

Witness Name: Dr Rosamond Jones on behalf of:
Children’s Covid Vaccines Advisory Council (CCVAC)
Statement No: 1
Exhibits: 241
Dated: 13-11-2024
UK COVID-19 INQUIRYWITNESS STATEMENT OF CCVAC
CONTENTS Paragraph
INTRODUCTION 1-10
OVERVIEW 11
IMPACT OF SARS-CoV-2 INFECTIONS ON CHILDREN 12-17
IMPACTS OF PANDEMIC MANAGEMENT ON CHILDREN 18-25
VACCINE DEVELOPMENT AND TYPE OF APPROVAL 26-45
ADULT VACCINES 46-54
VACCINE TRIALS IN CHILDREN 55-74
INITIAL PLANS, THEN MISSION CREEP 75-80
AUTHORISATION PROCESS & POLICY MAKING RE VACCINES FOR CHILDREN 81-110
FAILURE OF PHARMACOVIGILANCE 111-132
MARKETING TO CHILDREN 133-146
VACCINES IN PREGNANT AND LACTATING WOMEN 147-156
ETHICAL & LEGAL ISSUES 157-164
CENSORSHIP 165-171
SUMMARY 172-175
IMPORTANT QUESTIONS for the MHRA & JCVI 176-178
I, DR ROSAMOND JONES, will say as follows: –
INTRODUCTION
1. I make this statement on behalf of CCVAC pursuant to the Covid-19 Inquiry’s Module 4 Rule 9 request dated 9 November 2023.
2. The evidence presented is true to the best of my knowledge and belief.
3. The Children’s Covid Vaccine Advisory Council is an independent group of health professionals and scientists who came together specifically to challenge the government advice on the benefits and risks of covid vaccines for children. We come from a wide range of specialties including public health, general practice, paediatrics, intensive care, emergency medicine, microbiology, pathology, palliative care, obstetrics, oncology, pharmaceutical medicine and academics in genomics, ethics, and risk management. The group collaborated informally from May 2021 and more formally from February 2022.1 Individuals held differing views on the use of covid vaccines in the elderly and vulnerable but were and are united in our shared concerns that Covid-19 vaccines were not appropriate for healthy children. This view does not reflect our view on vaccination in general. For simplicity, we/our in this statement refers to the CCVAC. A list of over 30 letters we have written is contained in Appendix A.
4. I am the convenor of the CCVAC. My full CV is attached in Appendix B. All my work has been pro bono and I have no conflicts of interest. There are four other people on the leadership team: Professor Angus Dalgleish, Dr David Critchley, Dr John Flack, Professor David Livermore, whose CVs are also attached. A list of all members with job titles and qualifications is provided by way of evidence of the breadth of specialist expertise. Since May 2021 we have written 25 letters – for each letter the first author has shared drafts with relevant interested parties before each letter has been circulated to all members for their response. Every person listed on each letter has specifically endorsed that letter. Our aim has been to bring to the attention of the regulators, the serious questions over the safety of Covid vaccines for healthy children, in light of their very low risk from SARS-CoV-2 infection and the lack of any long-term safety data for these products. Where the regulators failed to respond, we then shared our concerns with ministers and other policy makers. We also shared all our letters with the public, to ensure that parents had access to a range of opinions on this topic.
5. I am also a member of the Health Advisory & Recovery Team (HART), which has been asked to provide a statement. The aims of each group are different and the CCVAC is focused primarily on covid vaccines in children, which this statement addresses.
6. As per the Inquiry’s Rule 9 request, this statement covers our concerns about the development and approval of vaccines during the pandemic, the Joint Committee on Vaccination and Immunisation (JCVI) recommendations on eligibility and decisions taken by policy makers concerning the vaccination of children. It also covers vaccine safety issues particularly pertaining to children, including post-marketing surveillance.
7. It also covers our concerns about the ethical and legal aspects of promoting vaccination of children with the aim of protecting adults.
8. We have provided evidence for a Judicial Review into the vaccination of 12-15-year-olds and also a separate legal challenge for 5-11-years-olds.
9. Our letters have gone to, inter alia, the Medicines and Healthcare Products Regulatory Authority (MHRA), the Joint Committee on Vaccination and Immunisation (JCVI), the Commission on Human Medicines (CHM), Chief Medical Officers (England, Scotland, Wales & Northern Ireland), Government Chief Scientific Adviser, UK Health Security Agency (UKHSA), Paediatric Medicines Expert Advisory Group (PMEAG), the Pharmacovigilance Expert Advisory Group (PEAG), the Patient Safety Commissioner (PSC), Nuffield Council on BioEthics, the General Medical Council (GMC) and the Medical Defence Union. All letters and any responses are provided in Appendix A.
10. I attended the All-Party Parliamentary Group on Covid-19 Vaccine Damage alongside the Perseus Group.
11. OVERVIEW
a. We contend that there was never an emergency regarding the health of children.
b. The pandemic management, in terms of fear messaging, school closures, masking of children and enforced social isolation was disproportionate to any risk to children from SARS-CoV-2 and set the scene for a demand for an unnecessary vaccination.
c. Given the lack of risk, there was never any justification for authorising or recommending the use in healthy children of novel technology gene-based vaccines with no long-term safety data.
d. To give such vaccines to children for the possible protection of vulnerable adults is a clear breach of our ethical duty.
The statement below sets out our detailed rationale and evidence for the above.
IMPACT OF SARS-CoV-2 INFECTIONS ON CHILDREN
12. Before the pandemic reached the UK, data from China and then from Italy had shown that this was a disease that primarily gave severe disease only in the elderly and infirm. In China,2 of the first 44,562 confirmed cases and 1,023 deaths, there was not a single death of a child under 10. For 10-39s there was a case fatality rate of 0.2% compared to 14.8% in the over 80s. Moreover, this was a likely overestimate of severity, largely because of undercounting of mild cases. The case fatality rate observed in China fell from 5% in the first 10 days of January, to 0.3% overall from 11th January to 11th February. In Italy, the average age of death from Covid was reported as higher than the all-cause average age of death. This was subsequently confirmed in England and Wales. Estimates of numbers of deaths from Covid were exaggerated by including anyone who died following a positive PCR test, regardless of the actual cause of death and the time interval after the PCR result. From August 2020 death counts were altered to count those within 28 days post test and/or with Covid-19 listed as a cause on the death certificate.
13. Fortunately, death in childhood is a rare event in the UK and all deaths are reviewed regularly to look for avoidable factors. A detailed review of child deaths between March 2020 and March 20213 (i.e. covering the first two covid waves) found 61 with a positive PCR test, for whom a detailed notes review found that in 36 children this was deemed to be coincidental, leaving 25 children where Covid-19 was either the main cause of death or a contributing factor. Of those 19 had major comorbidities, 15 of which were described as life limiting. Only 6 deaths occurred in otherwise healthy children, 3 of whom died acutely and 3 with a rare post-covid inflammatory condition (PIMS-TS). This was from a total population of over 12 million children and young people with 3105 all cause deaths. Risk of death from Covid-19 for healthy children was estimated at 1 in 2.5 million.4 Data from UK, US, S Korea, France, Germany and Spain confirmed mortality in children to be very low5 with covid-19 deaths accounting for only 0.48% of all childhood deaths.
14. Death rates from Covid-19 by age band for England and Wales, taken from Office of National Statistics (ONS) data for 20206,7 are shown in Figure 1. There is a nineteen thousand-fold difference in mortality rate between the over-80s (16,572 deaths per million=1.66%) and the under-15s (less than 1 per million=0.0001%). Understanding this, is vital to any decision making about the balance of benefit and risk for any intervention, whether lockdowns, masks or vaccines.
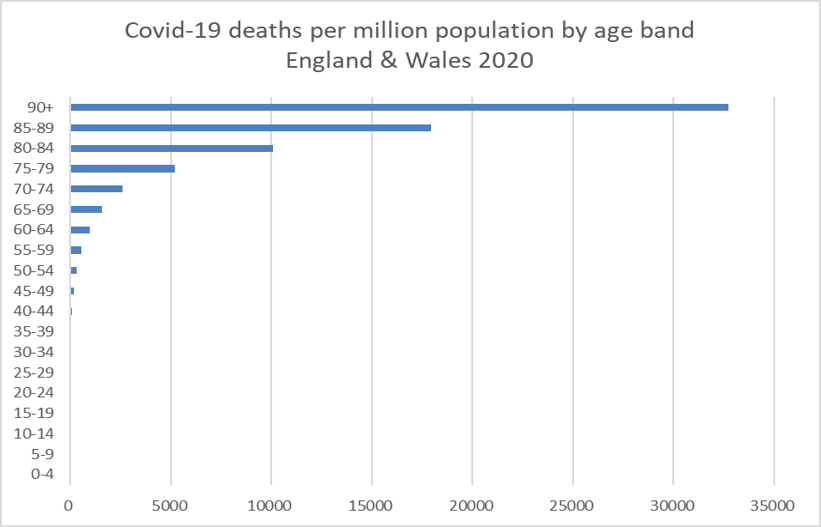
Figure 1. Covid-19 deaths per million population by age band, England & Wales 2020, ONS
15. Likewise serious hospital admissions for children were a rarity, and intensive care admissions even more so.8 Risk factor analysis for intensive care cases confirmed that for Covid-19, acute admissions were strongly linked to serious comorbidities and were similar to risk factors with childhood influenza admissions. A subgroup of children admitted with PIMS-TS were older and more likely to be Black or Asian or have a raised BMI. Children with no underlying comorbidities made a good recovery, irrespective of ethnicity.9 It is important to note that there is considerable similarity between PIMS-TS and Kawasaki disease which is caused by other viruses. The incidence of Kawasaki disease apparently halved in the covid era. PIMS-TS therefore should be considered in that context, with some Kawasaki cases presumably being recategorized as PIMS-TS.10
16. Once testing of children became widespread (see para 19e below), it was apparent that the vast majority of children encountering SARS-CoV-2 had either no or trivial symptoms.11 Long-Covid which has caused concern among adults, was shown to be rare and when it did occur, was milder and of shorter duration than in adults.12 Studies that compared symptoms after a positive test with children who had tested negative, showed very similar levels of headache, fatigue, depression and muscle aches and the term ‘long pandemic’ was coined.13
17. There has been much discussion about why children are affected so much more mildly. So-called innate immunity, which is the body’s initial defence to all invading organisms at first encounter, is already recognised to be much more robust in young children, and this has been confirmed for SARS-CoV-2 infection;14,15 other potential factors have been fully reviewed.16
IMPACTS OF PANDEMIC MANAGEMENT ON CHILDREN
18. In order to understand the background to the vaccine rollout, it is necessary to look at some of the major ways in which children’s lives had already been impacted by the pandemic management prior to the vaccine deployment. School closures starting in March 2020 seriously impacted children, who were themselves at minimal risk from SARS-CoV-2. Harms included the huge education loss which widened the gap for lower income families, plus the impact on children’s mental health. Reports from both Amanda Spielman, Chief Inspector for Education17 and Anne Longfield, the then Children’s Commissioner18 confirm these points. A paper on the impact of school closures was prepared for SAGE in early 2021.19
19. The disruption caused by non-pharmaceutical interventions led to a situation where parents and children were desperate to return to normality. Without such policies it is questionable whether any parent would have considered vaccinating their child against Covid-19, given the lack of direct benefit to them. These policies and key decisions included:
a. In early summer 2020, public houses reopened before schools, giving children and parents a message that children were either at serious risk themselves (clearly not the case) or were likely to be bringing SARS-CoV-2 infection home from school. When schools were scheduled to reopen, there was major lobbying from teachers’ unions,20 such that the Secretary of State for Education pulled back from compulsory reopening of school in June 2020, leaving it instead to individual headteachers. The result was a postcode lottery for children.
b. Lack of evidence of major transmission in school: Prolonged school closures were predicated on the idea that schoolchildren would be a major source of transmission but the evidence for this was not forthcoming. Rather, evidence from Public Health England (now UKHSA) showed that risk of transmission of SARS-CoV-2 was significantly greater from adult to child than the reverse.21 Data from Public Health Scotland revealed that teachers were less likely than other workers to be hospitalised with Covid-19 and had a reduced risk of serious disease.22 This may be because teachers are heavily exposed to other longestablished coronaviruses and that this exposure conferred some cross-immunity. The trajectory of infections in children followed that of infections in the community as a whole. No rise was seen throughout September 202023 after schools returned, a jump was seen in January when a fall would be expected from schools having shut, and no rise was seen in March 2021 when schools returned after the lockdown.
c. Masking of children in schools: Masks were first discussed for schoolchildren during summer 2020 and Dr Jenny Harries, then Deputy Chief Medical Officer suggested they might cause more harm than good, particularly because of repeated handling. She also acknowledged the poor evidence base for any protection from standard non-fitted masks.24 A letter sent to the Chief Medical Officer and the Chief Scientific Adviser in August 2020 (included in Appendix A) produced the reply that this decision was taken by the Department for Education.25 However, by September, masks were required in secondary school corridors. At that point, the Prime Minister confirmed that they would not be required in the classroom, stating “That’s clearly nonsensical, you can’t teach with face coverings and you can’t expect people to learn with face coverings.” However, mission creep soon led to masks in classrooms too. Leaked WhatsApp messages from Matt Hancock, then Health Secretary, imply that this decision was based on a political wish not to be upstaged by Nicola Sturgeon.26 That children’s wellbeing could be used as a political football is clearly inappropriate.
