
Why bite the hand that feeds you?
All HART articles also on Substack. Please consider a PAID SUBSCRIPTION so we can continue our work. Comments are open so you can join in the conversation.
This headline appeared on BBC News on 14 May:

Sky News followed suit:
The headline also appeared in other mainstream outlets, for example The Times and the Daily Telegraph.
This episode actually illustrates all that is wrong with our relationship with Big Pharma.
The first thing that anyone who wants to critically analyse these statements should do is find the actual study paper itself. All that can be found is this brief paper, actually published in November last year.
This reveals these key features of the study design:
- ~18,000 patients >45 years old with pre-existing cardiovascular disease, no diabetes and a BMI > 27 (so overweight) were recruited.
- Half received placebo and half semaglutide (double blind).
- The primary cardiovascular endpoint was a composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke in a time-to-first-event analysis. Safety was also assessed.
- The mean (±SD) duration of exposure to semaglutide or placebo was 34.2±13.7 months, and the mean duration of follow-up was 39.8±9.4 months.
- The study was funded by Novo Nordisk
The headline result was this:
A primary cardiovascular end-point event occurred in 569 of the 8803 patients (6.5%) in the semaglutide group and in 701 of the 8801 patients (8.0%) in the placebo group (hazard ratio, 0.80; 95% confidence interval, 0.72 to 0.90; P<0.001).
Sounds impressive? Well, there are some problems with this.
- No all-cause data at all are presented, not even for mortality. As we saw with the trials for the covid mRNA injections, this can hide a multitude of issues. Mortality or hospitalisation, or other serious adverse events, could be substantially higher in the active group compared to placebo, but we wouldn’t know.
- The benefit in terms of cardiovascular outcomes is quite thin. It is reported by the news media as a 20% reduction, which is technically correct (8% down to 6.5%). But that is the relative risk reduction (RRR). The absolute risk reduction (“ARR”) is 1.5%. Put differently, you need to treat 66 people to prevent one primary cardiovascular event.
- The primary cardiovascular endpoint was a composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke but they don’t tell us how these are broken down. Given the huge difference between a lethal and non-lethal event this is a glaring omission.
- It is clear that the rate of adverse events (about which we are given no details) is quite significantly greater in the active treated group compared to placebo since “adverse events leading to permanent discontinuation of the trial product occurred in 1461 patients (16.6%) in the semaglutide group and 718 patients (8.2%) in the placebo group (P<0.001)” – a difference of 8.4%.
- Put differently, out of 100 treated, 8 would have discontinued due to adverse events.
Want more data? You can’t have it. According to the data sharing statement, the data will not be made available to others.
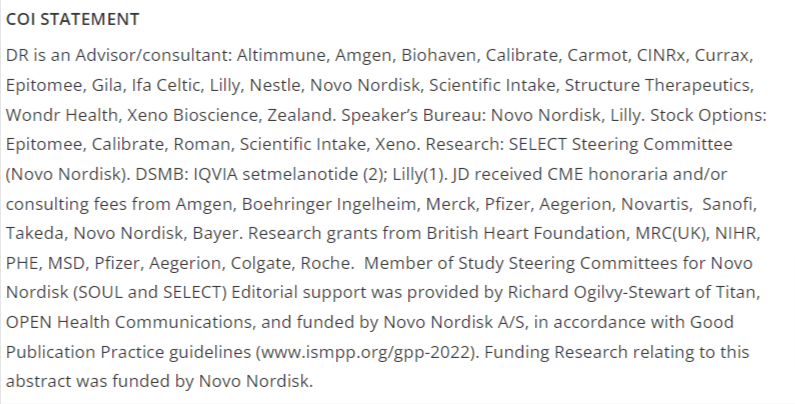
A look at the conflicts section in the paper is revealing but unsurprising:
As mentioned above, this study was actually published in November 2023, but the last few days have seen an absolute barrage of favourable mentions across broadcast and print media. The breathlessly enthusiastic reporting is something to behold.
Here is Amir Khan waxing lyrical – talking up the supply issues with the drug – about the results with absolutely no mention of any of the issues raised above. It would be remiss of us not to mention that to his credit, though, he DOES also mention the importance of non-pharmaceutical interventions such as diet. (Ironically, he – correctly – points out the harms of long-term inflammation, seemingly oblivious to the now overwhelming evidence that the mRNA injections cause a significant issue in this regard.)
