

Might this have significantly biased outcomes reporting?
This article by Jonathan Engler, co-chair of HART, is reproduced from his Substack page
“A couple of months ago I reported on a paper by Martin Neil, Norman Fenton and Scott McLachlan in which they systematically analysed all the covid vaccine studies they could find and categorised them by the extent to which the authors had mis-categorised vaccinated subjects as unvaccinated, thereby massively biasing the results in favour of the vaccines.
“The extent and impact of vaccine status miscategorisation on covid-19 vaccine efficacy studies.” By Martin Neil, Norman Fenton and Scott McLachlan

During the “covid era” many studies have been published which make extraordinary claims for vaccine efficacy which are universally at odds with people’s personal experience. These are also contradicted by high-level data which shows more cases, hospitalisations and deaths after the vaccine rollout than before; for these to be happening mainly to the (rel… Read full story
They found this:
Every single study was subject to serious miscategorisation bias.
Bad enough as that seems, this may not be the worst of it.
This miscategorisation error on its own will introduce significant bias even if the vaccinated and unvaccinated receive the same standards of care.
But what if they didn’t receive the same standard of care?
What if the unvaccinated received treatments which worsened their outcomes? This would act synergistically with the above to bias the results even further.
Is this unthinkable? No, I don’t think it is, and I had always suspected that differential hospital treatment protocols might have been a factor in the adverse outcomes for the unvaccinated reported by many healthcare professionals after the covid vaccine rollout. [Any adverse outcomes were, of course, ruthlessly weoponised by the vaccine proponents and amplified across all mainstream media.]
It is important to realise that this would be the case whether or not this was the intended outcome, and herein I am not intending to make inferences in that regard. Suffice it to say that the covid era was characterised by a series of drivers which resulted in harmful things being done to many people. [See this piece for a commentary on how HCWs can easily be manipulated by circumstance – either deliberately or not – into doing bad things while thinking they are acting virtuously]
