Many of you found our first bulletin last week useful. We are pleased to circulate our second bulletin below.
COVID-19 in context
With every death comes personal tragedy, nevertheless it is important to remember:
– The median age of at death with COVID-19 (around 82 years) exceeds normal life expectancy.
– The majority of those who died with the virus also had two or more serious, chronic illnesses.
– In 2020, there were 388 COVID-19 deaths in those aged 60 and under with no prior illnesses.
– 99.9% of people under 70 years and with no underlying conditions survive the virus.
Already, all those in the first four groups of the vaccine rollout strategy (70+ and those considered clinically extremely vulnerable) have received at least one dose. Meanwhile, the numbers of daily deaths and the number of people severely ill in hospital continue to fall steadily. This is extremely encouraging.
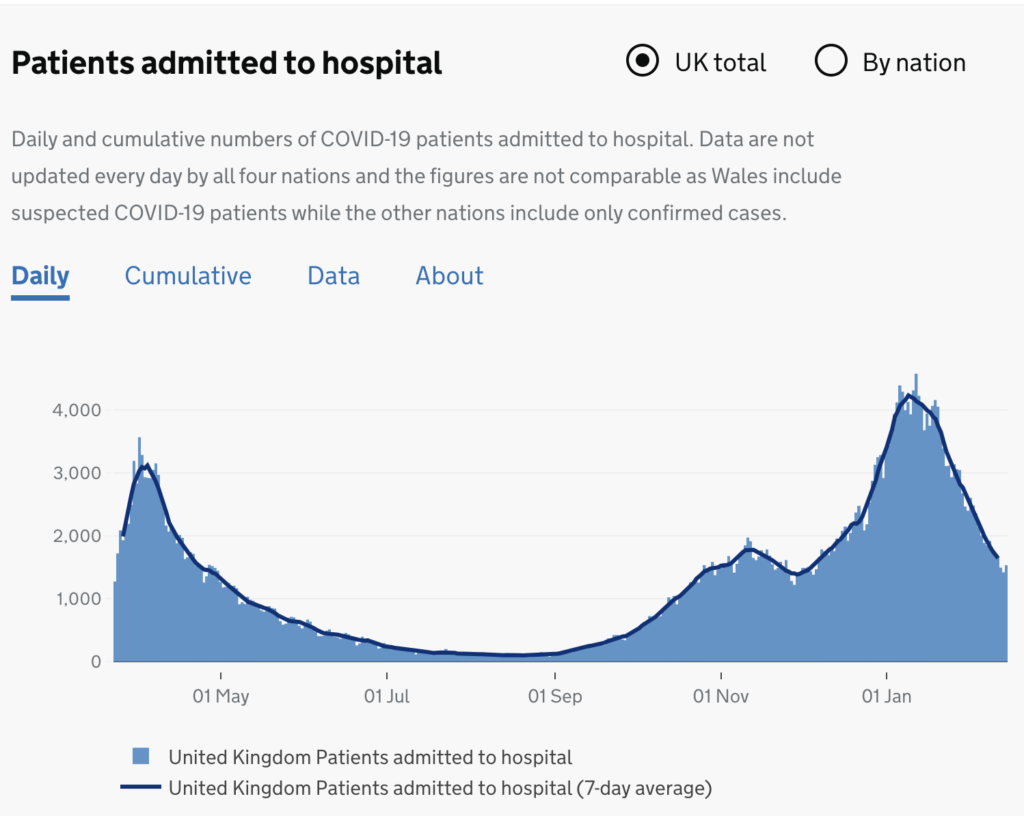
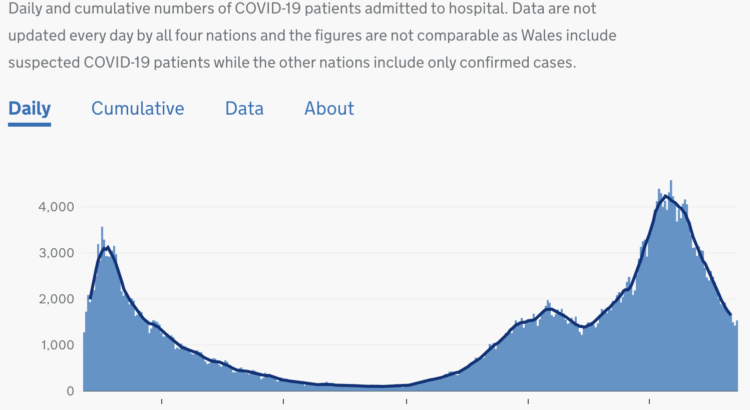
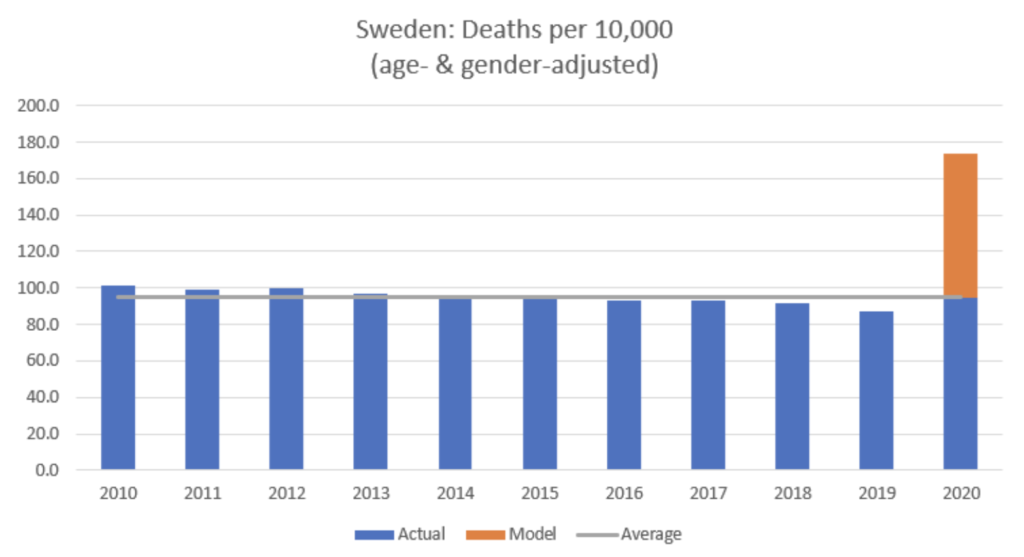
| It should also be noted that we have never previously counted deaths from a respiratory pathogen, season after season, as HART summarised here. This analysis provides useful context within which to assess the current situation. Unemployment rises, GDP falls Devastating economic impacts are now manifest, with unemployment rising to a 4-year high of 5% in January, while GDP in 2020 fell by 10%, the biggest recorded drop in history. Sweden by comparison with similar infections but few restrictions experienced a reduction in GDP of just 2.6%, lower than the EU average of 4.8%. While pandemic and lockdown impact is difficult to disentangle, the evidence would point to the economic restrictions being untenable going forwards. Rising debt, poor growth and a smaller economy (lower GDP) will jeopardise the country’s ability to care for its residents in the future, with less financial resources available for the NHS and all services. It seems likely that the restrictions will result in large parts of the hospitality, travel, tourism, events and arts sectors no longer being viable. Hospitality alone was responsible for over 3 million jobs in the UK before the pandemic. In 2020, sales in the sector were down by 54%, equivalent to £72 billion. The structural damage caused by the restrictions to these key sectors will have consequences for years to come. Evidence for increased psychiatric morbidity A year of COVID-19 restrictions has led to unprecedented levels of loneliness, fear and uncertainty about the future. This impacts on us all, causing an escalating risk of suicidal crises. A survey in July 2020 found that 1 in 6 children were exhibiting a significant mental health problem, many for the first time. By winter, 1 in 4 young people felt unable to cope. Adults of all ages suffered a