies. To state that they “do not contain ingredients that are known to be harmful” is misleading, and the claim that they are “quickly broken down once they have been injected” is simply incorrect. The comparison to “other non-live vaccines” is grossly inappropriate. Below, we elaborate on the evidence refuting your statements.
a) Comparison with other non-live vaccines
To suggest that reassurance regarding safety of COVID-19 vaccines in pregnancy may be drawn from data on “other non-live vaccines” completely ignores the fact that they are not even remotely comparable. COVID-19 vaccines are not just “new”, they are based on novel technology that has never previously been applied to humans on this scale. Whilst they may not “cause infection”, they utilise synthetic mRNA to code for the most pathogenic part of SARS-CoV-2 (S glycoprotein), which is then produced by the human body in unknown quantities for an unknown period of time with an unknown effect on the immune system. There was therefore significant uncertainty regarding the short- and long-term safety of these products when they were rolled out to large populations.
b) Metabolism of COVID-19 vaccine ingredients
Subsequent to initial uncertainty regarding safety of COVID-19 vaccines, there are now mounting studies and scientists raising significant concerns about observed and potential effects of several of their ingredients.
Synthetic mRNA
The mRNA in the vaccines is synthetic, with the uridine nucleoside replaced by pseudouridine for the purpose of delayed breakdown by the innate immune system. The knowledge about the precise effects on human physiology and immune function and therefore about safety remains far from established and concerns regarding potential health risks have been raised.
It has been categorically stated that mRNA vaccines will not alter human DNA. However, a preclinical study demonstrated that Pfizer/BioNTech mRNA (BNT162b2) is reverse transcribed into DNA of human liver cells in vitro as fast as 6h post-exposure.
Contrary to your statement that “within a few days of vaccination there will be no vaccine mRNA left”, a study has shown that “vaccine-associated synthetic mRNA persists in systemic circulation for at least 2 weeks”. This was replicated in a study finding spike mRNA vaccine sequences to be circulating in blood for up to 28 days. Another study found that “mRNA vaccination stimulates robust GCs [germinal centers in lymph nodes] containing vaccine mRNA and spike antigen up to 8 weeks post vaccination”.
Lipid nanoparticles (LNPs)
As we referenced in our previous appeal, Pfizer’s own pharmacokinetics studies showed that the lipid nanoparticles (LNPs) used to carry the mRNA are distributed to and accumulate in the ovaries at significant concentrations. LNPs are designed to cross cell membranes, which normally create a protective barrier to certain substances, and this includes the placental barrier. Potential ovarian toxicity of nanocarriers was warned about in a paper published 10 years ago. A further study from 2018 highlighted the potential adverse effects of nanoparticles on the reproductive system.
S glycoprotein (Spike protein)
As referenced above, the S glycoprotein (spike protein coded for by the mRNA) has demonstrated pathogenicity on its own. In addition, and as mentioned in our previous appeal, additional concerns based on molecular mimicry relate to similarities between spike glycoprotein and human proteins which may lead to an adverse autoimmune reaction. It is specifically relevant to pregnant women that the SARS-CoV-2 spike glycoprotein was found to share similarities with 27 human proteins relating to oogenesis, uterine receptivity, decidualization, and placentation in a study published in the American Journal of Reproductive Immunology.
4) Requests for correction and transparency
We submit the following as a Freedom of Information (FOI) request:
- Please disclose details of any correspondences relating to your dealing with our concerns outlined in our previous appeal
- Please disclose details of any correspondences relating to your decision-making process that led to your complete disregard of any of our concerns and references in your recent position statement:
- In the interests of transparency and clarity of the position you continue to maintain, please provide the following supporting evidence to justify your position statement:
- Any and all publications, studies and data you rely upon to claim that vaccination “is the best way to protect against the known risks of COVID-19 in pregnancy for both women and babies”, i.e. which show not only that COVID-19 vaccines are effective but also superior to any other measures.
- References of the animal studies which you claim provide satisfactory evidence that COVID-19 vaccines cause no harm to pregnancy or to fertility.
- The full study protocols “monitoring both the mother and baby’s health during pregnancy and for a year after the baby’s birth”.
- Any and all publications, studies and data you rely upon to claim that “worldwide data shows that the rates of miscarriage were the same in those who had received a COVID-19 vaccine during pregnancy as in the general population who had not been vaccinated”.
- The full MHRA analysis of “reports of miscarriage and stillbirth in pregnant women who have received the COVID-19 vaccines and have not identified any pattern”.
We hope you acknowledge that your statement falls well below the standards of a well-sourced document and therefore expect you to issue a corrected and transparent version based on up-to-date evidence as a matter of urgency so that both pregnant women and obstetricians may be guided appropriately in their decisions regarding COVID-19 vaccination.
