

No one needs folic acid fortification
Dr Clare Craig
In 1875, Parliament made it a criminal offence to adulterate flour.
The Sale of Food and Drugs Act of that year was written in answer to a scandal that had been building for decades. Bakers bulked out their flour with alum, chalk and plaster of Paris, and on occasion with sawdust. In 1861 Dr Edward Lankester told the Royal Society of Arts that 87 per cent of the bread and 74 per cent of the milk sold in London was adulterated. The Act was intended to end all adulteration; its long title promised “better provision for the Sale of Food and Drugs in a pure state”. Section 3 made it an offence to “mix… any article of food with any ingredient or material so as to render the article injurious to health”, with a second conviction punishable by being “imprisoned for a period not exceeding six months with hard labour”. Section 6 forbade selling any food “not of the nature, substance, and quality of the article demanded”. The principle was that you do not tamper with the staple food of the nation.
One hundred and fifty-one years later, the British government is about to add a substance known to be injurious to health – folic acid – to our flour.
From 13 December 2026, under the Bread and Flour (Amendment) Regulations 2024, it will be mandated that any white flour sold in the UK contains synthetic folic acid. The mandate includes imported flour and even organic flour. The stated aim is to ensure that women in the first trimester of pregnancy have adequate intake in order to reduce neural tube defects such as spina bifida and anencephaly (the absence of a brain). The policy has been presented as a straightforward public health benefit but like many such claims the risks have not been properly measured and the benefits have been massively exaggerated (with nine dead babies for every neural tube defect ‘prevented’) – if they exist at all.
The assumption is that there is a group of women who are short of folate. Therefore folic acid in the food will reduce the size of the group with inadequate levels. But this story is not like other stories of deficiencies. With rickets from too little vitamin D, scurvy from too little vitamin C, or goitre from too little iodine there is a genuine missing nutrient and a direct measurable and predictable consequence of that.
There is no deficiency like that regarding folates.
Today we are told folic acid fortification is obviously necessary. However, forty years ago, Britain’s own expert committee was adamant that it was not. What changed between then and now is worth following carefully, because it was not the evidence.
Is anyone deficient?
If you measure folate levels across a population the result is a bell curve. There is no point below which deficiency suddenly begins. There is no level that predicts neural tube defects. For decades this problem perplexed the medical profession. Then Irish data, published by Daly and colleagues in 1995, did link folate levels to neural tube defects. They showed that at every level of folate stores there was a risk of a neural tube defect but the lower the stores the higher the relative risk. Women with higher folate had lower risk than women with lower folate, but the risk never reached zero, not even at the very top of the distribution. Nor was there a deficient subgroup sitting below a threshold, waiting to be fed up to normal.
When you give an undernourished person more food, they reach a normal level and stop; the surplus is dealt with and excreted. Folic acid does not behave that way. Add it to the food supply and folate rises across the entire population, including in the great majority who had perfectly adequate levels to start with. That is not the correction of a deficiency. It is what a drug does.
What happened in Chile
Chile mandated folic acid fortification of flour in 2000, and the levels of folate stores increased across the whole population. Serum folate rose almost fourfold and red blood cell folate rose 2.4-fold, for everyone. The before-and-after curves barely overlapped. Almost nobody in fortified Chile had a folate level that would have counted as normal in the Chile of the year before. Only levels that had once belonged only to the extreme high end of the bell curve saw any overlap with the earlier measures.
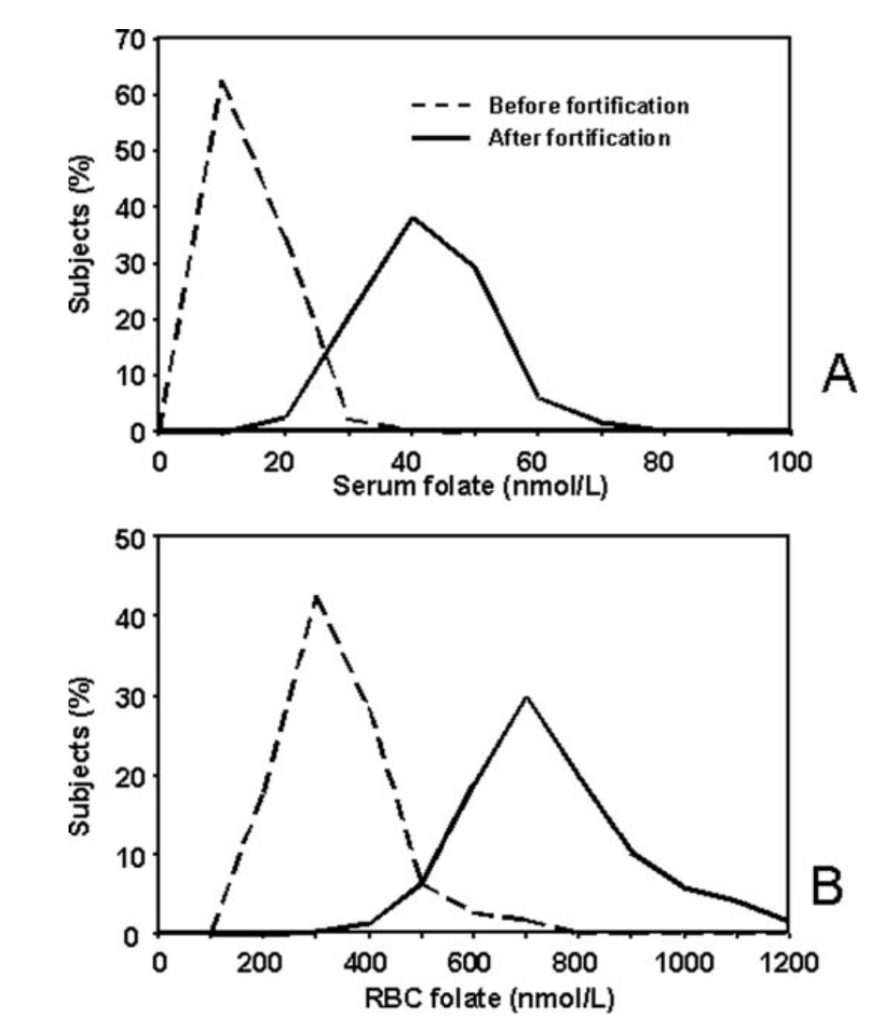
Figure 1: Serum folate (A) and red blood cell folate stores (B) in women of reproductive age in Chile before and after folic acid fortification of their flour
Shifting an entire population along a distribution is a pharmaceutical effect, and the long-term consequences of doing it to every person of every age, sex and health risk is simply not known. The assumption that having higher levels can only be good is wild. We do not know under what circumstances lower folate stores may be of overall benefit. There may be perfectly good reasons why folate stores are sometimes lower in some people. For a start, folate fuels cell division, which is precisely why fast-growing tumours depend on it too. It is an astonishing act of hubris to assume that we know better than human physiology what a “healthy” folate store should be.