We have already seen that certain policies which turned out to be extremely harmful – for example “shielding” – were applied to people who were perceived to be “more vulnerable”.
It is therefore not beyond the bounds of possibility that the unvaccinated too were also treated as “more vulnerable” and marked for “special treatment”. How confident can we be that such treatments were beneficial, rather than harmful? Based on everything else recommended (or mandated or coerced) during the covid era, not very.
Is there any evidence of this?
Yes, there is.
Robert Kogon has sent me links to several tweets, which can be found here, here and here and I said I’d amplify these by way of a short substack piece (which has become a lot longer than I intended). Be sure to read the entire threads in the case of the first two of these.
- The first tweet thread shows that from at least June 2022 in official WHO guidance “Clinical management of COVID-19” lack of vaccination was regarded as a factor increasing the risk of severe disease.


The document is clear that “treatment selection is determined by disease severity and risk factors”. (My emphasis.)
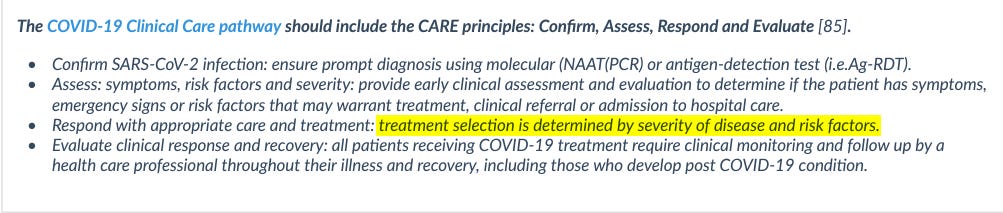
The link in that section to the “COVID-19 Clinical care pathway” leads to a document containing this guidance:
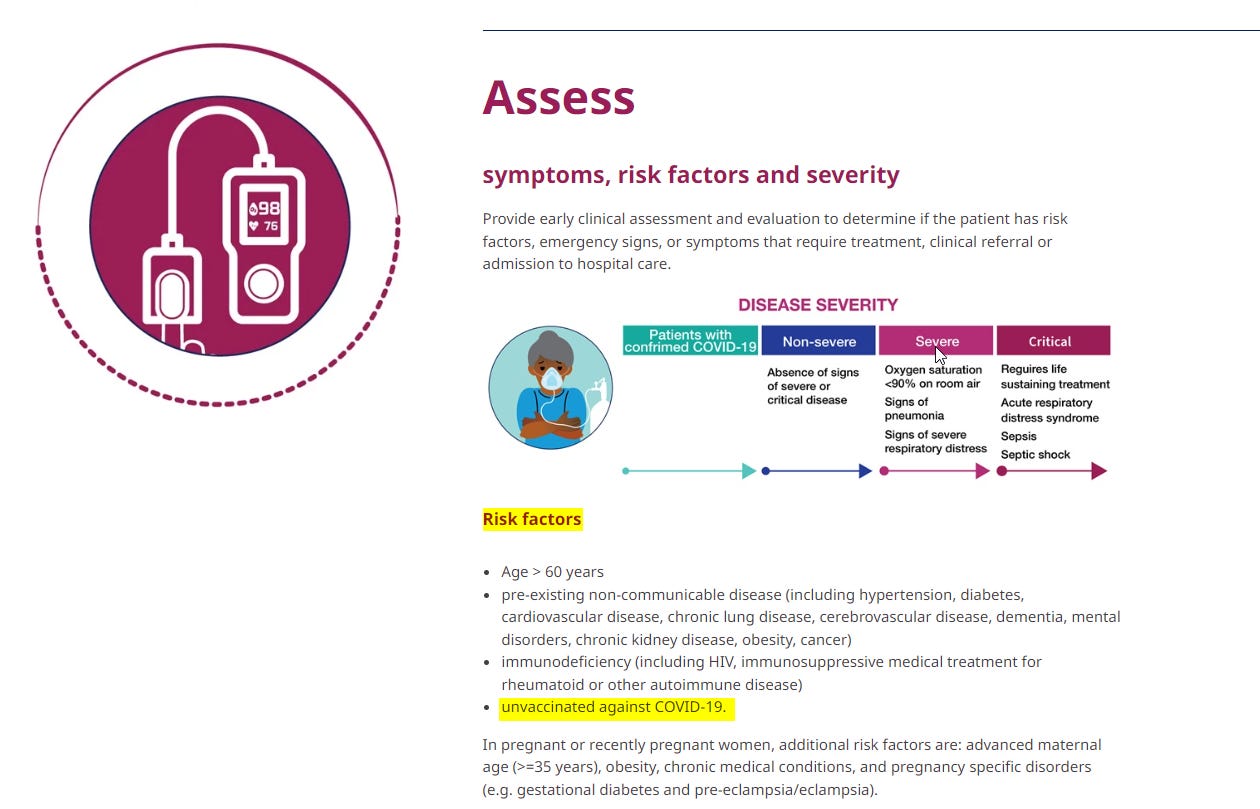
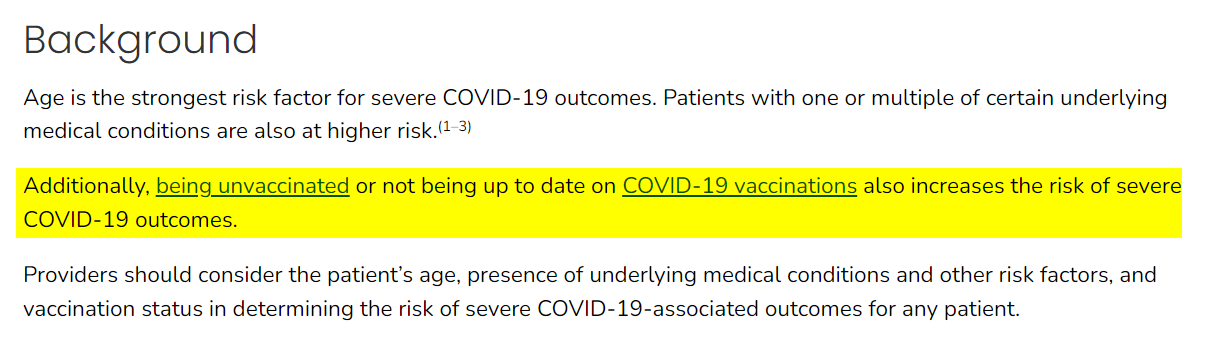
Firstly, being unvaccinated is reiterated as a risk factor for severe disease:
Secondly, under the “respond” section:

Note the disparity here:
- For mild / moderate disease with no risk factors: supportive care at home
- For the same mild / moderate disease WITH risk factors: consider Nimatrelvir/ritonavir (oral) (aka Paxlovid), Molnupiravir (oral) or Remdesivir (intravenous).
You don’t need to be a genius to realise that a decision to give an intravenous drug would ordinarily mean hospital admission.
- The second tweet thread (by Josh Walkos) is centred on illustrating some of the financial drivers towards certain treatment choices, which – though undoubtedly a huge factor – I won’t expand on here as this article is more focussed on evidence for differential treatment policies.