A recent systematic review of child mask mandates has concluded there was no robust basis for them whatsoever.27
d. Even primary school parents were required by many schools to wear masks when dropping off or collecting their children from the school playground; parents attending toddler groups were also expected to mask, despite the obvious impact that would have on speech and language development. For young children coming out of school to a sea of masked adults, the obvious implication is that the said adults need to be protected from children.
e. Routine testing of school children: in November 2020, a pilot study was carried out in Liverpool on regular testing for SARS-CoV-2 infection. Recruitment was on an ‘opt out’ basis and with significant emotional pressure on parents to comply.28 The lateral flow test being promoted had not at that time even been approved by the devices section of the MHRA. A letter to Public Health England is included in Appendix A. The UK National Screening Committee were not involved in setting up this programme.29 Very quickly this so-called pilot project was rolled out across the country, with teachers and pupils expected to take a test once or twice a week. The net result was that the inevitable false positive tests greatly increased the number of ‘cases’, leading to further lost education not only for the individual child but also for their classmates, who were also sent home from school. The so-called ‘pingdemic’ seen in summer 2021 was temporally related to the pressure and indeed the rationale for childhood vaccination – see para 97.
20. Failure to consider potential harms of non-pharmaceutical interventions (NPIs) or to consider ways of improving general health. At the same time as school closures, children’s outdoor sports were cancelled and playgrounds closed, with no consideration of ways to keep children active. Only the BBC’s Joe Wicks provided remote-led indoor exercise each morning, but this lacked the important social interaction required by children and also reduced their access to sunshine and hence Vitamin D, known to be vital for normal immune function. The arbitrary ‘Rule of 2’ meant that an ‘only child’ was deprived of any contact with other children and indeed a single parent could not meet a friend outdoors if their children were too young to be left alone at home. All of this conspired to make young families extremely vulnerable to the mental health impacts of the lockdown.
21. The argument put forward for introducing all these measures was that governments around the world were facing an unknown threat for which they were not prepared and that they had to ‘do something’. This is the reverse of the precautionary principle, which states that if there is no evidence of benefit from a procedure then it should not be undertaken. Thorough reviews of the evidence for non-pharmaceutical interventions (NPIs) designed to reduce viral transmission had already been undertaken by the Cochrane Collaboration30 and the WHO31 and had been used when drafting the existing pandemic plans. These found that, overall, there was limited and poor-quality evidence for NPIs, and that their impact on respiratory viral transmission was therefore likely to be limited. Regular hand washing particularly in young children, and isolation of symptomatic individuals were two recommendations from these reviews with a greater evidence-base. There is no robust evidence for the use of face masks by children or the general population (there was some evidence for use by staff in hospital and care settings when combined with gloves and gowns). The WHO review found “very low” quality of evidence on the impact of school closures and highlighted many negative consequences. Sweden did not close schools and did not enforce masking in schools (or elsewhere); the country suffered no adverse consequences in terms of pupil or teacher deaths and its children avoided the adverse consequences of the policies pursued elsewhere, including in the UK.
22. Despite evidence of the negative impact on children of school closures in March 2020, further closures took place in January 2021, around the time vaccines became available. This underscored the idea that vaccination was the only way out of the pandemic. The lack of evidence base for school closures was again highlighted in a leader in the British Medical Journal in February 2021.32
23. Fear messaging: it was confirmed from early in the pandemic that fear messaging was being deployed in order to increase compliance with lockdown measures, particularly among younger adults, see SAGE meeting minutes.33 The use of face masks by the public also served to provide a prosocial nudge “Wearing a facemask could demonstrate that an individual is concerned for other peoples’ welfare and is enacting desired social norms around safety and hygiene.” 34 It was suggested that mask wearing should be encouraged by social rather than medical messaging.35 ‘I wear my mask to protect you’ became the order of the day. Fear messaging was also aimed indirectly at children, with the phrase ‘Don’t Kill Your Granny’.36
24. Natural immunity: Naturally acquired immunity was repeatedly downplayed by politicians and senior medical advisers but data showed good antibody levels persisting 14-months after infection.37 Children have been shown to develop more robust immunity than adults both systemically,38 and in the upper airway.39 A study published early in 2020 from Singapore,40 tested 23 people who had recovered from SARS in 2003, and found that they still “possess long-lasting memory T cells that are reactive to the N protein of SARSCoV” (the virus associated with the SARS epidemic). Importantly, they also showed, “these T cells displayed robust cross-reactivity to the N protein of SARS-CoV-2”. These T-cells remained years after antibodies had waned. They also looked at 37 individuals with no history of SARS or COVID-19 or even contact with individuals who had had SARS and/or COVID-19. This group also had SARS-CoV-2-specific T cells, which the authors suggest may have arisen from past infection with other beta coronaviruses (this is the same family of viruses that are involved in the common cold).
25. Vaccines as the way out of lockdown: it was made clear by Boris Johnson that the only way back to normal life would be via widespread vaccination, and the various steps on the ‘Road Map’ back to normal were linked to steps in the vaccination rollout.41 Consequently, those most impacted by lockdowns would be amenable to receiving a vaccine even if they had already had Covid-19 and regardless of their own risk from SARS-CoV-2 infection. Mark Drakeford, First Minister for Wales, said in May 2021 even before vaccines were authorised for children, “Whether we might, by the autumn, be able to have young people returning to schools with a vaccine available to them and as a result some of the measures we currently have in schools, such as children wearing masks, might be able to be eased because vaccination will have been moved lower down the age range.” 42 In England reopening of night clubs in 2021 was linked to use of a Covid-pass with an announcement that double vaccination would be required in September.43 Thus discrimination against the unvaccinated briefly became a stated government policy, although in the event the proposal was never implemented.
VACCINE DEVELOPMENT AND TYPE OF APPROVAL
26. Much of the information in paragraphs 27-45 will have been covered elsewhere, particularly by the Perseus Group, but it is highly relevant to the rollout of these Covid19 vaccines for healthy children that the Inquiry is aware of the many concerns about the vaccine development and safety testing. The concerns discussed in this section become more relevant the lower a person’s risk from SARS-CoV-2 infection, and hence the change in risk:benefit balance (see Figure 1 para 14 above). It is noteworthy, that on 29th February 2020, Professor Chris Whitty, Chief Medical Officer (CMO), commented in a WhatsApp44 that “For a disease with a low (for the sake of argument 1%) mortality a vaccine has to be very safe so the safety studies can’t be shortcut. So important for the long run.” Sir Patrick Vallance, government Chief Scientific Advisor, agreed, responding, “Agree, existing drugs best things to try for this outbreak. Accelerate vaccine testing where we have good candidates for future, and prepare for manufacturing capacity for longer term.” Yet, the evidence is clear that many of the safety studies were cut, making these vaccines totally unsuitable to younger sections of the population whose likely mortality rate would be far lower than Professor Whitty’s suggested 1%.
27. Most of the vaccines developed for use against Covid-19 involved a novel gene-based technologies not previously used outside of clinical trials in human populations: some (AstraZeneca, Johnson & Johnson, and the Russian Sputnik) use DNA with an adenovirus vector; others (Pfizer and Moderna) use mRNA delivered with a lipid nanoparticle technology. All of these gene-based medicines should have been considered as “prodrugs” since the active moiety – the spike protein – was produced by the recipient using the injected genetic code. A prodrug is a pharmacologically inactive medication or compound that, after intake, is converted within the body into a pharmacologically active drug. The prodrug in this case is the messenger RNA which codes for the spike protein. In order to work as a vaccine, the mRNA first has to enter into a cell and then has to instruct the intracellular ribosomes to make a foreign protein which then has to be passed back out of the cell where it can be recognised by the person’s immune system leading to antibody production and an immune memory. This is different from a standard vaccine, in which the foreign protein itself would be given in a measured amount. In order to get the mRNA into the cells, it first had to be modified using pseudouridine so that the mRNA wouldn’t be broken down immediately. It also had to be coated in a lipid envelope to allow it to cross cell membranes. In addition, toxicology studies should have been conducted on all components of the vaccines, including the spike protein and the modified RNA itself and the lipids used in the nanoparticles, which have their own toxicity profile.
AstraZeneca is also effectively a ‘prodrug’ with a portion of DNA in this case linked to a non-replicating virus (so-called ‘viral vector’ technology) to enable cell entry. It then uses a similar mechanism to the mRNA vaccines, in that the genetic material given to the vaccine recipient then instructs their own cells to make the spike protein.
One major problem with both these technologies is that there were no appropriate pharmacokinetic studies during the vaccine development phase, to study how much spike protein would be made and in what organs of the body, and how much this might vary between individuals. Regarding children, it is unknown whether the quantity or duration of spike protein production would be more or less than that of adults.
28. In December 2019 the World Health Organisation (WHO) highlighted the need for separate regulations for mRNA vaccines in a consultation report45 which concluded: “The consultation also recognized that development of RNA-based vaccines requires WHO action…It was clear that the scientific evidence for these vaccines is limited and more data will most likely become available in coming years.” The WHO established meetings in autumn 2020 to draft new regulations and a first draft was published in December 2020,46 a year after they had first highlighted the need for this and just as the Covid-19 vaccines were first gaining approvals. However, these regulations were never ratified, and the standard vaccine regulations were used instead.
29. The 2017 WHO guidelines on clinical evaluation of vaccines were followed47 and state:
“It is strongly recommended that dialogue with the appropriate NRAs [national regulatory authorities] occurs at regular intervals during the pre-licensure clinical development programme to allow for agreement to be reached on the content and extent of the application dossier. This is especially important in the following cases:
■ The clinical programme proposes a novel approach to any aspect of development for which there is no precedent or guidance available.”
“Consistency of production is essential, and the demonstration that the product does not differ from vaccine lots that have been shown to be safe and adequately immunogenic and protective in clinical studies is a crucial component of vaccine evaluation, licensing and batch release.”
30. The latest WHO guidelines on nonclinical evaluation of vaccines are dated 200548 and state: “Potential safety concerns for a vaccine product include those due to inherent toxicities of the product, toxicities of impurities and contaminants, and toxicities that result from interactions between the vaccine components present in the vaccine formulation….The need for and extent of nonclinical testing will depend on the product under consideration. For example, for a product for which there is no prior nonclinical and clinical experience, nonclinical testing would be expected to be more extensive than for those vaccines previously licensed and used in humans”.
31. The draft WHO guidelines which were abandoned (see para 28 above) are much more strongly worded: “It is considered that mRNA vaccines are to be regulated as biologicals, and like other biologicals, adequate control of the starting raw materials and manufacturing process is as important as that of the final product. Regulatory considerations therefore place considerable emphasis on the control strategy of the manufacturing process of the vaccine as well as on comprehensive characterization and release testing of the bulk substance and the vaccine itself.” The importance of the correct classification of the products is that it would have led to the appropriate preapproval testing, as discussed in Paragraph 36, which in the vaccine paperwork was simply marked as N/A (not applicable).