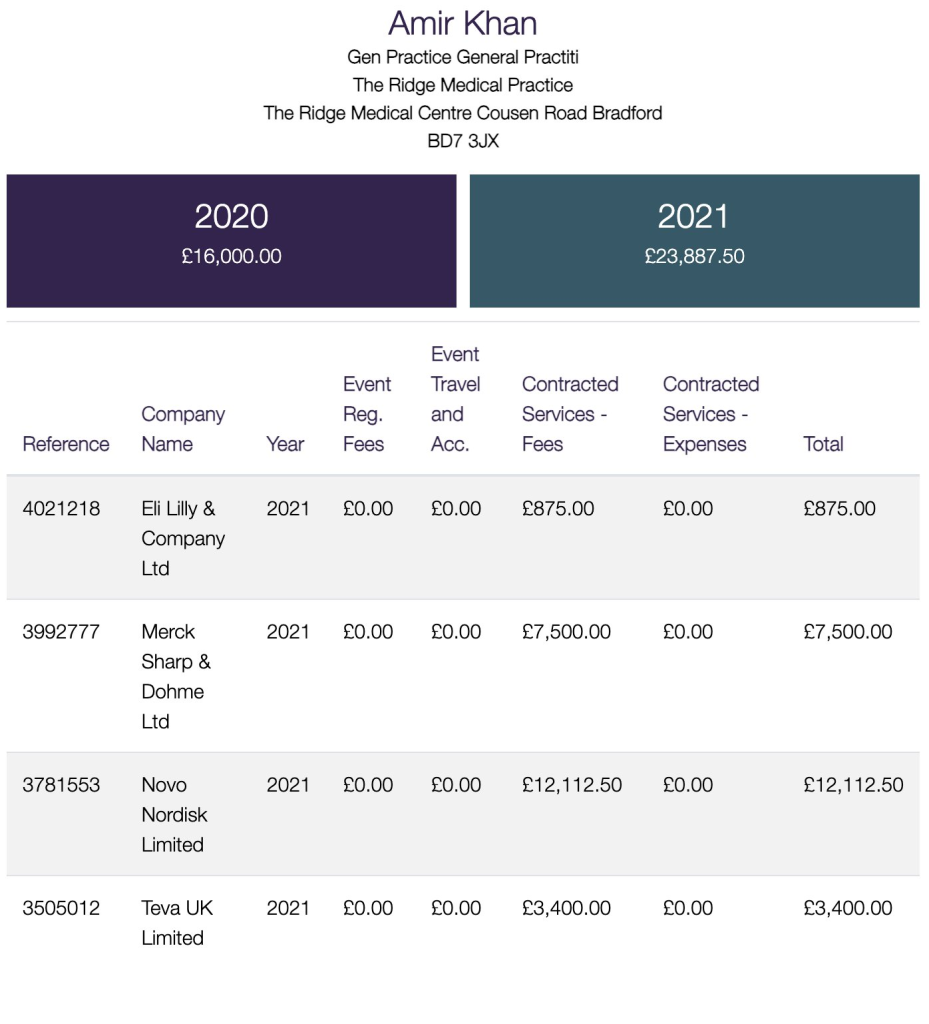
The cynical amongst our readers may question Dr Khan’s independence, given that he was in 2021 in receipt of over £12,000 from Novo Nordisk, the manufacturer of semaglutide.
As reported by the Daily Telegraph, Prof John Deanfield, who is also director of the National Institute of Cardiovascular Outcomes Research, said:
He would make “a clear case” to the Health Secretary about the benefits of a wide rollout of the jabs.
“The economics of this is very, very important,” he said, highlighting the potential to reduce taxpayer spending and boost the economy by preventing major diseases.
It follows research that shows obese workers are up to twice as likely to be off sick from work.
Around 8 million people in the UK have heart disease and a similar number take statins.
Prof Deanfield suggested around half of such patients could benefit from the jabs.
The “real excitement” about the findings was the way they showed that medicines that were designed to treat diabetes and obesity could prevent many killer diseases, he said.
Studies are now examining the impact of the jabs on a range of conditions including cancer, Alzheimer’s disease, multiple sclerosis and Parkinson’s disease.
“We are talking about cardiovascular disease but there are other diseases that might benefit from these drugs which are going to be equally exciting” with results on neurological conditions and kidney disease due soon, he said.
Yet a search of the ABPI disclosure log revealed that he too has been in receipt of cash from Novo Nordisk:

The fact is that we have been here before: a new wonder drug is claimed – by many who are in receipt of funding from the manufacturer – to have all sorts of benefits, it is announced in mainstream media accompanied with heady excitement; very little supportive data is available for proper scrutiny, and what studies are made public barely support the claims and are compatible with the opposite conclusions.
