But is more better?
Dr Ros Jones, HART member, retired Consultant Paediatrician, takes a look at trends in vaccination.
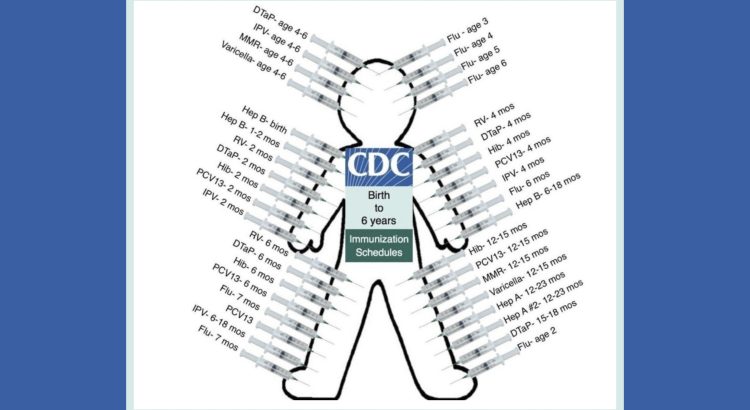
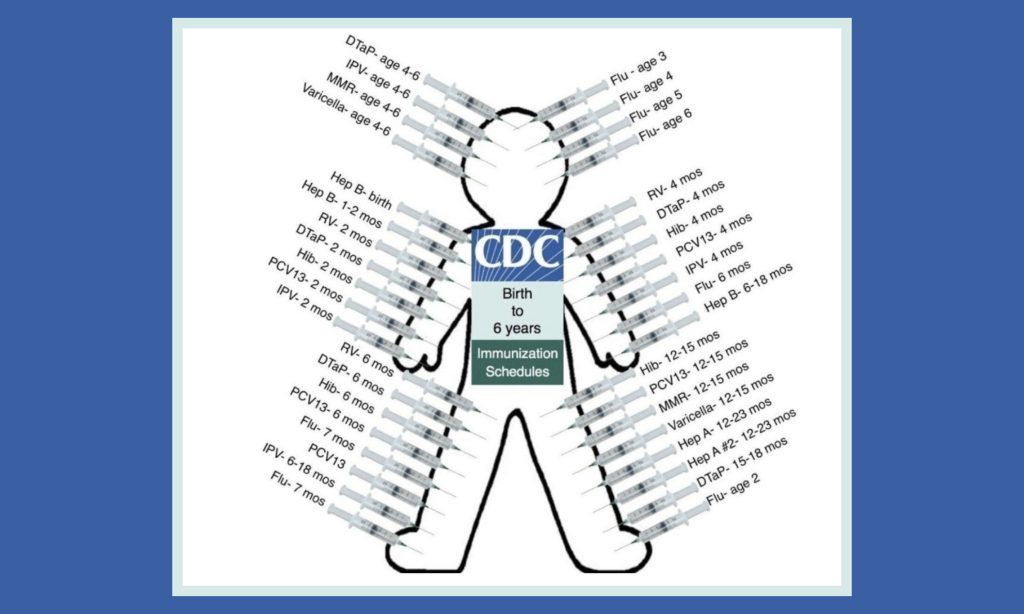
The picture above may shortly be out of date when the latest monoclonal antibody against respiratory syncytial virus (RSV) is added to the CDC list. The US approach stands in stark contrast to Europe’s.
So another dilemma for parents of young children who have already laboured long and hard over whether to give their children a covid-19 vaccine – will their children need this latest new immunisation?
An RSV vaccine developed in the 1960s got as far as human trials, but had to be hastily withdrawn when it became apparent that subsequent disease was far worse in the vaccinated than the controls. As expected, the babies made a good antibody response and there were no obvious serious side effects. Fast forward a few months to the next autumn’s RSV season and sadly for the drug company and even more sadly for the babies and their families, the vaccinated group developed much more severe disease than the controls (18/20 vaccinated infants hospitalised with 2 deaths versus 0 deaths and 1 hospitalisation in the 21 controls gives placebo efficacy of 100% against death and 95% against hospitalisation – wonderful stuff that normal saline!) Animal studies with the RSV vaccine had already highlighted such problems.
Similar difficulties were seen in candidate vaccines for SARS (SARS-CoV-1). No less than four new coronarvirus vaccines produced after the SARS outbreak in 2003 looked hopeful initially, until the animals were exposed to the SARS virus. Although the vaccinated animals cleared the virus more rapidly, they developed severe eosinophil infiltrates in their lungs, in contrast to the control animals, highly suggestive of an immune overreaction in the presence of the virus (a Th2 helper cell hypersensitisation).