32. Evidence from Pfizer and Moderna submissions to the US Securities & Exchange Commission in mid-2020, showed that their mRNA products were classed as gene therapies. Pfizer in its 2019 end-of-year report49 stated (page 14), “To our knowledge, there is no current precedent for an mRNA-based immunotherapy such as the type we are developing being approved for sale by the FDA, European Commission or any other regulatory agency elsewhere in the world. Although we expect to submit BLAs [Biologic Licence Applications] for our mRNA-based product candidates in the United States, and in the European Union, mRNA therapies have been classified as gene therapy medicinal products, other jurisdictions may consider our mRNA-based product candidates to be new drugs, not biologics or gene therapy medicinal products, and require different marketing applications. Securing regulatory approval requires the submission of extensive preclinical and clinical data and supporting information to the various regulatory authorities for each therapeutic indication to establish the product candidate’s safety and efficacy. Securing regulatory approval also requires the submission of information about the product manufacturing process to, and inspection of manufacturing facilities by, the relevant regulatory authority. Any product candidates we develop may not be effective, may be only moderately effective, or may prove to have undesirable or unintended side effects, toxicities or other characteristics that may preclude our obtaining marketing approval or prevent or limit commercial use.”
33. Moderna said in August 2020,50 “No mRNA drug has been approved in this new potential class of medicines, and may never be approved as a result of efforts by others or us. mRNA drug development has substantial clinical development and regulatory risks due to the novel and unprecedented nature of this new class of medicines…..Currently, mRNA is considered a gene therapy product by the FDA. …. In addition, because no product in which mRNA is the primary active ingredient has been approved, the regulatory pathway for approval is uncertain…. Moreover, the length of time necessary to complete clinical trials and to submit an application for marketing approval for a final decision by a regulatory authority …. may be difficult to predict.” Yet to describe these products as ‘novel technology’ or as ‘gene therapy’ after their approval, led to denigration as a ‘conspiracy theorist’.
34. Pharmacokinetic studies were leaked by a member of the Pfizer team in Japan in 2020, and the findings were subsequently confirmed through an FOI request to the Australian Therapeutic Goods Administration (TGA). Testing of a small number of rats looked at the lipid nanoparticle carrier only. Results showed that as expected, the lipid nanoparticles (LNPs) peaked at the injection site at 1 hour and were falling steadily over the next 48 hours. However, LNPs were distributed to and accumulated in many organs, with highest levels in the adrenal glands, the liver, the spleen and the ovaries, as shown in Table 1. The study was stopped at 48 hours when levels in these organs were still rising. Of particular concern for children or young adults, is the accumulation in ovaries, the significance of which is completely unknown, and could take decades to become apparent. The full data are available in the Nonclinical Evaluation Report.51
| Sample | Total Lipid Concentration (µg lipid equiv/g (or mL)) | ||||||
| Time post injection | 25 m | 1 h | 2 h | 4 h | 8 h | 24 h | 48 h |
| Injection site | 128.3 | 393.8 | 311.2 | 338.0 | 212.8 | 194.9 | 164.9 |
| Adrenal glands | 0.27 | 1.48 | 2.72 | 2.89 | 6.80 | 13.77 | 18.21 |
| Bone marrow | 0.48 | 0.96 | 1.24 | 1.24 | 1.84 | 2.49 | 3.77 |
| Liver | 0.74 | 4.62 | 10.97 | 16.55 | 26.54 | 19.24 | 24.29 |
| Ovaries | 0.104 | 1.34 | 1.64 | 2.34 | 3.09 | 5.24 | 12.26 |
| Spleen | 0.33 | 2.47 | 7.73 | 10.30 | 22.09 | 20.08 | 23.35 |
| Testes | 0.031 | 0.042 | 0.079 | 0.129 | 0.146 | 0.304 | 0.320 |
Table 1. Mean concentration of radioactivity (sexes combined) in tissue and blood following a single IM dose of 50 µg mRNA/rat
35. The report also revealed “A single-dose intravenous (IV) study in rats… demonstrated that both novel lipid excipients, ALC-0159 and ALC-0315 in the LNP formulation rapidly distributed from plasma to liver, which was the only organ collected for analysis…the concentration of ALC-0315 in liver tissue remained detectable on day 14.” This is the vaccine that the public were repeatedly told just stayed in the arm. At no point did the MHRA demand that further studies should be performed to test the duration of the lipid in any important organs. The testing was done on the delivery vehicle. We can find no evidence that the testing was done on the final product, spike protein produced by the cells, contrary to standard practice for compound drugs. No comparable blood work was performed in the Phase 1 human trials. To this day, there are no official data on where the mRNA is distributed nor for how long it remains active in inducing spike protein synthesis.
36. The use of standard vaccine regulations had major implications for the amount of animal safety testing. For example, no animal studies were required for genotoxicity (any effect on the genetic make-up particularly of sperm or egg cells), teratogenicity (i.e. causing fetal abnormalities), safety pharmacology (i.e. potential cardiovascular /neurological/ haematological and immunological toxicities) or carcinogenicity (cancer-producing). As mentioned earlier, no studies were conducted to establish the potential toxicity of the therapeutically-active moiety of these mRNA injections (i.e.the translated spike protein): they were simply marked as ‘N/A’ (not applicable). This is unacceptable for a totally new technology, especially one that is going to be given to healthy children. The Australian non-clinical evaluation report does contain one reproductive study on 22 rats that found an increase in anomalies of the umbilical artery and also a four times increased rate of extra ribs compared with the control animals. But when compared with historical data, the difference was smaller and the authors opined, “Thus, the higher incidence of supernumerary lumbar ribs relative to the concurrent control group is not considered to be treatment-related.” Only as recently as 10th January 2024, a paper has been published52 by an independent group who gave mRNA vaccine or saline placebo to pregnant rats and found an increase in neurological problems in the male offspring.
37. The novelty and complexity of these new products should have led to extreme caution from regulators who should have raised the bar substantially, rather than facilitating rapid authorisations and whole-population deployment. WHO guidance53 states, “The manufacture, control and administration of biological active substances and finished products require certain specific considerations and precautions arising from the nature of these products and their processes. Unlike conventional pharmaceutical products which are manufactured using chemical and physical techniques capable of a high degree of consistency, the manufacture of biological active substances and finished products involves biological processes and materials, such as cultivation of cells or extraction from living organisms. As these biological processes may display inherent variability, the range and nature of by-products may also be variable. As a result, quality risk management (QRM) principles are particularly important for this class of materials and should be used to develop the control strategy across all stages of manufacture so as to minimize variability and reduce the opportunity for contamination and crosscontamination.” Yet there was a lack of Good Manufacturing Practices (GMP) applied to what are extremely complex and delicate mixtures, along with inadequate pharmacovigilance.
38. Enormous differences in adverse event rates between batches have also been highlighted, suggesting a lack of scrutiny of the manufacturing processes.54
39. In early 2021, leaked emails from the EMA55 revealed a significant drop in the RNA integrity of the Pfizer-BioNTech vaccine in commercial vaccine batches (Process 2) (around 55%) compared to clinical trial batches (Process 1) (around 78%). The EMA classified this drop in quality as a ‘product related impurity’ and simply lowered the acceptance criterion of the commercial batches rolled out to the general public to 50%.
Neither they nor the MHRA took any account of the mRNA, now with known impurities, being coated in a lipid nanoparticle specifically designed to help it cross cell membranes.
40. As if these concerns were not enough there is the additional problem of the lipid nanoparticle delivery system which was originally designed for gene therapy and therefore their ability to carry material to the cell nucleus. The Australian Non-Clinical Evaluation report cited above (see paras 34 & 36) includes images that clearly show the S1 portion of the spike present inside the nucleus of cells in culture after vaccine mRNA was inserted into the cell cytoplasm.
41. It was also repeatedly stated that the mRNA could not be incorporated into the DNA of the recipient but again independent researchers56 have found that DNA in human liver cell culture was altered within 6 hours of infusion with Pfizer BioNTech mRNA vaccine.
42. In 2023, independent testing57 of surplus vials of Pfizer’s Covid-19 vaccine revealed contamination with residual DNA fragments which were not completely removed during the Process 2 manufacturing process used for the commercial product. The FDA had issued a warning to manufacturers back in 2010,58 “Residual DNA might be a risk to your final product because of oncogenic and/or infectivity potential. There are several potential mechanisms by which residual DNA could be oncogenic”. In ‘Process 1’, the mRNA was produced by a PCR mechanism specifically for the trials, but for ‘Process 2’ where vaccine production was required at scale for whole populations, a completely different method was used, involving DNA fragments coding for the spike protein being inserted in E Coli bacteria which then replicate producing vast quantities of the DNA. This is then separated from the bacterial culture and then converted into mRNA. The trials for the authorisation were carried out almost entirely using the Process 1 pure product.
43. As recently as December 2023, 3 years after mRNA vaccines gained a conditional marketing authorisation, scientists from the MRC Toxicology Unit, University of Cambridge and colleagues from Oxford, Kent and Dublin, have investigated whether the use of the modified mRNA could affect the proteins produced. As the authors point out, “Despite their widespread use, surprisingly little is known about how ribonucleotide modification affects protein synthesis. Modified ribonucleotides are commonly incorporated… but their effects on mRNA translation fidelity have not been fully explored.” The findings “demonstrate that incorporation of N1-methylpseudouridine into mRNA results in +1 ribosomal frameshifting in vitro and that cellular immunity in mice and humans to +1 frameshifted products from BNT162b2 vaccine mRNA translation occurs after vaccination.” 59 The so-called ‘frameshifting’ occurs when a modified RNA sequence incorrectly codes for a specific string of amino acids that make up a protein. Instead of cells making the intended spike protein, they made a ‘nonsense’ protein. But no-one can say whether these ‘nonsense’ proteins matter.
44. Whilst there are arguable justifications for the emergency deployment of hurriedly developed vaccines/gene therapies in vulnerable individuals, all this basic science should have been completed by the manufacturers before they considered applying for approval for a vaccine for use in healthy children. If it had not been done, it should have been demanded by the regulators. The most basic role of a regulator is to ensure that the drug is what the manufacturer says it is. In this case the drug was a pro-drug, and the end product was considerably more variable and unpredictable than was claimed and also markedly different from the synthetic product used in the trials.60
45. Pfizer animal studies revealed “Antibodies and T cells in monkeys declined quickly over 5 weeks after the second dose of BNT162b2 (V9), raising concerns over long term immunity, which will be assessed by clinical studies according to the Sponsor” The human adult trials were presented for authorisation with only 2 months of data, and the brief duration of efficacy was not reported until after the rollout.
ADULT VACCINES:
46. Adult phase 2/3 trials: the adult trials had major shortcomings in terms of duration of follow up and unblinding. Pfizer/BioNTech started unblinding (and giving the vaccine to the placebo group) in its trial on 14 December 202061 less than 2 weeks after UK Temporary Authorisation. Unblinding may have been reasonable for any trial participants at high risk from Covid-19, but the majority were in good health and at low risk of severe disease. Unblinding destroys the control group and means no more meaningful safety or efficacy data can be collected after that point.
47. The removal of the control group was in contravention of advice from the International Coalition of Medicines Regulatory Authorities of which the MHRA is a member.62 This decision greatly undermined the ability of the trials to assess mid- to long-term safety, with adverse events subsequently reported via the Yellow Card system often dismissed as coincidences. The durability of efficacy also became unknowable. This is highly relevant to the decision over vaccinating children as, despite JCVI delaying its decision for several months, there were no more data forthcoming from the adult trials.
48. Adult trials also failed to consider all-cause mortality as a formal endpoint and confined themselves to looking at deaths from Covid-19. Pfizer failed to highlight that there were more deaths in the vaccine arm of the trial than in the placebo. The US Food & Drug Administration (FDA) reported60(page 23) “From Dose 1 through the March 13, 2021 data cutoff date, there were a total of 38 deaths, 21 in the COMIRNATY (Pfizer vaccine) group and 17 in the placebo group. None of the deaths were considered related to vaccination.” Pfizer reported63 four cases of cardiac arrest in the vaccine group compared to one in the placebo group. Real world data subsequently demonstrated the risk of myocarditis particularly in younger adults after mRNA vaccines and it is entirely plausible that any Covid deaths prevented in the vaccine arm were more than offset by vaccine-induced cardiac deaths.
49. Post-marketing pharmacovigilance and real-world data: the Yellow Card reporting system, the American Vaccine Adverse Events Reporting System (VAERS) and European Medicines Agency (EMA) report all received adverse events reports including deaths in numbers far above those reported for previous vaccines over a 30-year period, as shown in Figure 2.64 This excess is evident even after correcting for the large number of Covid-19 doses given.
