Vaccine passports: the debate
Parliament is due to debate vaccine passports on 15th March, triggered by an online petition. After consideration of the arguments for and against below, HART strongly contends that any vaccine certification or passport would create a precedent of eroding informed consent. An independent group, the UK Medical Freedom Alliance, has prepared a detailed open letter on the topic, which is well worth reading.
| For | Against |
| – The vaccine is the way out of lockdowns. – Other countries might do it and it will be the only way to restart the tourist industry. – The hospitality industry and performing arts could quickly abandon social distancing which has such an impact on profit margins and business viability. – It is necessary, in case unvaccinated people cause asymptomatic transmission. | – The vaccine rollout to all vulnerable groups has been very efficient. These groups account for 99% of those at risk of dying, thus transmission by younger unvaccinated people becomes irrelevant. – Although 30% of people testing positive for SARS-CoV-2 may be asymptomatic, that does not mean that 30% of transmission comes from this group. Proven asymptomatic transfer is very rare. – The UK has a strong record of public health measures by consent; vaccination has never been mandatory. – Vaccine passports would have a coercive effect on informed consent which is contrary to UNESCO’s “Universal Declaration on Bioethics and Human Rights” (2005). – Any inducement is especially inappropriate given these vaccines are still in a period of temporary licence pending publication of long-term safety data. – Vaccine passports would create a two-tier society, in which those who remain unvaccinated for whatever reason are deprived of their basic freedoms of travel, association and employment. – The WHO does not support vaccine passports. – The flu vaccine is given to high risk members of society and those who choose not to have it do not suffer any restrictions. Given COVID-19 is now endemic, the vaccination programme should follow this previously well-established protocol. |
Variants no cause for concern
Variants arise spontaneously due to the error-prone replication of SARS-CoV-2. Compared with influenza, however, the rate of variation is slow. Despite the exaggerated news on this front, in over a year, the most-changed variant (Brazilian P1) of SARS-CoV-2 is just 0.2% different from the Wuhan sequence. So far, none of the observed differences in any variant has been particularly important functionally, with the expected trend towards modestly increased ease of transmission. Reassuringly, it has recently been shown that the vaccinated and those recovering from natural infection all possess a broad repertoire of T-cell responses entirely capable of recognising all the most noted variants. As mentioned before, immune escape is considered by the most qualified immunologists to be implausible. We are therefore perplexed by the concept of ‘Red List Countries’ and border restrictions. It is simply not true that variants are more likely to arise in unvaccinated people. It is an immunologically unsound concept and arguably the converse is more likely.
Back to school
As we reported last week, after conducting 1.9 million tests in secondary schools throughout January and February, the results have shown no genuine COVID-19. Given that the children attending schools in those months were mostly the children of key workers and therefore most at risk of COVID-19, this is a wonderful result that should be celebrated.
Despite having established that there is no COVID-19 in the asymptomatic (or healthy) school population, we are about to embark on mass testing. Even if the positive rate stays at the current record-breaking low there will be tens of thousands of false positive results before Easter, resulting in more education being missed. All mass testing (such as cancer screening), treats the initial result as an indication of a higher risk of diagnosis. Only a confirmatory test can make the diagnosis. By ignoring this basic principle the Government risks undermining faith in their ability to correctly diagnose COVID-19.
Even though we have both low prevalence and mass testing, most children are now having to wear masks. Boris Johnson called this approach “nonsensical” in August. Masks have been introduced without assessment of the potential harms they cause nor any evidence that they have a benefit. The UsforThem open letter opposing mask wearing in schools has attracted support from hundreds of professionals.
Children have been disproportionately affected with the sacrifices of lockdown resulting in an epidemic of mental health issues. Gavin Williamson has promised no child’s prospects should be “blighted by the pandemic”. Consequently there are plans to address academic achievement. However, there is a failure to understand that academic success will be severely hampered for those struggling with mental health problems and for many children these need to be addressed before efforts at catching up academically will succeed.
US states are opening up
The situation in the USA is changing rapidly. North and South Dakota are well matched across many key metrics so make an ideal comparison. Neither state instituted spring lockdowns, but, in November, in response to rising case numbers, North Dakota imposed stringent policies of mandatory face covering and lockdowns, whereas South Dakota did not. No difference in case counts was observed.
Initially, Florida followed the established policy line. Later, however, as reported here, Gov. Ron DeSantis shifted policy towards focused protection of the vulnerable, while allowing the remainder of society to continue living life near to normal. The disaster predicted by many advocating lockdowns did not come to pass. In fact, the opposite happened. Florida has had a lower age-adjusted mortality than most other states, yet the economy and tourism are in comparatively good shape. COVID-19 deaths per million are, in fact, similar to California’s, which has instituted one of the toughest lockdown and mask mandate regimes in the US.
Over the past week Texas, Mississippi, Tennessee, West Virginia, Arizona, Wyoming and Connecticut have also announced the restoration of freedoms to their citizens, either by ending mask mandates, reducing restrictions on business, or both. This is despite having a vaccination program dramatically behind the UK’s in terms of percentage vaccinated.