Dengue vaccines have had similar problems, with Dengvaxia withdrawn after the vaccinated group experienced much more severe disease the following season. In that case, the vaccine had been rolled out widely in the Philippines without awaiting the one-year trial follow-up, in a moment of political hubris which resulted in their Minister of Health facing criminal charges, but far more seriously it also resulted in the deaths of at least 10 healthy children.
What all these disasters had in common was a condition called ADE (Antibody Dependent Enhancement). In the presence of a large immune response, inflammatory markers are activated; this led to acquired respiratory distress in the case of the SARS vaccine, severe wheezing and airway inflammation in the case of the RSV vaccine, and a severe systemic reaction with the Dengue vaccine.
So what of this latest RSV prophylactic? There are two types, firstly monoclonal antibodies which give so-called passive immunisation i.e. the infant is given injections of antibodies to protect them against RSV in the early months of life but these just disappear naturally. There is an existing drug called palivizumab which has been around since 1998, so it is not clear why they need the new one, nirsevimab. The main advantage of the new product is that it is given as a single dose, rather than the monthly injections recommended for palivizumab, which makes it more practical, hence the new version has been authorised for all infants, rather than the high risk groups only for whom the monthly palivizumab injections were recommended. Nirsevimab was approved for use in the EU and the UK last November, following trials involving 3580 treated infants. The report combines various studies – one involving only infants at high risk from RSV such as preterm babies or those with heart or lung disease, for whom there was a reduction in hospitalisation from 4.1% in the placebo group to 0.8% in the nirsevimab group. A second study then recruited healthy low risk babies and for them the reduction in hospitalisations was only from 1.6% to 0.6%. There was a reduction in overall infections, but it is not clear whether that means these infants will simply get RSV infection the following winter. Having said that, most hospitalisations for this condition are in infancy. But as so often, it seems that no longer-term outcomes are required for approval to be given.
Interestingly, the FDA have yet to approve it, although their advisory committee last month voted 21:0 to recommend it for all infants. A worrying observation in the FDA approval paperwork was an increase in all cause deaths in the nirsevimab arm of the various trials (12/3710 (0.32%) nirsevimab versus 4/1797 (0.22%) controls). I could find no mention of this on the European Medicines Agency or MHRA websites, although the same drug company results were submitted.
Meanwhile in April, the FDA approved a new RSV vaccine from GlaxoSmith Klein(GSK), Arexvy for use in over 60s, followed in May by approval of a similar Pfizer vaccine, Abrysvo. As with Covid-19 vaccines, Pfizer gave results as relative risk reductions, so an encouraging 66.7% efficacy, but much less impressive when looking at the absolute risk reduction of 0.24% (from 0.36% to 0.12%) for symptomatic lower respiratory tract infections. The number of hospitalisations was too small to look at efficacy. More worrying is that looking at the supporting information on the FDA website reveals both vaccines showing an increase in atrial fibrillation compared to the placebo and also neurological adverse events, namely Guillain-Barré syndrome and Acute Disseminated Encephalomyelitis (ADEM) in the vaccinated group, with one fatality and one woman requiring 6-months hospitalisation. In two of the studies, flu vaccine and the new RSV vaccine were given simultaneously making it impossible to know which of the vaccines to blame.
The Pfizer Abrysvo RSV vaccine is expected to be approved by the FDA in August for pregnant women, for whose infants there was a 0.8% reduction in hospital admissions for RSV infection over the following 6 months (from 1.3% to 0.5%). But the independent panel vote was not unanimous, and concerns were raised about an increase in preterm births. Indeed, the GSK RSV vaccine trial for use in pregnancy was already stopped for this reason. Because this is proposed for use in the mothers, it will need a large number to vaccinate to prevent one infant hospitalisation, given most babies don’t go anywhere near hospital for this condition. It is not at all clear whether those infants whose mothers have already been vaccinated, will also be offered the monoclonal antibody in a ‘belt-and-braces’ approach or whether the two different types of preventative are simply to provide a choice. GSK have specifically said that they do not anticipate their vaccine being used in infants: ‘evidence from an animal model strongly suggests that AREXVY would be unsafe in individuals younger than 2 years of age because of an increased risk of enhanced respiratory disease’ (remember the 1967 vaccine), whereas the Pfizer document only says of Abrysvo, ‘Pediatric studies should be delayed until additional safety or effectiveness data have been collected’.