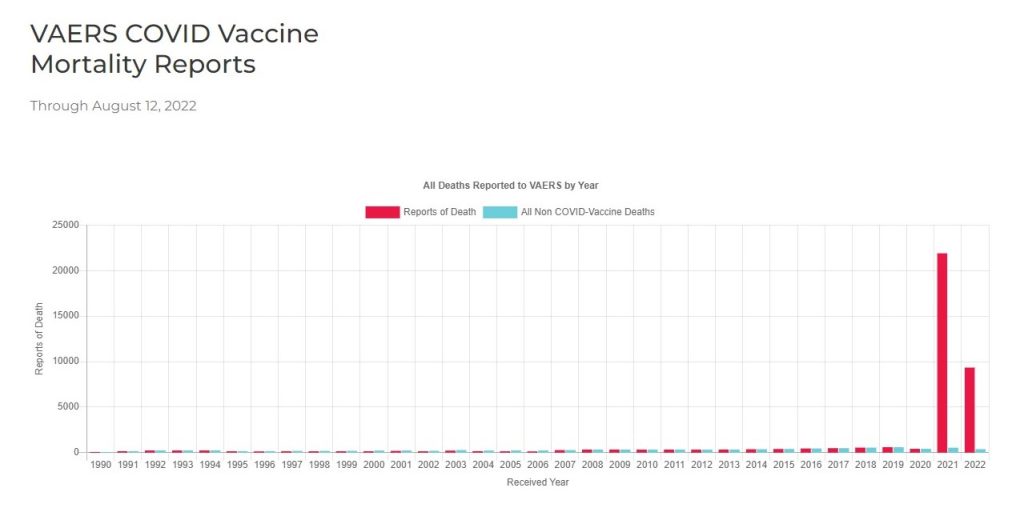
Figure 2. All deaths reported to VAERS following vaccinations since 1990
50. Of particular concern was the observation that some serious adverse events were more likely to occur in younger age groups, i.e. the very groups at lowest risk of severe SARSCoV-2 infection. Major thromboembolic events after AstraZeneca vaccine were quoted in the MHRA’s Yellow card summary report, August 202165 at 20.2 per million doses in those aged 18-49 years compared with 11.0 per million doses in those aged 50 years plus. This ultimately led to discontinuation of AZ vaccines in younger adults. However reports of myocarditis following mRNA vaccines were described in much vaguer terms:
“There has been a recent increase in reporting of these events in particular with the Pfizer/BioNTech and Moderna vaccines, with a consistent pattern of cases occurring more frequently in young males and shortly after the second dose of the vaccines.” This information was especially important when considering vaccination of healthy young adults and children.
51. Reports of serious side effects quickly began to appear in the medical literature, ranging from the serious clotting problems with viral-vector vaccines outlined in para 60 below, through to cardiac inflammation in young men following the mRNA vaccines. Neurological and inflammatory conditions were reported and perhaps most worryingly a possible link with aggressive cancers. A compilation listing over a thousand peer reviewed articles reporting adverse events was published in February 2022.66
52. Importantly, the products were not tested for prevention of infection and transmission; an effect would be unlikely given the vaccines have no effect on the upper airway from where the virus is shed or received. Moreover, given the general brevity of protection, a lasting effect would have been even less likely. This is highly relevant when much of the marketing to healthy children and young adults was predicated on ‘don’t kill your granny’ or the ‘no one is safe until everyone is safe’ messages.
53. The promotion of these products simply as “Safe and Effective” was often conducted in a misleading way. In particular, it is worthy of note that the Association of British Pharmaceutical Industries (ABPI) and the Prescription Medicines Code of Practice Authority (PMCPA) Code of Practice for the pharmaceutical industry.67 Clause 6.1 states: “Referring only to relative risk, especially with regard to risk reduction, can make a medicine appear more effective than it actually is. In order to assess the clinical impact of an outcome, the reader also needs to know the absolute risk involved. In that regard, relative risk should never be referred to without also referring to the absolute risk.” In addition, Clause 6.4 of this code states: “Information and claims about adverse reactions must reflect available evidence or be capable of substantiation by clinical experience. It must not be stated that a product has no adverse reactions, toxic hazards or risks of addiction or dependency. The word ‘safe’ must not be used without qualification”. The jurisdiction and authority of the PMCPA extends only to pharmaceutical companies, including those marketing covid vaccines, and their employees, however, the general principles set out in these clauses are sound. Yet repeatedly, the government and the media published claims of 95% efficacy, with no reference to the low likelihood of catching Covid-19 in any given wave resulting in an absolute risk reduction of only 2-3%. Moreover, use of the word ‘Safe’ implies knowledge beyond the available data. In truth a more honest assessment was, “We hope the vaccines are safe and we think they are effective”.
54. Informed consent was also a casualty of the rapid vaccine rollout. General Medical Council (GMC) guidance68 on obtaining consent is very clear. The second key pillar of informed consent states: “Decision making is an ongoing process focused on meaningful dialogue: the exchange of relevant information specific to the individual patient.”
Members of the CCVAC were particularly concerned at the push to vaccinate the whole population, with no individualised informed consent. We wrote to the GMC about this and had a helpful reply.69 We also wrote to the Medical Defence Union regarding the same concerns.70 Both the GMC and the MDU in their replies acknowledged the difficulties of obtaining fully informed consent.
VACCINE TRIALS IN CHILDREN
55. The initial trials recruited only those aged 16 years and over. However, all the main manufacturers commenced trials in children within months of their Emergency Use Authorisations for adults, even though the very low risk to children from Covid-19 was already established and well before any long-term vaccine safety data on adults was available.
56. This raises serious questions about compliance with the Helsinki Declaration. The Medicines for Human Use (Clinical Trials) Regulations 200471 enacted the Declaration of Helsinki into UK law, and stipulates that “The rights, safety, and well-being of the trial subjects are the most important considerations and shall prevail over interests of science and society.” Moreover, the Universal Declaration on Bioethics and Human Rights (2005)72 states that, “Scientific research should only be carried out with the prior, free, express and informed consent of the person concerned”. Article 7, referring to people without the capacity to consent, states, “authorization for research and medical practice should be obtained in accordance with the best interest of the person concerned” and that “research should only be carried out for his or her direct health benefit”.
57. UK guidance on research in children has been extensively reviewed, leading to detailed guidance from the Nuffield Council on Bioethics,73 endorsed by the Royal College of Paediatrics and Child Health (RCPCH). Children and others unable to give informed consent have particular protection under international law. Research can only be undertaken when the child or vulnerable adult has a possibility for personal benefit. Consent cannot be given on their behalf (i.e. by parents or carers) for research aimed at a benefit to wider society. In applications to the Research Ethics Committee and the Health Research Authority, there is a specific question about Helsinki compliance. But a tick in the box is not evidence of compliance. Moreover, the recruitment processes for the trials often included comments about ‘helping’ to advance knowledge or develop vaccines or other general societal benefits.
58. In February 2021, Oxford University vaccine development group began advertising on Twitter for children aged 6-15 to join a trial of the AstraZeneca viral-vector vaccine.74 As a retired paediatrician, I was extremely surprised to see trials being started on young children at minimal risk from Covid-19 at a time when the adult trials were still in progress. I therefore wrote directly to Professor Pollard, who was the chief investigator.75
He replied immediately with the open admission that he didn’t know the vaccines were safe for children. This was particularly concerning given Professor Pollard’s position as Chairman of the JCVI. He and his fellow principal investigator Professor Adam Finn, also a JCVI member, were unable or unwilling to provide me with the protocol or information leaflets, though these were provided to me by the Berkshire Research Ethics Committee. They are now available in the Clinical Trials website, but the lack of transparency at the time of trial recruitment should be of concern.
59. Professor Pollard was clear to me in a subsequent Zoom call, that this was a preliminary study which if it looked promising would lead to a full-sized phase 3 trial, and there was no likelihood of children receiving Covid vaccines for at least a year.
60. It was somewhat ironic that, less than 4 weeks after children began joining the Oxford AstraZeneca trial, the first death of a young adult with a stroke due to a dangerously low platelet count following an AZ vaccination was reported from Austria.76 This was followed a few days later by a death in Denmark, which immediately suspended the AZ vaccine, followed shortly by countries across Europe and as far away as Indonesia.77 A month later, on 7th April 2021, the JCVI advised against use of AZ vaccine for under-30s.78 By 7th May this advice had been extended to under 40s.79 Vaccine-Induced Thrombotic Thrombocytopaenia (VITT) was added to the patient information leaflet in summer 2021. The propensity for adenoviral–vector products to cause this had been first reported in 1999.80 but warnings had been ignored. The Oxford children’s trial was temporarily suspended, and recruitment was stopped on 17th April.81
61. This whole episode highlights why research on new drugs for children is normally delayed by several years until adult trials are fully completed, analysed and published.
62. Of note, the AZ patient information leaflet for 16-17-year-olds was amended on 27th May, after recruitment had been suspended. Where it had previously stated, “The data from this study may be used to support further larger scale trials in children, the results of which may be used by AstraZeneca to support approvals of this vaccine for use in children in the future”, the updated version states, “The data from this study may potentially only benefit a small group of children at high-risk of COVID-19 disease in the UK or children in other countries.” A whole section on the clotting adverse events was also added. However, the section called What are the advantages of taking part states, “At the end of the study, if you received the MenB vaccine [i.e. the control group], you will be offered two doses of ChAdOx1nCoV-19 vaccine if it is approved for use in your age group and you are not eligible under a national immunisation programme.” The wording of this section was not altered from previous versions, although it was known that the AZ vaccine had already been withdrawn in the UK for all under 40s.
63. Follow-up results for the 262 children recruited to the AZ trial were published in 2022,82 and included: “Amendment to Study Design: During the recruitment window for participants aged 6–11 years, the UK Government was advised by the Joint Committee on Vaccination and Immunisation that individuals younger than 30 years who had not yet received a first dose of the ChAdOx1 nCoV-19 vaccine should be given an alternative COVID-19 vaccine following safety concerns of vaccine-induced thrombosis and thrombocytopenia syndrome. This recommendation led to the cessation of further recruitment of participants aged 6–11 years, although recruitment targets for participants aged 12–17 years had already been met. Second-dose vaccination was then paused pending an MHRA review. Only participants aged 12–17 years randomly assigned to the 28-day interval groups had received second doses by this time. By April, 2021, further safety data in adults who had received second doses of ChAdOx1 nCoV-19 in the UK became available for review by the MHRA. The MHRA then authorised administration of second vaccine doses to those participants aged 12–17 years randomly assigned to 84day interval groups and to all those aged 6–11 years. As the originally intended day 84 window for second doses had passed, the second dose of vaccine was given to those participants aged 12–17 years randomly assigned to 84-day interval groups and to all those aged 6–11 years at day 112.”
64. It is inexplicable that the MHRA or indeed paediatricians in the participating centres could consider giving more doses to children for a research project, after the risk of blood clotting had come to light.
65. The study reported adverse events in >80% of the children after their 1st dose, including 81% fatigue, 81% headache and 69% feverish. Despite this, they state, “Interpretation: ChAdOx1 nCoV-19 is well tolerated…No safety concerns were raised in this trial.”
66. Meanwhile, Pfizer and Moderna were pressing ahead with trials in children. Pfizer applied to the MHRA for an extension to their licence to include 12-15-year-olds. At the point when the MHRA gave conditional marketing authorisation to Pfizer, the trial contained 1131 vaccinated adolescents who were followed for a total of two months.83
67. There was an over-reliance on comparing serum antibody levels, so-called ‘immunobridging’ as a proxy for efficacy in all the children’s trials. For the 12-15s, antibody responses were compared with those seen in 16-25s and on that basis the vaccine was assumed to be effective. This was despite the Pfizer documentation for the FDA approval stating, “a specific level of neutralizing antibodies has not been established to correlate with protection, and other aspects of the immune response elicited by the vaccine may also be important”. There were indeed fewer cases of SARS-CoV-2 infection in the vaccinated group but, “There were no reports of severe COVID19 cases (and no cases of MIS-C) in participants 12-15 years of age.”. Not surprisingly, there were no deaths in either group. The lack of any severe Covid-19 cases in either the vaccinated or the placebo group underlines the futility of such a study.
68. The study did not include enough children to claim any kind of ability to determine a safety signal. There were 4 severe adverse events in 1131 vaccinated children (0.4%) versus 1 in the 1129 receiving the placebo (0.1%). These numbers are too small for statistical significance, confirming that the trial was grossly underpowered for assessing safety. The adult vaccine trials recruited over 20,000 volunteers.