We thank you for your attention to this most important matter and look forward to hearing from you.
Dr Julia Wilkens, MD, Consultant in Obstetrics & Gynaecology (former FRCOG)
Dr Hans Peter Dietz, MD PhD FRANZCOG DDU CU, Obstetrician & Gynaecologist & Urogynaecologist
Dr John Williams, FRCOG, retired Consultant in Obstetrics & Gynaecology
Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMedSci, Professor of Oncology, University of
London; Principal, Institute for Cancer Vaccines & Immunotherapy
Professor Richard Ennos, MA, PhD, Honorary Professorial Fellow, University of Edinburgh
Professor John Fairclough, FRCS, FFSEM, retired Honorary Consultant Surgeon
Professor David Livermore, BSc, PhD, retired Professor of Medical Microbiology
Professor Dennis McGonagle, PhD, FRCPI, Consultant Rheumatologist, University of Leeds
Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Honorary Professor of Professional
Practice, Buckingham University
Professor Roger Watson, FRCP Edin, FRCN, FAAN, Professor of Nursing
Lord Moonie, MBChB, MRCPsych, MFCM, MSc, House of Lords, former parliamentary under-secretary of
state 2001-2003, former Consultant in Public Health Medicine
Dr Najmiah K Ahmad, BM, MRCA, FCARCSI, Consultant Anaesthetist
Julie Annakin, RN, Immunisation Specialist Nurse
Helen Auburn, Dip ION MBANT NTCC CNHC RNT, registered Nutritional Therapist
Dr Ancha Bala-Joof BSc BSc MBChB MRCGP General Practitioner
Dr David Bell, MBBS, PhD, FRCP(UK), Public Health Physician
Dr Mark A Bell, MBChB, MRCP(UK), FRCEM, Consultant in Emergency Medicine
Dr Michael D Bell, MBChB, MRCGP, retired General Practitioner
Dr Alan Black, MBBS, MSc, DipPharmMed, retired Pharmaceutical Physician
Dr Gillian Breese, BSc, MB ChB, DFFP, DTM&H, General Practitioner
Mr John Bunni, MBChB (Hons), DipLapSurg, FRCS, Consultant Colorectal and General Surgeon
Dr H Burger, MRCGP, DRCOG, General Practitioner
Dr David Cartland, MBChB, BMedSci, General Practitioner
Caroline Cartledge, RM, BA (hons), Midwife
Angela Chamberlain, BSc (hons), Midwife
Dr Peter Chan, BM, MRCS, MRCGP, NLP, General Practitioner, Functional Medicine Practitioner
Michael Cockayne, MSc, PGDip, SCPHNOH, BA, RN, Occupational Health Practitioner
Mr Ian F Comaish, MA, BMBCh, FRCOphth, FRANZCO, Consultant Ophthalmologist
James Cook, NHS Registered Nurse, Bachelor of Nursing (Hons), Master of Public Health (MPH)
Dr Clare Craig, BMBCh, FRCPath, Pathologist
Dr David Critchley, BSc, PhD in Pharmacology, 32 years’ experience in Pharmaceutical R&D
Dr Sue de Lacy, MBBS, MRCGP, AFMCP, UK Integrative Medicine Doctor
Dr Jayne LM Donegan, MBBS, DRCOG, DCH, DFFP, MRCGP, General Practitioner
Dr Jonathan Eastwood, BSc, MBChB, MRCGP, General Practitioner
Dr Elizabeth Evans, MA(Cantab), MBBS, DRCOG, Co-founder UKMFA
Dr Christopher Exley, PhD FRSB, retired Professor in Bioinorganic Chemistry
Dr John Flack, BPharm, PhD, retired Director of Safety Evaluation, Beecham Pharmaceuticals,
Senior Vice-president for Drug Discovery SmithKline Beecham
Sophie Gidet, RM, Midwife
Dr Cathy Greig, MBBCh(Hons), General Practitioner
Dr Ali Haggett, Mental health community work, 3rd sector, former Lecturer in the history of medicine
Mr Anthony Hinton, MBChB, FRCS, Consultant ENT Surgeon, London
Dr Keith Johnson, BA, D.Phil (Oxon), IP Consultant for Diagnostic Testing
Fiona Jones, BSc(Hons), DipPreSci, Cert Med Ed, FRPharmS, MFRPSII, Clinical Pharmacist Independent
Prescriber (retired)
Dr Ros Jones, MBBS (Hons), DObstRCOG, MD, FRCPCH
Dr Tanya Klymenko, PhD, FHEA, FIBMS, Senior Lecturer in Biomedical Sciences