It is noteworthy that approval for the vaccines has progressed via the FDA’s Priority Review mechanism – the excuse for Covid-19 vaccines was of course that there was an emergency due to a novel and deadly virus sweeping across the world, with a saviour vaccine the only way out of endless lockdowns. But what is the possible excuse for a priority vaccine for RSV? This virus was first isolated in 1956 and was presumably around long before that. But of course, if we’d been listening, we would have heard Sir Patrick Vallance in 2014 saying “In the future, medicines will come to market quicker with less data, with more research being conducted in the post-license phase”. It seems that the future has arrived.
The plethora of new vaccines in the pipeline, in particular mRNA vaccines which will be developed at the new UK government-funded Moderna facility in Oxford, must be subject to the proper scrutiny which has sadly been totally lacking in recent years.
This begs the question: what of the multitude of existing vaccines shown so graphically in the picture at the top of this article? It struck me that as a retired paediatrician in my seventies, now being labelled by the government as a conspiratorial ‘antivaxxer’, I had of course only had 2 vaccines in my infancy, smallpox and diphtheria. At age 7, I received the new polio vaccine and as a 13-year-old BCG against tuberculosis (and that only after a negative skin test showed I wasn’t already naturally immune). And that was it, until I reached medical school where I got the new tetanus vaccine. Yellow fever and Typhoid vaccines followed for a student elective in South Africa and then nothing until Hepatitis B vaccine 20 years later.
The generation below mine had only diphtheria, tetanus and polio in infancy with measles at 13 months. This UK timeline makes interesting reading. But my grandchildren’s generation are apparently offered 15 in their preschool years (many of course are combinations so an 8-week infant is now vaccinated against 8 different diseases simultaneously). But this is still well below the number offered (and indeed mandated for many schools) to American children. Perhaps the JCVI are full of ‘anti vaxxers’, let alone the Danish authorities where infants are only vaccinated against 6 diseases and with a much more spaced out programme at 3, 5 and 12 months.
Can anyone point me to the randomised trials showing that this huge sum total of vaccines is beneficial in terms of overall outcomes? Because I have failed to find it. Instead I have found interesting articles such as that from the Bandim project in Guinea Bissau, where the delayed introduction of childhood vaccinations in the 1970s gave a natural control group. In collaboration with the Statens Institute in Denmark, they found that killed vaccines were associated with an increase in childhood mortality. Or this one comparing the infant mortality of the healthiest 30 countries by number of vaccines given, which certainly showed no support for the idea that more is better.
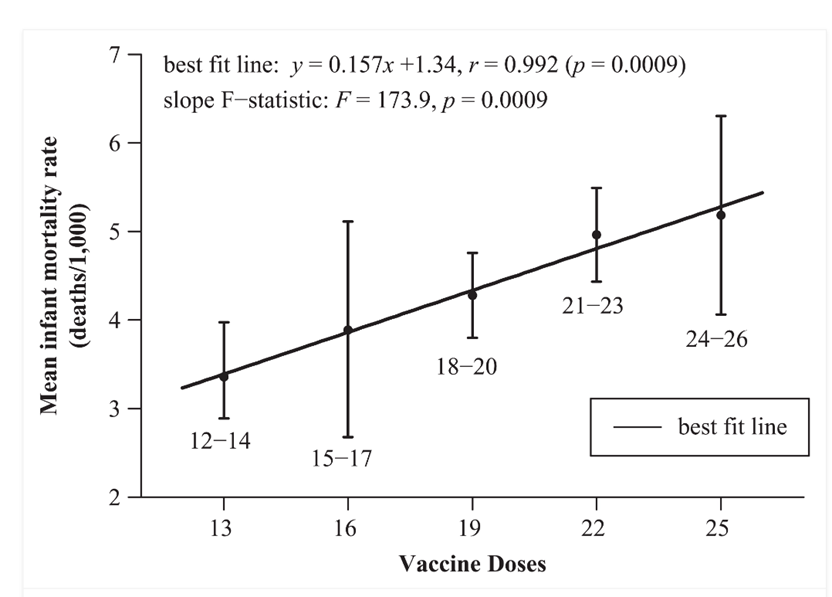
Figure 1: Mean infant mortality rates and mean number of vaccine doses 2009
Statements from WHO, BMGF etc that vaccination has been the biggest life-saving breakthrough does beg the question: if the same amount of money and effort had been put into ensuring every child had access to clean drinking water and adequate food (the most basic physiological need in Maslow’s hierarchy of needs), then how many more lives would have been saved?
Would ‘Big Plumbers’ now be dominating public health policy?