Covert ‘nudges’ – is it ethical?
Throughout the pandemic, the Government’s behavioural scientists have used covert psychological strategies – ‘nudges’ – as an effective way of increasing compliance with restrictions. Several interventions of this type have been woven into the intensive communication campaign, including: fear (strategically inflating perceived threat levels); shaming (framing compliance as akin to being a virtuous person); and peer pressure (portraying non-compliers as a deviant minority). Contrary to the traditional tools of persuasion, such as information provision and rational argument, these ‘nudges’ largely work subconsciously and raise important ethical questions.
The same covert strategies are now being used to promote the uptake of COVID-19 vaccines. A recent NHS England document recommends, for example, that healthcare staff “leverage anticipated regret” on the over-65s by asking them “how will you feel if you do not get vaccinated and end up with COVID-19?”. For young people, who are at vanishingly small risk of suffering serious illness, one recommendation is that they should be told “normality can only return, for you and others, with your vaccination”. Obtaining informed consent before administering an intervention should be a vital part of medical practice. To ensure ethical integrity, healthcare staff should be encouraging each individual to, consciously and rationally, weigh up the pros and cons to themselves of accepting a vaccine rather than covertly “nudging” them towards compliance.
The ethical dilemmas of using covert methods have long been recognised; in 2010, prominent figures in the discipline stated (pg 74), “Policy makers wishing to use these tools… need the approval of the public to do so”. No such consent has been sought or granted. HART believes that an open debate about the ethical integrity of these approaches, and the collateral damage associated with them, is now urgently required.
Quicker reopening could help boost vaccine immunity
This winter, levels of many common seasonal infections – such as flu – remain extremely low due to a combination of lockdown measures, reduced global travel and high flu vaccination uptake. HART scientists are concerned that this may result in waning immunity to flu and other respiratory pathogens, following a year where the population has had very little exposure. Evidence for this is already emerging in Australia, where a sharp increase in Respiratory Syncytial Virus infections in young children has been observed at an unusual time of year. A child’s immune system is not fully developed until the age of 6-7 years old, and exposure to pathogens during those early years helps shape an individual’s ability to deal with common pathogens circulating within the population. HART’s view is that this demonstrates yet another potential harm of prolonged lockdowns and social distancing measures that has not been properly evaluated. The longer populations remain unexposed to common pathogens, the greater the risk this poses.
It is worth noting that as vulnerable groups are vaccinated against COVID-19, opening up society swiftly would allow natural boosting of vaccine-induced immunity at a point when the population is most protected. The vulnerable will thereby be exposed at a point when their antibody levels are highest and they are best able to defend themselves, and their immunity will be strengthened by this exposure.
Being overly cautious in lifting lockdown is not a cost-free option, and risks not building on the advantages that have been gained by the rapid rollout of vaccines. We could end up in a vicious circle of reduced immunity caused by lockdowns leading to worse respiratory illness and deaths the next season, with calls for more lockdowns to deal with the resulting healthcare crisis. Now is the time to open up society, to prevent this decline in public health and immunity.
And some good news…
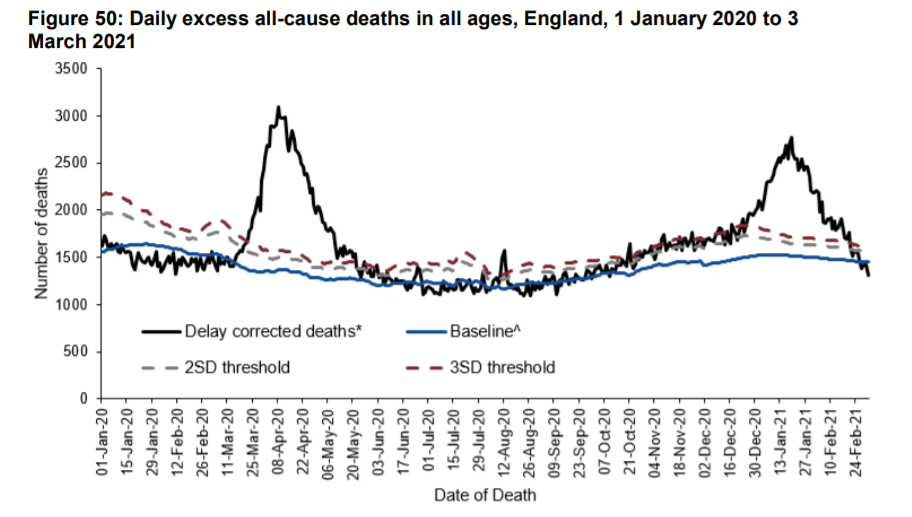
All measures of COVID-19 prevalence and harm are currently low and falling. The most important measure, excess deaths, now shows that deaths are below normal levels for the time of year. As there is a 23 day window between contracting infection and death, this shows that transmission levels have been essentially zero for nearly a month now.