Why does the government want to add it to flour?
The claim the government makes is that folic acid supplementation reduces neural tube defects. There is some evidence of that from animal studies showing that folate deficiency in brain cells is the cause of these defects and giving very high doses to women at high risk does reduce that risk in trials. However, the only trial of a reasonable dose in low risk women showed an illusory benefit with nine dead babies for every claimed prevented defect.
The deficiency argument runs into a second, more awkward fact. The great fall in neural tube defects in Britain happened before any folic acid campaign began.
A retrospective study by Kadir and colleagues, published in the BMJ, tracked neural tube defects in England and Wales from 1972 to 1996 using national data on live births, stillbirths and terminations. The figures are striking. Spina bifida fell from 215 per 100,000 births in 1972 to 38 per 100,000 by 1991, a fall of 82 per cent. Anencephaly fell by 81 per cent and encephalocele by 77 per cent over the same years.
The official recommendation that women take 400 micrograms of folic acid a day in the first trimester or when trying for a baby did not arrive until 1992. That was after almost all of that decline had already happened. None of the reduction can be credited to folic acid.
What is more, the authors looked at what happened next and found that the rate of decline slowed after 1992, significantly so. As folic acid prescriptions and over-the-counter sales climbed through the decade, the fall in neural tube defects decelerated rather than accelerated. That is the opposite of what the policy predicts, and there is a biological reason for it that I take up in the third article of this series. For now it is enough to note the shape of the thing: the decline came first, and the intervention arrived to take the credit.
What Britain decided in 1981
Earlier policymakers understood all of this. When they examined the same question they reached the opposite conclusion to today’s public health officials.
In 1981, the Department of Health published Nutritional Aspects of Bread and Flour, the report of an expert panel of the Committee on Medical Aspects of Food Policy. The panel — chaired in turn by Sir Frank Young and Dr John Cummings, and including Dr Elsie Widdowson, co-author of the foundational wartime bread studies — reviewed every additive then required in British flour and recommended, unanimously, that ALL of them be removed. The Chief Medical Officer, Sir Henry Yellowlees, set out the conclusion in the preface, “The Panel concluded unanimously that there is no nutritional reason for continuing to add calcium carbonate compulsorily to flour or to restore thiamin, nicotinic acid and iron to flour.”
On folate the panel could hardly have been plainer. In the absence of any public health problem of deficiency, it found, “there is no evidence of a public health problem arising from folate deficiency in the general population…. The Panel considered whether there was any nutritional justification for the addition of folic acid to flour and concluded that there was not.” Its reasoning on iron reads now like a direct answer to the argument being used today: “The fact that some individuals become iron-deficient due to clinical disease is not a basis for a national policy of adding iron to flour.”
At the time this was not thought controversial. It was simply the reasonable reading of the evidence. Today it has been almost entirely forgotten.
Something changed, but not the evidence
Between 1981 and 2024 there was no new evidence that British folate intakes had fallen. If anything the diet had improved: more fruit and vegetables, higher living standards, no return of any deficiency disease. There was no public health problem of folate deficiency then, and there is none now.
What changed was the momentum behind the public health greater good policy. In 1998 the United States produced a new and much larger folate recommendation, and in the same year mandated the fortification of American flour. For the next twenty-five years British advisory bodies were under steady pressure to fall into line. In November 2024 they did.
The stated case for the policy is the prevention of neural tube defects. Even if that benefit were achievable, this would be a sledgehammer to crack a nut. Tens of millions are exposed every year with no possibility of benefit, so any risk at all must outweigh it for them. The NHS lists large numbers of people who are told to avoid folic acid for their health including those with cancer, B12 deficiency, stents and kidney disease. Most of them have no idea that this will mean avoiding all flour. In addition there are numerous other risks including a doubling of the risk of prostate cancer in men and inhibition of immune response in women.