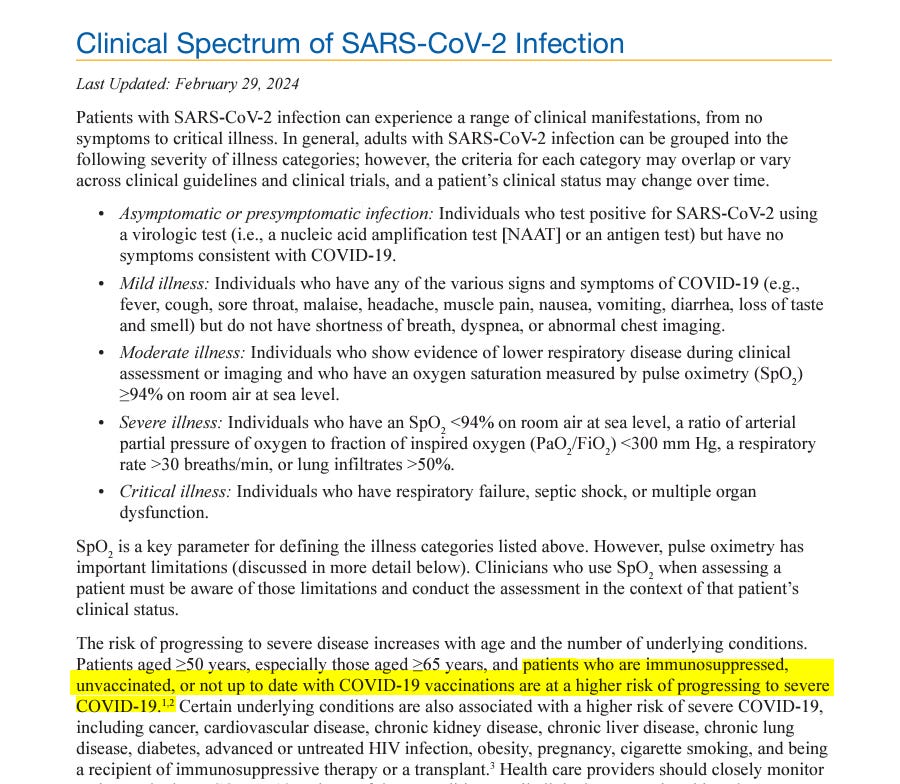
This NIH document contains the following section:
Under the section describing Therapeutic Management:
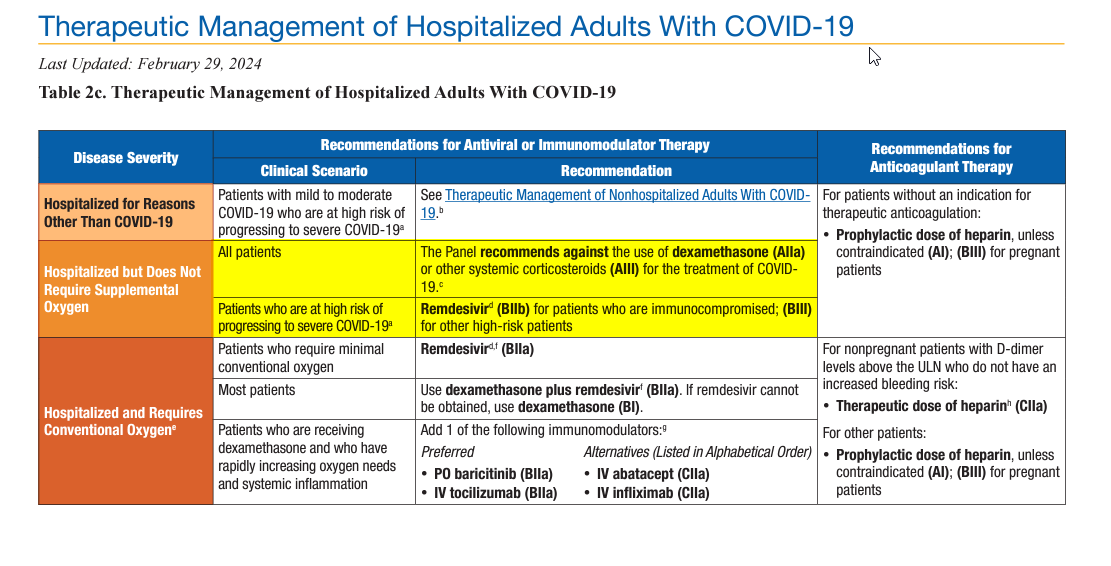
The same disparity as above is evident here. For patients “In hospital but supplemental oxygen not required” (so those with mild illness):
- All patients – even dexamethasone not recommended
- Patients at high risk of progressing to severe disease – Remdesivir for immunocompromised and “other high-risk patients” (ie the unvaccinated).