69. Trials for 5-11s. These used a lower dose of mRNA vaccine and again recruited very small numbers, with the Pfizer trial84 recruiting 1517 for vaccination and 751 for placebo. As with the 12-15s study, “No cases of severe Covid-19 or MIS-C were reported.” Efficacy against (mild) symptomatic Covid-19 was reported as 90.7% (95% CI, 67.7 to 98.3) but already by 6 weeks after the second dose was waning steeply. Already the bar for efficacy was being lowered – see page 144 of the study protocol85 “Amendments 4 on 29 September 2021 Revised the success criterion for the efficacy hypotheses to the lower limit of 95% CI >30%, in response to regulatory feedback”.
70. Trials for 6 months to 4-year-old children: the Pfizer trial86 for the preschool age group was even less adequate. The investigators chose a smaller dose of 3mcg still with the same 2-dose schedule as for older children and adults. But after the first dose, vaccine efficacy had become negative, i.e. vaccinated children were more likely to become infected than the placebo group. There was a short-lived upturn in efficacy after the 2nd dose. By then, as with the adult trials, the sponsors had broken the code and vaccinated most of the controls and they subsequently were forced to recruit extra children for a third dose.
| Time post dose | Pfizer BioNTech (number) | Placebo (number) | Vaccine efficacy (95% confidence) |
| Dose 1 to Dose 2 | 13 (1027) | 5 (524) | -29.7% (-365,+57) |
| 0-7 days post dose 2 | 3 (1002) | 3 (517) | 48.4% (-285,+93) |
| 7 days post dose 2 to before dose 3 | 80 (998) | 48 (512) | 14.5% (-25,+41) |
| 0-7 days post dose 3 | 1 (336) | 0 (147) | -100% (undefined) |
| ≥7 Days after Dose 3 | 1 (277) | 2 (139) | 75.5 (-370,+99.6) |
Table 2. COVID-19 Occurrences 6-23 month cohort
71. By the time they applied for and obtained MHRA approval, only “Approximately 32.7% of participants 6-23 months of age had ≥2 months of blinded follow-up time after Dose 3.” The much quoted 75% efficacy shown in Table 2 above, was based on only 3 cases, 2 in the placebo group and 1 in the vaccine group with confidence intervals for efficacy as low as minus 370%. Had they included the case in the first 7 days post vaccination, then efficacy would have been non-existent.
72. Adverse events were rife: “The most commonly reported solicited ARs after any dose for participants 6-23 months of age were irritability (68.4%), drowsiness (41.3%), decreased appetite (38.6%), and tenderness at the injection site (26.4%).” But perhaps more seriously, “Seven cases in participants 2-4 years of age met the criteria for severe COVID-19: 6 in the BNT162b2 group, of which 2 cases occurred post unblinding, and 1 in the placebo group.” This hardly suggests efficacy, it could even represent antibody dependent enhancement (ADE). Twelve children had multiple episodes of infection, 10 of whom were vaccinated versus 2 placebo.
73. The Moderna trial87 for this age group was also woefully inadequate with an estimated vaccine efficacy (i.e. relative risk reduction) against Covid-19 of 36.8% (95% CI, 12.5 to 54.0) among 2-to-5-year-olds and only a 2.5% absolute risk reduction. In the younger group prevention of asymptomatic infection was at a mere 3.8% with confidence intervals from -111 to +53%
74. Adverse events were significant. The trial abstract states, “Adverse events were mainly low-grade and transient, and no new safety concerns were identified.” but in the full results they reported within 28 days of injection “In the cohort of children 6 to 23 months of age, eight serious adverse events occurred in the mRNA-1273 group, and none occurred in the placebo group.” Moreover, in the Supplementary Appendix88 they report ongoing serious adverse events beyond the 28-day window, with only 1(0.17%) in the placebo group against 15 (0.78%) in the vaccinated children in the younger age group. This included a one-year-old child with new onset type 1 diabetes occurring 37 days after the second dose. It was notable that serious adverse events were more common in the younger age group, for whom the dose per kg body weight would be higher.
INITIAL PLANS, THEN MISSION CREEP
75. Kate Bingham, head of the UK Vaccine Task Force, said89 in October 2020: “People keep talking about ‘time to vaccinate the whole population’, but that is misguided”,
“There’s going to be no vaccination of people under 18. It’s an adult-only vaccine, for people over 50, focusing on health workers and care home workers and the vulnerable.” The then Secretary of State for Health confirmed this in the Commons on 10 November 2020,90 “The vaccine will not be used for children. It has not been tested on children. The reason is that the likelihood of children having significant detriment if they catch covid-19 is very, very low. This is an adult vaccine for the adult population.”
76. But by February 2021, SAGE member Professor John Edmunds was telling Andrew Marr on BBC, that “we can all spread the virus, and so until we’ve all been vaccinated and I include children here, then there is going to be a significant risk of a resurgence …I think there’s an argument for turning to children as fast as we can”.91 In other words, he was already suggesting a policy which contravened the requirement for a direct benefit to the child.
77. By March 2021 there were leaks to the press even before the vaccines were approved for children, that the government would be starting the rollout to children in August.92 At around this time (i.e. 3 months before the vaccines were approved for children), teaching materials began circulating in London schools, which applied both peer pressure and fear. Produced by the Stephen Hawking Foundation,93 the opening slide asks, “If you were offered a COVID vaccine today, would you take it? Hands right up for YES, down for NO, in the middle for ‘I’m not sure’ ”, but in the image, all the children have their hands up. One image (slide 11) showed particularly frightening images of children with smallpox, tetanus and polio, immediately followed by a slide asking, ‘When can I have my vaccine?’
78. In May, Geoff Barton, general secretary of the Association of School and College Leaders (ASCL), said,94 “Education leaders would be willing to help facilitate a vaccine roll-out at schools around the country”…“I think there will be a sense of schools wanting to step up and play their part and explain to children why having the vaccine is important during assemblies and in tutor time.”… “mass vaccinations among children could be a way to end the system of controls that are currently in place in schools, including face masks in the classroom, social distancing and bubbles.”… “vaccinating children at school could result in higher take-up because pupils would not want to feel socially isolated by refusing to have the jab.”… “The peer pressure of seeing that your friends are lining up to do it is likely to make the overall numbers taking up the vaccine higher”. Using peer pressure is in clear contravention of the principles of informed consent. On the same day, Professor Linda Bauld, from Edinburgh University, also supported the move, saying,95 “I think the reason to vaccinate children… is really to add to herd immunity.”
79. Not everyone shared this view. An Editorial in the British Medical Journal in May 202196 opened with, “the value of childhood vaccination against respiratory viruses in general remains an open question for three reasons: the limited benefits of protection in age groups that experience only mild disease; the limited effects on transmission because of the range of antigenic types and waning vaccine induced immunity; and the possibility of unintended consequences related to differences in vaccine induced and infection induced immunity.”
80. No-one in any official capacity would appear to have questioned the ethics of encouraging children to be given a vaccine they didn’t need, in order to protect adults. Nor did they seem to understand that there was no evidence that the vaccines prevented transmission and therefore that this policy would work or that it would have any effect on herd immunity.
AUTHORISATION PROCESS & POLICY MAKING RE VACCINES FOR CHILDREN
81. In spring 2021, Pfizer submitted an application for their conditional marketing authorisation to be expanded to cover 12-15-year-olds. At that point, the CCVAC group sent our first detailed letter to the MHRA, drawing their attention to a number of concerns, both medical and legal.97 The JCVI were copied into the letter and replied promptly advising me to contact the MHRA who were responsible for safety analysis. The MHRA failed to reply within their stated 18-day framework despite a personal phone call to Dr June Raine’s secretary, who promised to expedite a response. Dr Raine eventually sent a very bland reply, 2 hours after the authorisation had gone ahead. She stated that they had reviewed all the data in detail and were confident that the vaccine would be ‘safe and effective’ for this younger age group. We sent a further reply on 8th June, highlighting specific questions which had not been addressed. A further reply from Dr Raine in August again failed to provide any detailed evidence for the safety of the Pfizer vaccine relative to the extreme mildness of SARS-CoV-2 infection in children. Our letters and her replies are shown in full in Appendix A.
82. It was already clear by then from VAERS,98 EMA and Yellow Card data that severe adverse reactions were being reported at much higher rates than with any previous vaccines, yet the MHRA appears only to have looked at data from Pfizer itself when deciding whether to give a conditional marketing authorisation. The Public Assessment Report99 states in the Introduction, “This report is based on the information provided by the company in a rolling data submission procedure and it covers the authorisation for temporary supply of BNT162b2.”
83. The Moral and Ethical Advisory Group (MEAG)100 was set up somewhat presciently in 2019, as part of pandemic preparedness planning, their remit being: “provide independent advice to the UK government on moral, ethical and faith considerations on health and social care related issues as they occur. This advice will be used to inform management of health-related incidents including but not limited to pandemic flu.” At their first meeting on 10th March 2020 they discussed ‘The Ethical Framework for Adult Social Care’. At their next meeting the following week, a cabinet official “outlined the significant challenges and difficult decisions that lie ahead”. By April they had written a report on funeral arrangements and specifically commented that “Members felt that differing views and the wide range of areas of expertise were a positive element for the Group, which enables fruitful discussions, and thus constructive advice provided on issues posed.”
84. They continued to meet regularly throughout the first year, reporting directly to the DHSC and covering a wide range of topics including that of possible mandatory vaccination for care home workers. At their meeting in March 2021,101 they specifically requested input regarding children’s vaccination including asking for their views to be sought in advance of any decision. A meeting was set up for June but was cancelled as they were told that the JCVI would not be recommending it. They then had no further meetings during the critical time when the JCVI was deliberating. At their September meeting, just before the CMOs’ final decision, Covid-19 was not even on the agenda.
85. Given the MHRA authorisation, we wrote urgently to the JCVI102 and the Chief Medical Officer, with copies to the Nuffield Council on Bioethics. It appeared that MHRA were saying that they had merely ‘authorised’ their use, but it would be up to the Government in consultation with the JCVI to make the final decision on deployment. We therefore specifically requested the JCVI to make their own safety assessment rather than relying on the MHRA who clearly had not evaluated anything beyond the data offered them by Pfizer.
86. JCVI issued a statement on 19th July 2021 stating clearly that they did not consider the benefit:risk ratio for under 18s to be favourable.103 They commented on the reported adverse events, which in the press briefing were described as ‘extremely rare’ but in the full statement were described as ‘rare’.104 In their statement, they clarified the position already outlined by the Royal College of Paediatrics and Child Health (RCPCH), namely that those children with comorbidities that put them individually at high risk from Covid-19 were already able to receive the vaccines ‘off-label’ in consultation with their paediatrician. The RCPCH recommendation was for those children with a combination of severe neuro-disability and respiratory problems to be considered for vaccination, whilst explaining to parents the lack of any trial data for these high-risk groups.
87. It was notable that the 19th July statement advised that Covid vaccination could begin 3 months prior to the child’s 18th birthday. The rationale for this became clearer later that day, when Boris Johnson announced the plan to introduce mandatory vaccination for nightclub attendance, see para 25 above. The 3-month run-in would allow a teenager to get 2 doses and the required delay 3 weeks post dose and still be in time for an 18th birthday night club trip. It was at about this time that vaccine pop-up centres began to appear at venues such as the Ministry of Sound nightclub, Thorpe Park Theme Park and Charlton Athletic Football Club (even including free football tickets for the first 1000 vaccine recipients). Thus the combination of carrot and stick was embedded.
88. The minutes of an Emergency JCVI meeting in August reveal this was held at the request of the CMO to reconsider their decision105 on vaccination of under 18s. It is not clear where this political pressure originated. The JCVI modified its advice the following week, to provide a single dose only, for 16-17-year-olds. Although not stated, it seems likely that the choice of a single dose stemmed from awareness of myocarditis (heart inflammation) particularly in younger males after the second dose.