Dr. Eashwarran Kohilathas, BMBS, doctor and author
Dr Caroline Lapworth, General Practitioner
Dr Branko Latinkic, BSc, PhD, Reader in Biosciences
Dr Theresa Lawrie, MBBCh, PhD, Director, Evidence-Based Medicine Consultancy Ltd, Bath
Dr Felicity Lillingston, IMD, DHS, PhD, ANP, Integrated Doctor, Doctor of Humanitarian Services, Research
fellow
Dr Nichola Ling, MBBS, MRCOG, Consultant obstetrician, Clinical Advisor to Digital Child Health and
Maternity Programme NHS England
Katherine MacGilchrist, BSc(Hons) Pharmacology, MSc Epidemiology, CEO, Systematic Review
Director, Epidemica Ltd
Dr Geoffrey Maidment, MBBS, DRCOG, MD, FRCP, retired Consultant Physician
Mr Ahmad K Malik, FRCS(Tr & Orth), Dip Med Sport, Consultant Trauma & Orthopaedic Surgeon
Dr Ayiesha Malik, MBChB, General Practitioner
Dr Kulvinder S. Manik, MBChB, MRCGP, MA(Cantab), LLM, Gray’s Inn
Dr Sam McBride, BSc(Hons) Medical Microbiology & Immunobiology, MBBCh, BAO, MSc in Clinical
Gerontology, MRCP(UK), FRCEM, FRCP(Edinburgh), NHS Emergency Medicine & Geriatrics
Kaira McCallum, BSc, retired Pharmacist, Director of Strategy UKMFA
Mr Ian McDermott, MBBS, MS, FRCS(Tr&Orth), FFSEM(UK), Consultant Orthopaedic Surgeon
Dr Franziska Meuschel, MD, ND, PhD, LFHom, BSEM, Nutritional, Environmental and Integrated Medicine
Dr Alistair Montgomery, MBChB, MRCGP, DRCOG, retired General Practitioner
Dr David Morris, MBChB, MRCP(UK), General Practitioner
Dr Alan Mordue, MBChB, FFPH, retired Consultant in Public Health Medicine & Epidemiology
Margaret Moss, MA(Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
Theresa Ann Mounsey, BSc (hons) in midwifery studies
Dr Alice Murkies, MBBS, MD, FRACGP, General Practitioner and Medical Researcher
Dr Greta Mushet, MBChB, MRCPsych, retired Consultant Psychiatrist in Psychotherapy
Dr Angela Musso, MD, MRCGP, DRCOG, FRACGP, BS, General Practitioner
Dr Sarah Myhill, MBBS, Dip NM, Retired GP, Independent Naturopathic Physician
Dr Chris Newton, PhD, Biochemist working in immuno-metabolism
Dr Rachel Nicholl, PhD, Medical Researcher
Sue Parker Hall, certified transactional analyst (CTA, psychotherapy), MSc (Counselling & Supervision),
MBACP (senior accredited practitioner), EMDR practitioner, Psychotherapist
Dr Christina Peers, MBBS, DRCOG, DFSRH, FFSRH, Menopause Specialist
Rev Dr William J U Philip, MBChB, MRCP, BD, Senior Minister The Tron Church, Glasgow, formerly doctor
working in cardiology
Anna Phillips, RSCN, BSc Hons, Clinical Lead Trainer Clinical Systems (Paediatric Intensive Care)
Angharad Powell, MBChB, General Practitioner
Dr Gerry Quinn, PhD, Microbiologist
Dr Johanna Reilly, MBBS, General Practitioner
Jessica Righart, MSc, MIBMS, Senior Biomedical Scientist
Mr Angus Robertson, BSc, MBChB, FRCSEd (Tr & Orth), Consultant Orthopaedic Surgeon
Dr Jon Rogers, MBChB (Bristol), Retired General Practitioner
Mr James Royle, MBChB, FRCS, MMedEd, Colorectal Surgeon
Dr Salmaan Saleem, General Practitioner
Sorrel Scott, Grad Dip Phys, Specialist Physiotherapist in Neurology
Dr Rohaan Seth, BSc (hons), MBChB (hons), MRCGP, retired General Practitioner
Natalie Stephenson, BSc (Hons) Paediatric Audiologist
Dr Noel Thomas, MA, MBChB, DObsRCOG, DTM&H, MFHom, retired Doctor
Dr Livia Tossici-Bolt, PhD, Clinical Scientist
Tanya Wardle, RM, Registered Midwife
Dr Helen Westwood, MBChB, MRCGP, DCH, DRCOG, General Practitioner
Dr Carmen Wheatley, DPhil, Orthomolecular Oncology
Mr Lasantha Wijesinghe, FRCS, Consultant Vascular Surgeon
Dr Lucie Wilk, MD, Consultant Rheumatologist