substantial rise in anxiety and depression during the first lockdown, and almost 1 in 3 people have increased their alcohol intake. Loneliness is likely to have evoked mental defeat in elderly people with dementia, often resulting in premature death. This month, further evidence of the mental health costs of restrictions has emerged with reports of significantly increased anxiety and depression in postnatal mothers and a rise in disabling tic disorders in children. Due to the psychological characteristics underpinning their difficulties, people already struggling with these particular mental health problems may suffer the most: obsessive-compulsive anxiety, fuelled by inflated concerns about contamination and the protection of others; panic attacks, often driven by recurrent thoughts of imminent death; generalised anxiety, involving excessive worrying about future threats; depressed mood, maintained by negative thoughts about the future.The psychological impact of constant testing is also something that needs to be urgently investigated, as there are likely to be repercussions for all, especially those prone to health anxiety. COVID-19 in hospitals and care homes The low prevalence of the virus in the community and the increasing levels of immunity in the population means this virus is becoming mostly a problem in hospitals and care homes. HART believes it is crucial to take account of this insight in managing the residual cases. When the R-value is estimated, it is not a quantity that’s measured directly, but inferred from the total number of cases, whether they arise in the community or within institutions. With the latter playing a dominant role, it now seems needlessly destructive to maintain restrictions in the community. It has been estimated that up to 40% of infections in the spring 2020 peak were acquired in hospitals and that 39.3% of the COVID-19 deaths in spring 2020 were from care homes. It has been estimated that, during the growth phase of an outbreak, the R number in hospitals may have been as high as 14. Yet decisions have been made to close schools based on a potential reduction in R of 0.2 or less. By contrast, the results of mass testing in the population indicate rapidly falling prevalence. A strategy of ‘unremarkable COVID-19’ is in sight It is not necessary nor likely possible at an acceptable social or economic cost to reach “Zero Covid”. Furthermore, the methods proposed to monitor progress are flawed. This point was made by the eminent statistician Sir David Spiegelhalter some time ago. As prevalence falls, the impact of the operational false positive rate (which has never been properly determined) comes to dominate the results. At very low prevalence, with mass testing of those without symptoms, it is unavoidable that most of the positive test results are