89. Reports had already come from Israel regarding myocarditis in adolescent boys following Pfizer vaccination, first reported in April 2021 and confirmed with further cases over the next two months.106 The Public Health team at Ben Gurion University kindly arranged to send me the same slide set that had been provided to the JCVI from a report to the Israeli Ministry of Health. Their data on myocarditis after the Pfizer mRNA vaccine very clearly demonstrated the inverse relationship to age, as shown in Table 2 with a more than ten-fold higher incidence in the 16–19-year-old males than in the over 30s. I followed this up with a Zoom call which confirmed their findings. They noted that symptoms had settled quickly but they had not performed cardiac MRI scans to seek for evidence of scarring.
| Age & gender | Dose 1 | Dose 2 | |
| Males | 16-19 | 1 in 90,511 | 1 in 6,230 |
| 20-24 | 1 in 132,724 | 1 in 10,463 | |
| 25-29 | No cases | 1 in 25,304 | |
| 30+ | 1 in 393,9418 | 1 in 71,785 |
Table 2. Incidence of myocarditis in young males per vaccination doses. Israel, August 2021
90. In August 2021, an American multicentre study of children with post-vaccination myocarditis was published,107 reporting on 63 patients aged 13-20 presenting to 16 cardiology centres with cardiac symptoms following an mRNA Covid vaccine (all but one were after the second dose); 43% required admission to intensive care. The children underwent cardiac MRI scanning which revealed significant changes in no fewer than 88% of those studied. Although symptoms settled quickly, the authors concluded, “Close follow-up and further studies are needed to understand the long-term implications and mechanism of these myocardial tissue changes.”
91. The JCVI committee met again, and members were clearly concerned about myocarditis in adolescents. They undertook a Zoom call with cardiologists from the US and they minuted a wish for at least a further 6 months in order to look at follow-up data from this group.108
92. I undertook a Zoom call with Dr Supriya Jain, from New York Medical College, who was lead author on the American study. A senior colleague from Oregon also joined the meeting. They confirmed that they had been on the call to the JCVI. They noted that although the children in their study had relatively mild symptoms which were settling, they had been surprised by the level of abnormalities. The test they used, Late Gadolinium Enhancement (LGE), is known to be predictive of late deaths in the first 6 years following viral myocarditis.109
93. Dr Jain has provided some early follow-up scan results suggesting that by 6 months later, approximately one third had normalised, one third had improved and one third had continued significant changes. It is this sort of data that the JCVI sought. Dr Jain is now in receipt of an FDA 5-year grant to study the long-term implications of vaccine-induced myocarditis.110 [Update: 07/09/2024, Dr Jain et al have just published a 6-month followup of 333 children and young adults with Vaccine-Associated Myocarditis and found that 60% had persistent changes of LGE, indicative of ongoing cardiac damage.111]
94. Following the JCVI’s emergency call with the various cardiologists, they published a statement on 3rd September112 in which they concluded, “The margin of benefit, based primarily on a health perspective, is considered too small to support advice on a universal programme of vaccination of otherwise healthy 12 to 15-year-old children at this time. As longer-term data on potential adverse reactions accrue, greater certainty may allow for a reconsideration of the benefits and harms. Such data may not be available for several months.” They went on to say, “JCVI is constituted with expertise to allow consideration of the health benefits and risks of vaccination and it is not within its remit to incorporate in-depth considerations on wider societal impacts, including educational benefits.” This is a surprising comment, given that they had specifically mentioned impact on transmission in schools in previous statements.
95. The JCVI report went on, “The government may wish to seek further views on the wider societal and educational impacts from the chief medical officers of the 4 nations, with representation from JCVI in these subsequent discussions. There is considerable uncertainty regarding the impact of vaccination in children and young people on peerto-peer transmission and transmission in the wider (highly vaccinated) population. Estimates from modelling vary substantially, and the committee is of the view that any impact on transmission may be relatively small, given the lower effectiveness of the vaccine against infection with the Delta variant. Delivery of a COVID-19 vaccine programme for children and young people is likely to be disruptive to education in the short term, particularly if school premises are used for vaccination and there is potential for a COVID-19 vaccine programme to impact on the efficiency of roll-out of the influenza programme. Adverse reactions to vaccination (such as fevers) may also lead to time away from education for some individuals.”
96. It was at this point that the CMOs deliberated and 10 days later came up with a statement113 that they were recommending vaccination of 12-15s with claims of a mental health benefit. This was predicated around a vaccination programme reducing school disruption and hence the secondary impact of school closures on children’s mental health. There were two major fallacies with this argument:
a. First and most importantly, the vast majority of school disruption had been produced not by Covid itself (which for most children is very mild) but by the government policy of school closures and the ongoing quarantining of healthy contacts. The latter policy was known to be leading to an average of 30 children sent home for each positive test. On the 15th July 2021, 17.9% of 11-16-yearolds were absent from school, the majority as class or year-group contacts of a positive case. The policy was extremely disruptive, no data were provided to support it and it was discontinued on 19th July just 2 days before the end of the summer term.114
b. The second fallacy lay in the calculation of schooling saved by the vaccination programme. The government published a supportive paper.115 This used models to estimate potential school days saved as between 10,000 and 290,000. This would be across a secondary school population of over 3 million pupils and the lower estimate would be less than the time taken for children to queue up for their vaccines. The CMOs admitted they had not factored in any time lost for vaccine adverse events, despite the known systemic side effects of fatigue, headache and fever occurring in the children’s trials, let alone any more serious adverse events.
97. By mid-September 2021, 78% of 15-24-year-olds and 36% of 5-14s were already estimated to have been infected.116 Natural immunity was already known to be robust117 and vaccine side effects to be worse if already immune. One study from Israel found that “Short-term severe symptoms that required medical attention were found in 6.8% among the post-infected individuals, while none were found in the infection naïve population”.118 Professor Chris Whitty was questioned by the Education Select Committee, who suggested to him that the models of the educational disruption potentially saved were likely to be a vast overestimate, given the changes to quarantine procedures. He was also asked about only vaccinating the non-immune but replied that this would be too complicated for a routine programme “You could do a theoretical thing where you say if you are a middle-class white boy, we will do a blood test, work out if you are serology positive and if you are, we won’t do a vaccination. I am not convinced that feels to me like an effective public health intervention”.119 He had clearly forgotten that in the past, the schools’ routine BCG immunisation programme had involved skin testing every child with a Mantoux or Heaf test which had to be read 48-72 hours later, whereas SARSCoV-2 immunity could easily have been checked on the day using a rapid saliva antibody test.
98. Also, worryingly for parents, there was emphasis on children being able to give their own consent if a health professional deems them to be Gillick competent.120 In the context of queuing up in a busy Secondary School with all your peers (whose parents had consented), it is not hard to see how choices might involve a degree of coercion.
99. The decision-making for the 5-11-year-olds was equally confusing. The MHRA first approved the new children’s lower dose mRNA vaccines in December 2021, following an EMA approval system.121 But it appears JCVI members were in no rush to follow countries such as the US, Israel and Australia into vaccinating this younger cohort, for whom serious illness from SARS-CoV-2 infections was vanishingly rare. Eventually, in February 2022 they recommended a ‘non-urgent offer’ to be implemented in April of that year.122 The statement included the following, “Data in adults indicate that vaccine effectiveness against symptomatic infection due to Omicron (Pfizer-BioNTech vaccine) wanes over time from around 70% shortly after 2 vaccine doses to around 25% after 10 weeks and 10% after 20 weeks.”
100. They go on to say, “Most children aged 5 to 11 have asymptomatic or mild disease following infection with SARS-CoV-2. Some may experience post-COVID-19 symptoms lasting longer than a few days. Children aged 5 to 11 years who are not in a COVID-19 clinical risk group are at extremely low risk of developing severe COVID-19 disease. It is estimated that over 85% of all children aged 5 to 11 will have had prior SARS-CoV-2 infection by the end of January 2022, with roughly half of these infections due to the Omicron variant. Natural immunity arising from prior infection will contribute towards protection against future infection and severe disease.”
101. They continued, “The impact of vaccination on school absences was indeterminate; the balance between school absences due to reactions following vaccination versus school absences avoided due to prevention of infection is highly influenced by the uncertain timing of any future wave of infection and of the vaccination programme…Vaccination of children aged 5 to 11 who are not in a clinical risk group is not expected to have an impact on the current wave of Omicron infection. The potential benefits from vaccination will apply mainly to a future wave of infection; the more severe a future wave, the greater the likely benefits from vaccination. Conversely, the less severe a future wave, the smaller the likely benefits from vaccination.”
102. It is hard to comprehend the logic of using a vaccine that was developed against a previous variant (Wuhan strain) and was acknowledged would be less effective against the then current Omicron strain and also acknowledged to wane rapidly, and yet to hope it might give protection against some unknown future strain. It was particularly illogical to recommend giving that ‘one-off’ dose in April at a time when circulating coronaviruses were in steep seasonal decline and that would have no persisting benefit by the time of any potential winter wave.
103. A further letter to the JCVI123 was signed by 650 health professionals and presented at their office 8 days later. Specific questions were asked about the current benefit:risk balance, given the fact that most children already had good natural immunity and the mildness of the prevalent Omicron variant which, moreover, was poorly covered by the vaccine being deployed.
104. When it came to the 0-4s, ‘First do no Harm’ finally prevailed and despite conditional marketing authorisation by the MHRA, the JCVI declined to recommend the vaccines for healthy preschool children, unlike north America and many countries in Europe.
105. It is notable that the British National Formulary for Children (BNFC)124 currently states for Covid vaccines side effects:
● Rare or very rare: Angioedema; cardiac inflammation; embolism and thrombosis; facial paralysis; Guillain-Barre syndrome; sensation abnormal; visceral venous thrombosis
This is very vague, since there is a huge difference between ‘Rare’ which might be as much as 1 in 1000 and ‘very rare’ which could be as low as 1 in 100,000.
106. Negative efficacy: It became apparent very early on, that vaccine efficacy waned quite quickly. This was obscured by the very short follow-up time of only 2 months used in the adult trials that supported the initial authorisation and led to a system of repeated boosters. A booster was recommended for all adults in autumn 2021 and ongoing 6 monthly boosters for the most vulnerable. Despite this strategy, Covid infections continued in highly-vaccinated populations. There is good evidence of a specific rise in infection risk in the first 7-10 days after vaccination, thus putting family members at increased rather than reduced risk.125 Peaks in infection rates have been seen directly after booster uptake e.g. in Israel.126
107. A large study of healthcare workers in Cleveland127 revealed that infection rates were highest in those who had received the largest number of vaccine doses as shown in Figure 3. The authors later demonstrated this effect was not due to differences in testing or prior infection rates.