This CDC guidance “Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals” reiterates the above:
- The third tweet refers to the below extract of this document describing Covid-19 treatments from authorities in the Canadian Province of Saskatchewan:
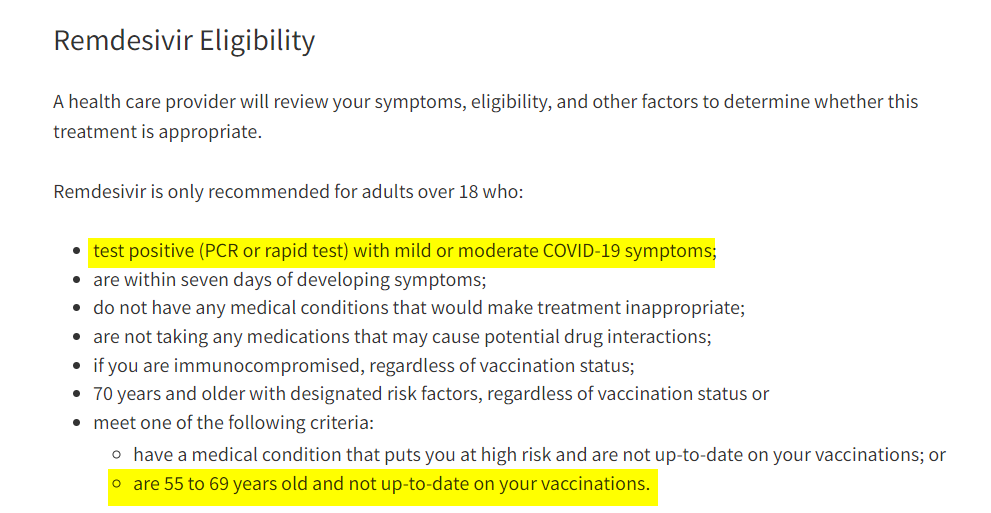
Whilst this is expressed in exclusionary terms (“Remdesivir is ONLY recommended for…”) it seems clear that the implication is that it should be considered for healthy 55 to 69 year olds with mild symptoms.
Evidence from Australia is even more damning.
The anonymous blogger known as Jikkyleaks uncovered some further detail about Australia – see this thread.
In the above tweet Jikky gives a link to a document which no longer works, but I found it on wayback machine here.
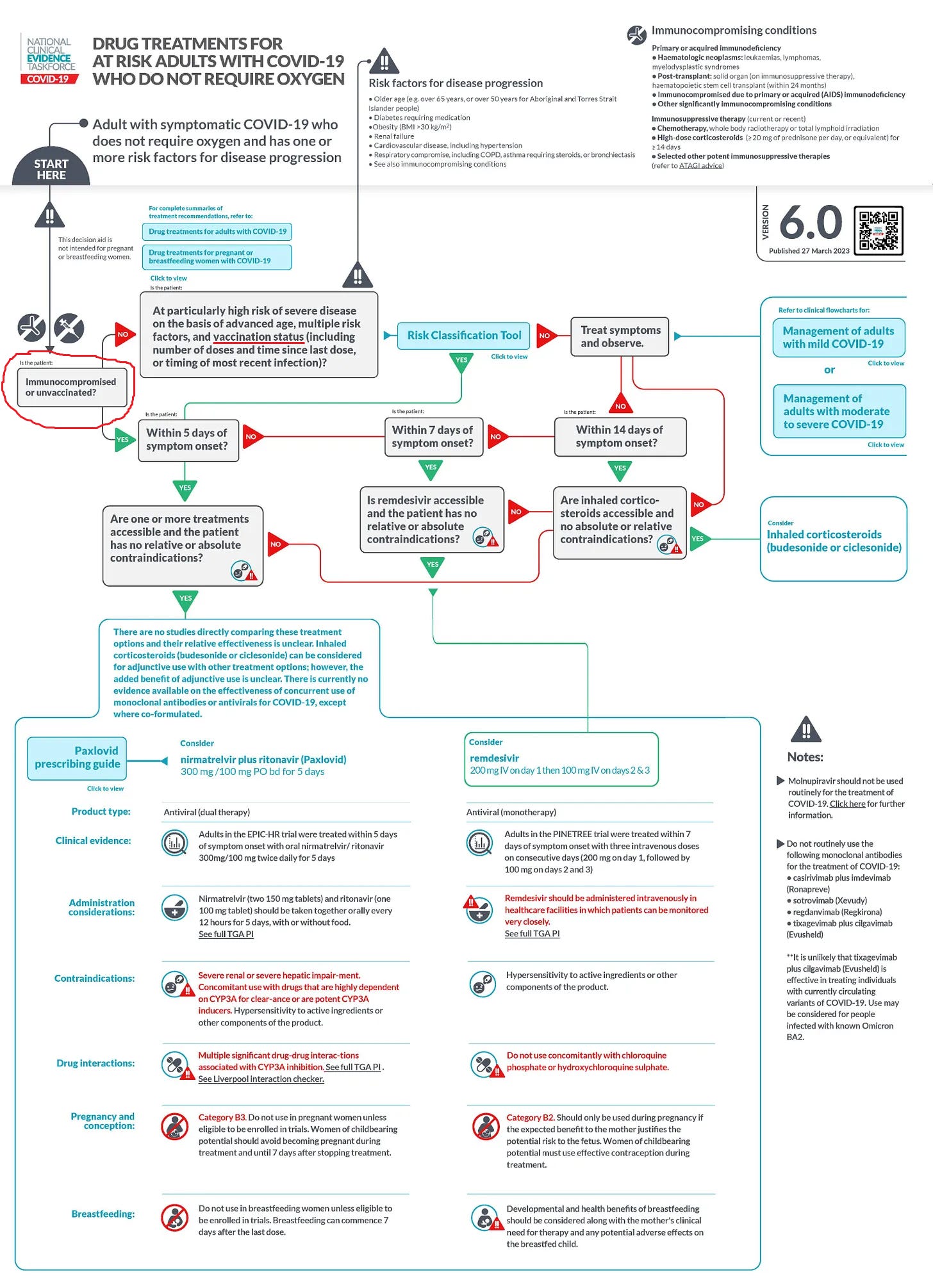
If you follow the chart from my red annotations, again it is clear that vaccination status is key to risk assessment:
- low risk is associated with symptomatic treatment / observation
- for higher risk (including being unvaccinated) Paxlovid is recommended if within 5 days of symptom onset together with Remdesivir if within 7 days.
Incidentally, the domain clinicalevidence.net.au (the source of the above protocol) is no longer active, having been merged with another here, but from the Wayback machine we can see that this is an official Australian Government website:
The stated objective of this site is:
The National Clinical Evidence Taskforce is a multi-disciplinary collaboration of 35 member organisations – Australia’s medical colleges and peak health organisations – who share a commitment to provide national evidence-based treatment guidelines for urgent and emerging diseases.
This pioneering alliance established the world’s first ‘living guidelines’ for the care of people with COVID-19 and the scope has now expanded to include MPX.
The Taskforce undertakes continuous evidence surveillance to identify and rapidly synthesise emerging research to develop and update recommendations to ensure Australian clinicians are up-to-date with the latest advice.
Other factors to consider.
In considering the extent to which the above might be relevant in what patients actually received, I would make the following points:
- Doctors have become extremely protocol-driven as a result of the threat of litigation and the general “dumbing down” of medical education. It is safer and faster to look at a flowchart than to apply critical thinking. So yes, I would expect these protocols to have been followed
- These protocols likely reflected the “zeitgeist” so even where not reduced to documentary form I would have expected these to have been the principles upon which doctors decided on treatment options.
- The covid era was in general terms characterised by a lockstep and centralised approach to treatment so, even though the above represent just a few documents out of many thousands which must be in existence I would be very surprised if the others said anything which differed from those.
- Fear was a heavily motivating factor in respect of healthcare workers. It was believed that “covid positive” patients were dangerous bioweapons to be avoided. It was even believed that “viral load” was higher in the unvaccinated and hence the unvaccinated posed more of a danger, in which case there would have been a greater propensity to treat vigorously, especially using ventilation, believed to protect healthcare workers from aerosolisation of virus particles. [See here for a discussion about the role of ventilation as an accomplice in cases of hospital-acquired pneumonia.]
- If the unvaccinated received treatments which were ultimately harmful, on seeing this in front of their eyes the delusional belief systems in operation during the covid era would (in my view) not have led doctors to ask the rational question: “might these treatments actually be harmful?”.
Instead, the “lessons learned” would have been: “look how badly the unvaccinated are doing” and “we need to be even more aggressive in our treatment of the unvaccinated”.
Thereby, a ghastly feedback loop would have ensued.
Come to think of it, there have been a lot of ghastly feedback loops involved during the covid era, most of them involving fear in one form or another.
As Vinay Prasad said:
“It is a unique situation in medicine. In our whole medical career, doctors have never been personally afraid the way they were [with covid].”