false. Given the backdrop of vaccines, natural immunity and novel, effective treatments, it is HART’s position that we can safely shift focus away from this single virus. A strategy of ‘unremarkable COVID-19’ seems a more pragmatic and ethical solution and one which lines up with public health strategy on numerous other infectious diseases. Computer modelling – handle with care In contemplating the consequences of emerging from lockdown, it is concerning that we continue to apply high weighting to the results of computer modelling. Models are imperfect. A recent paper from Imperial College predicted over 100,000 deaths from COVID-19 between now and summer 2022. However, an undergraduate student of mathematics spotted a serious error in the assumptions in the model, as agreed by the modelling team in a cordial exchange with this bright student. The Imperial team had not accounted for the strongly seasonal nature of virus transmission. Due caution is strongly encouraged when looking at modelling outputs; it is important to look at the empirical data and the underlying assumptions. One of the best examples of modelling failure is Sweden. In the below, the orange bar represents the age and gender-adjusted mortality per 10k population predicted by a team who employed a model based on work by Ferguson et al, assuming Sweden didn’t institute a stringent lockdown similar to the UK. In the event, Sweden did not adopt such measures; mortality (blue bars) was actually slightly greater than in recent years, but unremarkable when viewed over the past decade, and clearly not remotely close to the disaster predicted. |
Sources:
https://www.medrxiv.org/content/10.1101/2020.04.11.20062133v1.full.pdf
https://www.statista.com/statistics/525353/sweden-number-of-deaths/
https://www.statistikdatabasen.scb.se/pxweb/en/ssd/START__BE__BE0101__BE0101I/Dodstal/
What are the risks of not lifting lockdown?
The evidence is clear that the longer these restrictions are in place, the greater the threat to our economy, livelihoods, mental and physical health and our children’s future. Some businesses will no doubt bounce back in time, many unemployed people will find work again, but the chances of a full recovery are diminishing by the day. Our top priority, as always, should be the wellbeing of our children. Experts are calling for urgent action. We need to act now to safeguard the potential of our most vulnerable young people and ensure that continuing restrictions do not derail their path to a happy and successful future.
It appears we are already beyond the risk of overwhelming the NHS, which is great news. HART believes now is the time to lift restrictions as we aspire to a world where COVID-19 is treated like other seasonal respiratory viruses, as explained by pathologist Dr John Lee in this newspaper piece.