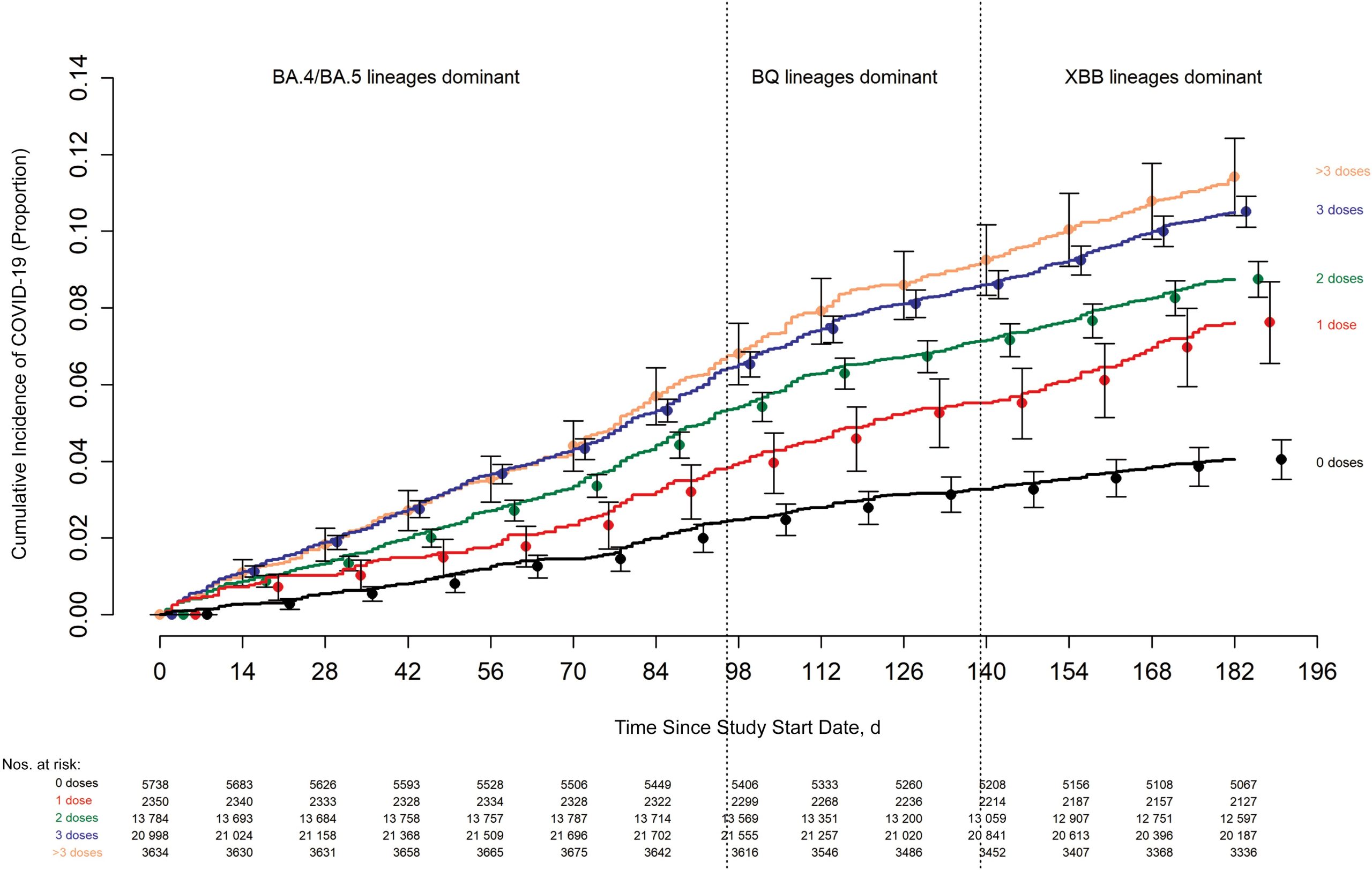
Figure 3. Cumulative incidence of COVID-19 stratified by number of vaccine doses. (Day 0 was 12 September 2022, when the bivalent vaccine was first offered to employees)
108. With the children’s vaccines, it appears that efficacy wanes even more rapidly, perhaps because in an attempt to reduce side-effects, lower doses have been used. One study from New York of 5-17-year-olds128 showed that for the 12-17-year-olds (the orange bars in Figure 4. below), vaccine efficacy had fallen from 76% to 46% within 6 weeks of their second dose. For 5-11-year-olds (blue bars in Figure 4) who received a lower-dose vaccine, the decline was even more rapid falling to negative by 5 weeks after their second dose, i.e. making them more likely to acquire infection than the unvaccinated group. Note the dashed horizontal line at RR=1 indicates a result where vaccine and placebo effects are equal, values above 1 denote vaccine more effective than placebo and levels below one denote that the vaccine is less effective than the placebo.
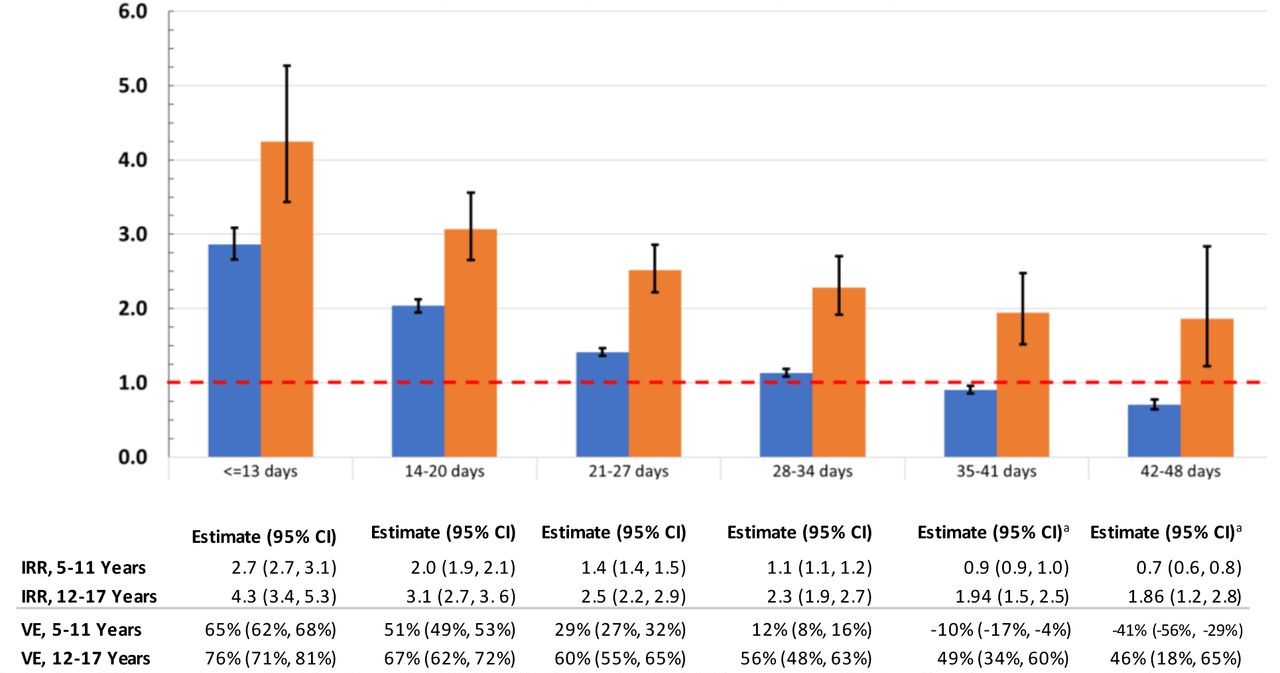
Figure 4. Incidence rate ratios, comparing cases during January 3 – January 30, 2022 for unvaccinated versus children newly fully-vaccinated December 13, 2021-January 2, 2022, by Time Since Full Vaccination (blue columns age 5-11, orange columns age 12-17)
109. Natural immunity: When making decisions around vaccinating children, it was reckless to ignore the benefits of naturally-acquired immunity. From the beginning of the pandemic, it was suggested that no-one knew how long immunity would last and therefore vaccination would be essential for all. Yet vaccination technology has always been based on trying to mimic natural immunity which for a healthy population is normally robust. Studies from US129 showed that the ‘naturally immune’ cohort were at the lowest risk of a subsequent infection regardless of their vaccination status, as shown in Figure 5 below. As expected, a proportion of the non-immune caught Covid during the period of observation but those who already had natural immunity were protected, with or without vaccination. Similar data have been reported from Israel130 “found a statistically significant 13.06-fold (95% CI: 8.08 to 21.11) increased risk for breakthrough infection as opposed to reinfection (P < .001)” and from Qatar131 where the authors reported “Natural infection was associated with stronger and more durable protection against infection, regardless of the variant, than mRNA primary-series vaccination.” A systematic review of 9 studies132 found, “natural immunity in COVID-recovered individuals is, at least, equivalent to the protection afforded by complete vaccination of COVID-naïve populations.” The authors also found,“Vaccination in COVID-recovered individuals provided modest protection from reinfection, but the absolute risk difference was extremely small”. This was highly relevant when considering rolling the vaccines out to children, the large majority of whom had already been exposed to SARS-CoV-2 repeatedly by the time they were offered the vaccine and therefore had nothing to gain from it.
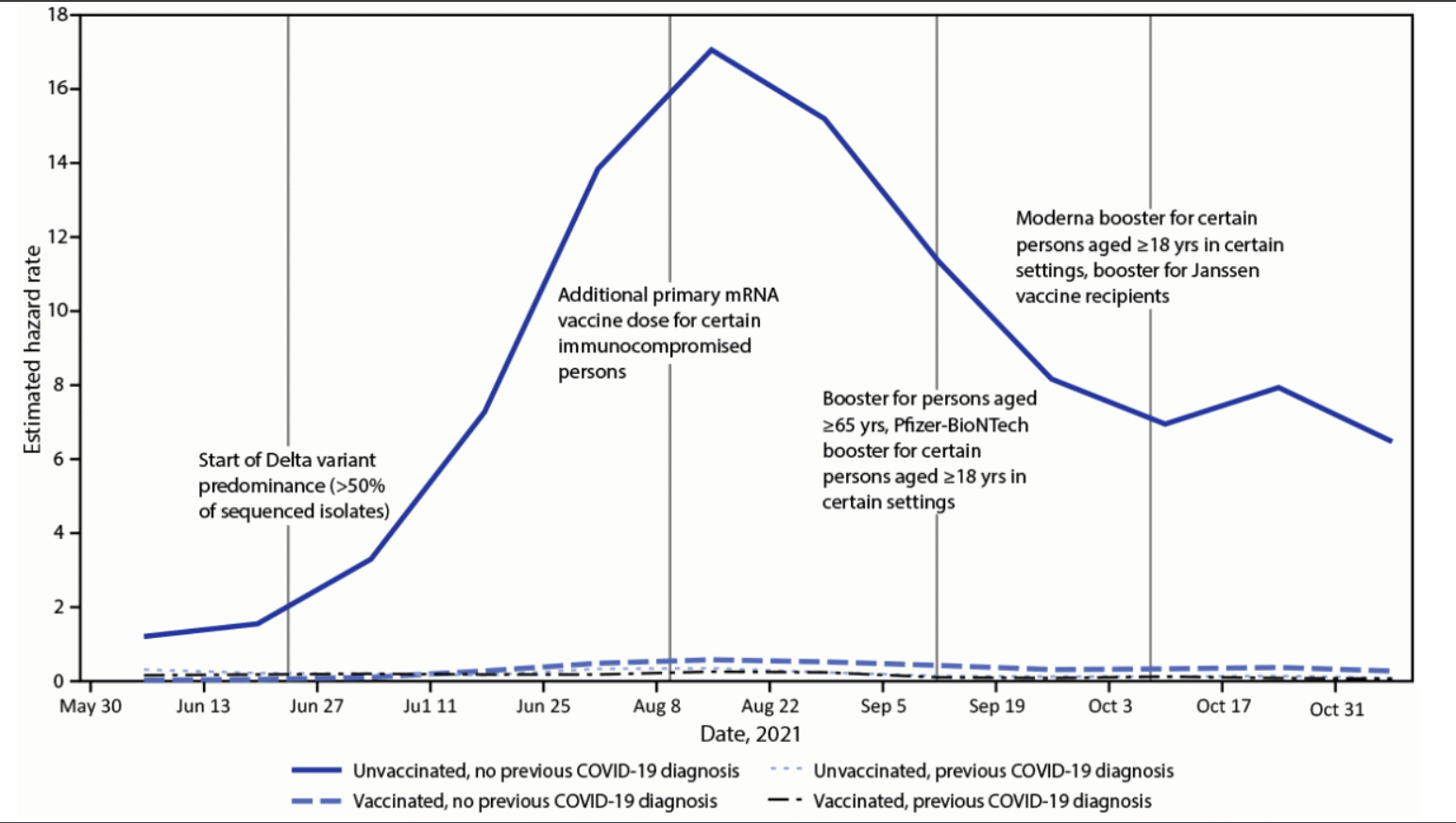
Figure 5. Laboratory-confirmed COVID-19-associated hospitalizations among cohorts defined by vaccination and previous diagnosis histories, May 30–November 13, 2021
110. There appears to have been an assumption by many, that governments and their advisers had no choice but to push ahead with vaccinating children but there are several countries which made different decisions. For example, Sweden133 and Norway134 never recommended it for healthy under-12s, although in Norway it was available at the parents’ request. The Norwegian health authorities also stated that vaccination was not needed for 12-15s if they had already had Covid and they did not actively recommend a second dose because of risk of myocarditis. The Norwegian Institute of Public Health stated that “municipalities should be cautious about organising vaccination at schools, as this may be seen as a strong wish on the part of the authorities for them to get vaccinated, and may be felt to be less voluntary”. In the Netherlands135 it was stated, “The corona shot is not necessary for children without a high medical risk. The risk of them becoming seriously ill from corona is low.”. In Iceland136 vaccines were offered to all children, but it was observed that 107 of the 41,800 vaccinated children suffered an adverse event with 11 severe enough to require hospital admission. They had not a single child admitted to hospital from Covid-19, in their 60,000 child population. In Denmark, the National Director of Health advised children’s vaccines in 2021 but subsequently went on record to say that in hindsight it was the wrong decision.137
FAILURE OF PHARMACOVIGILANCE:
111. Given the novel nature of these vaccines and the lack of long-term safety data, a much more robust system for post-marketing surveillance was required. It is generally agreed that passive reporting systems such as MHRA’s Yellow Card system or the American VAERS will always underestimate adverse events, often by substantial margins.138 A Ministry of Health study from Israel revealed huge under-reporting.139 Moreover, these systems tend to pick up adverse events occurring within the first few days after vaccination and would be unlikely to pick up more gradual impacts on the immune system, particularly if these only arise after multiple doses.
