Mass testing in schools
From next week, secondary pupils across England will be asked to take rapid lateral flow tests to help identify anyone who might be infectious. According to PHE and the University of Oxford, lateral flow tests have a false positive rate of around 0.3%, which in a clinical setting would be acceptable, but when testing 4 million healthy, asymptomatic schoolchildren twice a week will mean 24,000 false positive tests. When you add in their contacts this could see up to 700,000 children out of the classroom every week (based on classes in quarantine rather than whole year groups). This clearly undermines the “national priority” of ensuring British schoolchildren have the education that they deserve. It is also important to note that after conducting 1.9 million tests in secondary schools throughout January and February, the results have shown no genuine COVID-19.
UK’s data is progressing faster than the ‘Road Map’
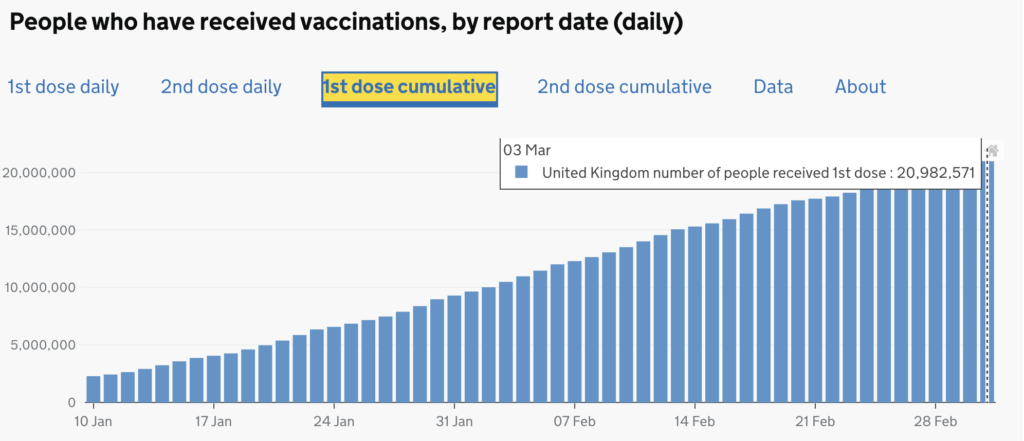
Vaccination proceeds at pace, with the UK the second most prolific vaccinator worldwide behind Israel. Over 20 million people have now had their first dose and everyone in the first four priority groups – those aged 70 and over, care home residents, healthcare workers and people required to shield – were offered a jab by mid-February. The foresight in securing supplies from multiple manufacturers appears to be paying off and may enable the UK to assist other countries once our greatest priorities have been met. Regardless of the inconclusive debates about why it is happening, the following numbers continue to fall and are to be celebrated:
| Numbers | % reduction over last 7 days | |
| Cases | 6573 (as of 4 March) | -34.4% |
| Hospitalisations | 757 (as of 28 Feb) | -29% |
| Deaths | 242 (as of 4 March) | -33.6% |
Do COVID-19 restrictions work?
When the relationship between lockdown stringency (as measured by Oxford University Blavatnik School’s index) and COVID-19 deaths (from Worldometer) is examined, there is a striking lack of any suggestion whatsoever that the more severe the lockdown, the lower the COVID-19 mortality, and in fact, if anything, the data suggests the opposite may be true. This is also apparent from studies in the USA which have shown that COVID-19 mortality is not linked to lockdown stringency (or mask usage).
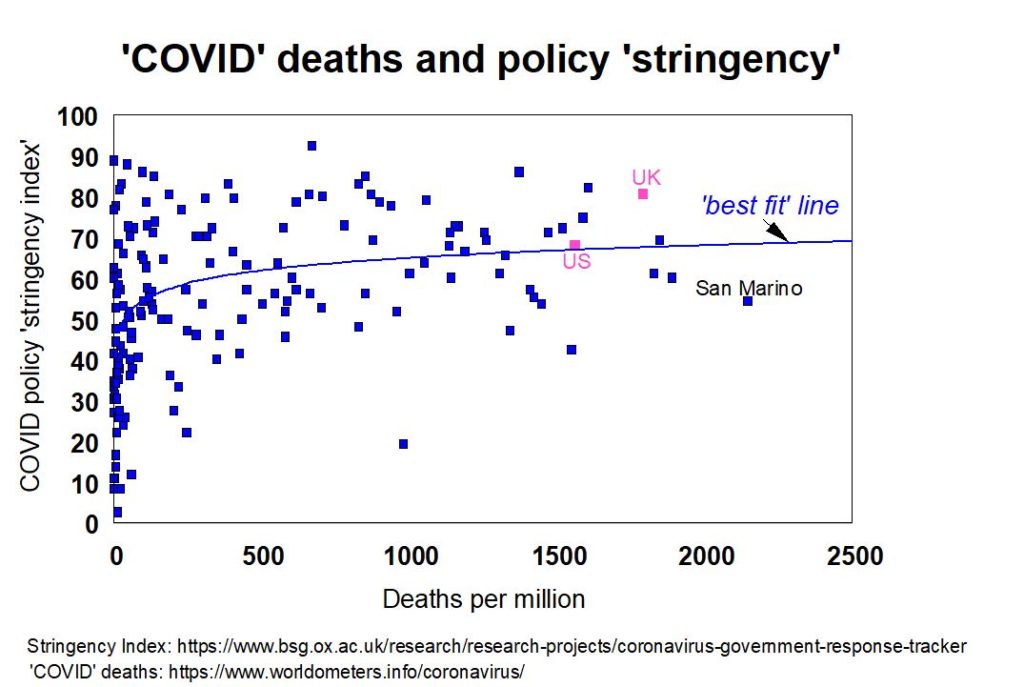
This should be investigated as a priority, because the costs of lockdown are truly large, in every possible dimension. A number of groups have, throughout the pandemic, estimated that the negative impacts of lockdown have or will exceed the anticipated lives saved or deaths delayed – read more here.
Modelled predictions by definition rely on assumptions and these assumptions might be wrong. Only by correcting models in light of real life data can errors be avoided. Real world data should always trump modelled data as it is not based on potentially false assumptions. Instead, the modelers appear to have “doubled down” on their position, creating ever more frightening projections which have never actually come to pass, but which have been used to frighten the population into compliance with the restrictions.
There have not been many assessments of whether the theoretical expectations of lockdown match up with the reality and accordingly, a member of HART recently published this review in The Critic which was endorsed by a member of NERVTAG. In brief, it is conceivable that, by altering the evolutionary pressures on the virus, our measures may inadvertently be making the situation worse.
Avoiding harm to children
As it stands, COVID-19 vaccines will not be offered to children and indeed all the original trials specifically excluded them. It is worth noting that phase 3 of the vaccine trials to establish long-term safety data are on-going and not due to conclude until late 2022/early 2023. It is concerning to hear scientists continue to call for COVID-19 vaccines to be rolled out to this age group. Some have expressed concerns that a very small number of children may develop ‘long Covid’, a post-viral syndrome; however given the unknown risks of adverse events from blanket vaccination, this is not a reason to proceed. None of the trials have specifically looked at whether the vaccines could reduce ‘long Covid’ – so this is a hypothesis that must first be investigated and substantiated.
Any suggestion that children should be vaccinated to prevent spread to older people is surely questionable on two grounds: (1) the ethics of children having an unknown long-term risk imposed on them for no matching benefit – given their extremely low COVID-19 risks – and (2) if vaccination is available for those vulnerable persons who desire it, such a need is surely absent. We encourage you to read this fully-referenced letter on the ethical concerns over COVID-19 vaccine use in children.
Assessing asymptomatic transmission’s role in the pandemic
As SARS-CoV-2 is transmitted from person to person, measures intended to reduce the number of daily contacts for each person should reduce transmission and ultimately deaths – as concluded in this Imperial College London paper. However, the underlying assumption is that all contacts are approximately of equal weight in terms of the probability of infecting others and that the prevalence of the infected individuals are similar, wherever one looks.
Prior to 2020 the default assumption was that only symptomatic individuals are at high risk of infecting others with a respiratory pathogen, as droplet secretion expulsion is the major mode of transmission. Early in the COVID-19 pandemic however, based on very limited evidence (a mere 6 case studies involving just 7 people), it was claimed that asymptomatic transmission was a very important driver of the pandemic (although Dr. Maria Van Kerkhove of the WHO is quoted as saying it is ‘very rare’). The entire rationale for mask wearing and mass testing is based on the assumption of the importance of asymptomatic transmission being correct. However, when the source data was reviewed this assumption was called into question. Empirical data show that transmission risk is very variable and is much greater in those displaying symptoms than from those who test positive for the virus, yet show no symptoms. For example, in this household infection survey, those with symptoms had a surprisingly low transmission rate of 17% probability of infecting another householder while those who had not yet developed symptoms led to another householder turning positive in just 0.7% of cases.
By contrast, it is clear that a high proportion of infections have been acquired in institutions.In spring 2020, up to 40% of infections were hospital acquired (which are attended by large numbers of people, even in lockdowns) and 40% of deaths were in care homes. It seems plausible therefore that COVID-19 may be well on its way to becoming predominantly a disease of institutional spread, as was the case with prior novel coronaviruses. HART recommends urgently undertaking a detailed, multi-disciplinary review of the effectiveness of non-pharmaceutical interventions in community and institutional settings.
SARS-CoV-2 or COVID-19?
It is very important to avoid conflating the virus and the disease. SARS CoV-2 is a respiratory virus. If you contract that virus, you will likely have mild symptoms. In rarer cases, SARS CoV-2 can lead to a more severe collection of symptoms, characterising a disease we call COVID-19. This is not a problem of semantics, it is a public mental health issue. By referring to the virus and the disease interchangeably, we end up with unnecessary panic. Headlines where experts describe COVID-19 as “the worst illness I’ve ever had” do not sit well alongside announcements that imply “60,000 people [are] catching Covid each day”. By failing to grasp the difference between the disease (severe illness) and the virus (usually mild or no symptoms) the public are inferring an exaggerated risk to their own health, resulting in increased anxiety and widespread fear of germs that could have long-term implications for mental health.
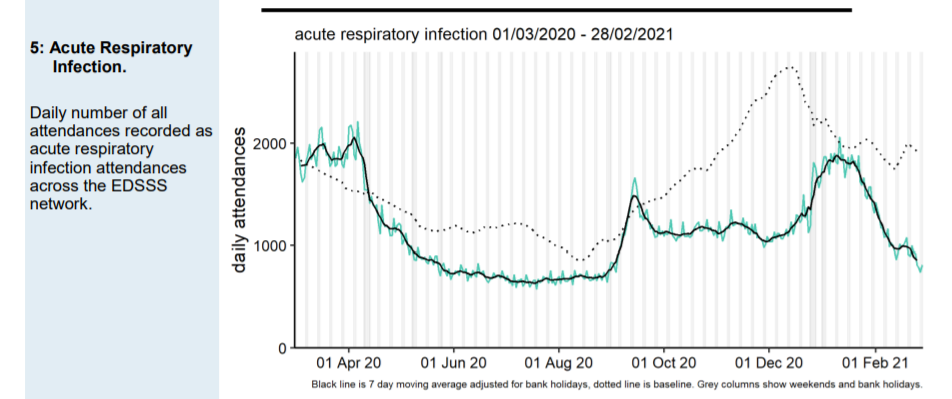
More good news from the NHS
Not only are suspected COVID-19 attendances continuing to decrease nationally and across all age groups and regions, but people coming to A&E with an acute respiratory infection is almost as low as the summer minimum and well below normal for the time of year. This would suggest that any pressure the NHS is experiencing is not related to community spread of SARS-CoV-2.