112. The MHRA failed to commission studies to ensure the scaled-up vaccine production for a whole population rollout was of comparable quality to the clinical trial product. The level of integrity of the mRNA vaccines and data on the existence of DNA contamination has only recently emerged. (See para 39 above). The MHRA also failed to insist on completion of those safety experiments that were not completed in time to expedite the initial approvals. Finally, they failed to commission studies as concerns arose about specific safety issues.
113. No formal prospective studies were carried out for myocarditis, despite concerns from abroad. In Hong Kong,140 noting the post-vaccination myocarditis cases from Israel, all paediatricians, cardiologists and emergency medicine specialists were told to look out for cardiac symptoms and report them. They found a risk of 1 in 3000 for adolescent boys after their second dose, so they changed their policy to emulate the single dose in England and Wales. Hong Kong followed up and noted a reduction in myocarditis cases after discontinuing the second dose,141 by which time the JCVI here were switching to two doses.142 Two more letters to the JCVI in November and December 2021 pointing out the ongoing reports of post-vaccination myocarditis generated a reply in March 2022 which contained many statements but not a single supportive reference.143
114. In Thailand, researchers went a step further and organised a prospective study144 in which teenagers at two large secondary schools had ECG and blood troponin levels (a marker for cardiac damage) carried out before their second Pfizer dose; vaccinees then kept a symptom diary card and returned for repeat troponins and ECG on days 3 and 7. The authors found a shocking 29% with symptoms or signs of heart disturbance and 1 in 43 children with evidence of clinical or subclinical peri-myocarditis. A further prospective study from Switzerland found similarly high levels of cardiac involvement with raised troponin levels in 2.8% of patients 3 days post vaccination.145 These are the sort of studies that should have been carried out in the UK.
115. In a study using American VAERS data146 to calculate the risk:benefit balance for adolescents, the authors found that the increased risk of myo/pericarditis outweighed benefits in most scenarios: “Incidence per million after dose two in male patients aged 12–15 and 16–17 was 162.2 and 93.0, respectively. Weighing post-vaccination myo/pericarditis against COVID-19 hospitalization during delta, our risk-benefit analysis suggests that among 12–17-year-olds, two-dose vaccination was uniformly favourable only in nonimmune girls with a comorbidity. In boys with prior infection and no comorbidities, even one dose carried more risk than benefit according to international estimates. In the setting of omicron, one dose may be protective in nonimmune children, but dose two does not appear to confer additional benefit at a population level”.
116. NHS England produced inappropriate guidance regarding further vaccination after myocarditis,147 suggesting further doses could be given once symptoms had settled and have provided no trial data on which to base such advice. Pfizer and Moderna have both belatedly set up 5-year studies which will not report back until 2027. The FDA has also set up a 5-year project. Despite the lack of long-term safety data, the UK continues to offer mRNA vaccines to healthy adolescents who have an immunocompromised household contact.
117. MHRA Yellow Card reports give overall figures and only provide general statements such as ‘more common in younger males’, which lack precision and specificity, making the system unusable for the public or their doctors to guide informed consent. See para 50 above.
118. The US military has the best documented figures for side-effects among mandatorily vaccinated young adults but has not released any significant amount of data officially. A whistleblower has been sanctioned after presenting data that showed significant increases in a number of cardiac problems in 2022 compared with the previous 5-year average.148
119. In September 2022, analysing data from the published Phase 2/3 drug trials, Fraiman et al149 found “Combined, the mRNA vaccines were associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated (95 % CI 2.1 to 22.9)”. That equates to 1 in 800 suffering a severe adverse event, which comes under the definition of ‘uncommon’, rather than the ‘very rare’ often quoted.
120. The quantification of the risk/benefit ratio was calculated for college students (age 1829) and suggested that for every 1 hospitalisation by Covid-19 there are 18.5 serious adverse events from Covid-19 vaccines.150 This was published in late 2022, at a time when students at several North American universities with third-dose Covid-19 vaccine mandates, risk disenrollment if choosing to remain unvaccinated. In another study of 1217s and 18-49s, a comparison of the adverse event rates between Covid-19 vaccines and those for influenza, HPV and the new monkeypox vaccines, the rates of significant adverse events were significantly higher for Covid-19 vaccines, resulting in a rate 19.60fold higher than influenza vaccines, 4.15-fold higher than HPV vaccines and 7.89-fold higher than monkeypox vaccine.151
121. An analysis of data from the Pfizer and Moderna phase 2/3 children’s trials152 found “Severe AEs in vaccine vs placebo recipients in the two oldest populations, but not in the two youngest populations. For the 12-15(17)-year-olds, the combined RR was 3.76 (1.24-11.39[0.6% vs 0.2%])” An excess of 0.4% severe adverse events equates to 1 in 250, which is significantly higher than the risk of severe Covid-19 in this age group. For younger children, there were less problems overall, but there was a significant increase in lower respiratory tract infections in the 6-month to 4year-olds in the vaccinated group “The risk of LRTI was higher in vaccine recipients (3.03 (1.29-7.09[0.6% vs 0.2%])”
122. Excess deaths have been apparent in 15-19-year-old males from summer 2021 as shown in Figure 6.
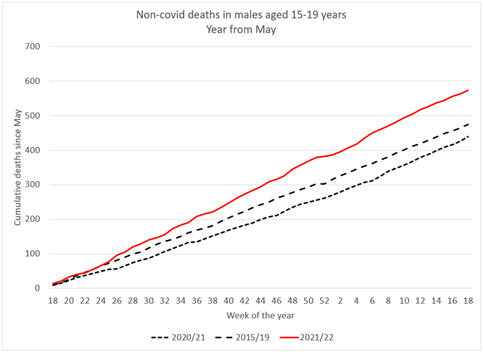
Figure 6. Cumulative non-covid deaths in 2021-22 compared with 2015-2019 & 2020-21
This finding was confirmed by the ONS in the High Court.153 Indeed they suggested the numbers provided were an underestimate because of delays in cases referred to the coroner but said they did not plan to investigate unless the signal increased. It was not clear how many children needed to die before an investigation would be triggered.
123. By August 2022, the MHRA Yellow Cards Covid-19 vaccines report summary included 6 child deaths, the first time any child deaths had been reported.154 Yet it was still deemed ‘Safe and Effective’.
124. The National Child Mortality Database has been in place since 2019. The review for the year ending March 2023155 showed deaths for each age band fell in April 2020-March 2021 compared to 2019-20, but subsequently increased in 2021-22 and increased further in 2022-23, as shown in Figure 7. Overall, deaths of children aged between 1 and 17 years increased by 16% in 2022-23 over the preceding year.
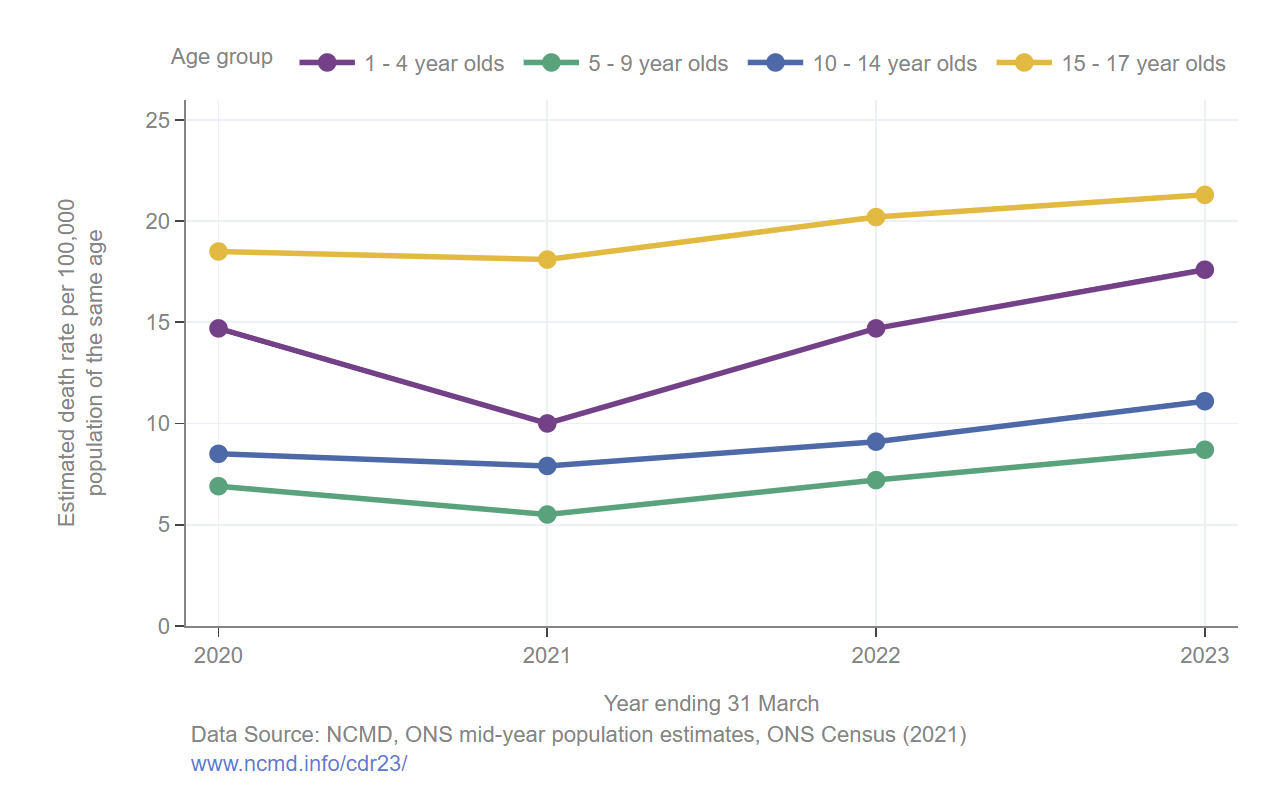
Figure 7. Estimated death rates for children aged between 1 and 17 years per 100,000 population, by age group.
125. Excess non-Covid deaths have continued across most age groups in the UK throughout 2022 and 2023 as shown in Figure 8.
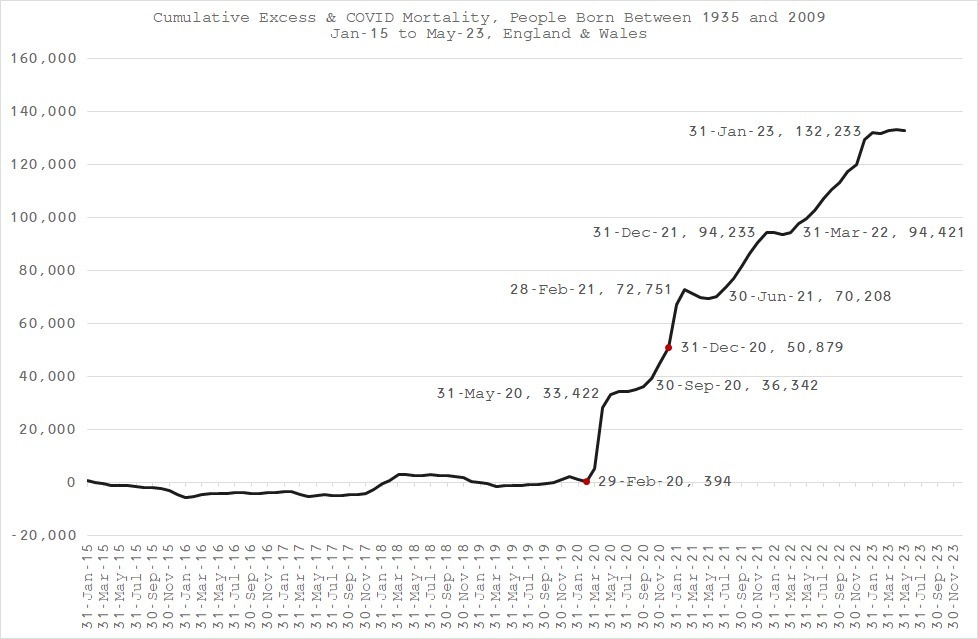
Figure 8. Cumulative Excess all-cause deaths in 11-85s in England & Wales (ONS data)
126. Data from the Office for Health Improvement and Disparities shows the worst-affected group by age is 50–65-year-olds, and the predominant cause is ‘circulatory’, see Figures 9 and 10.156
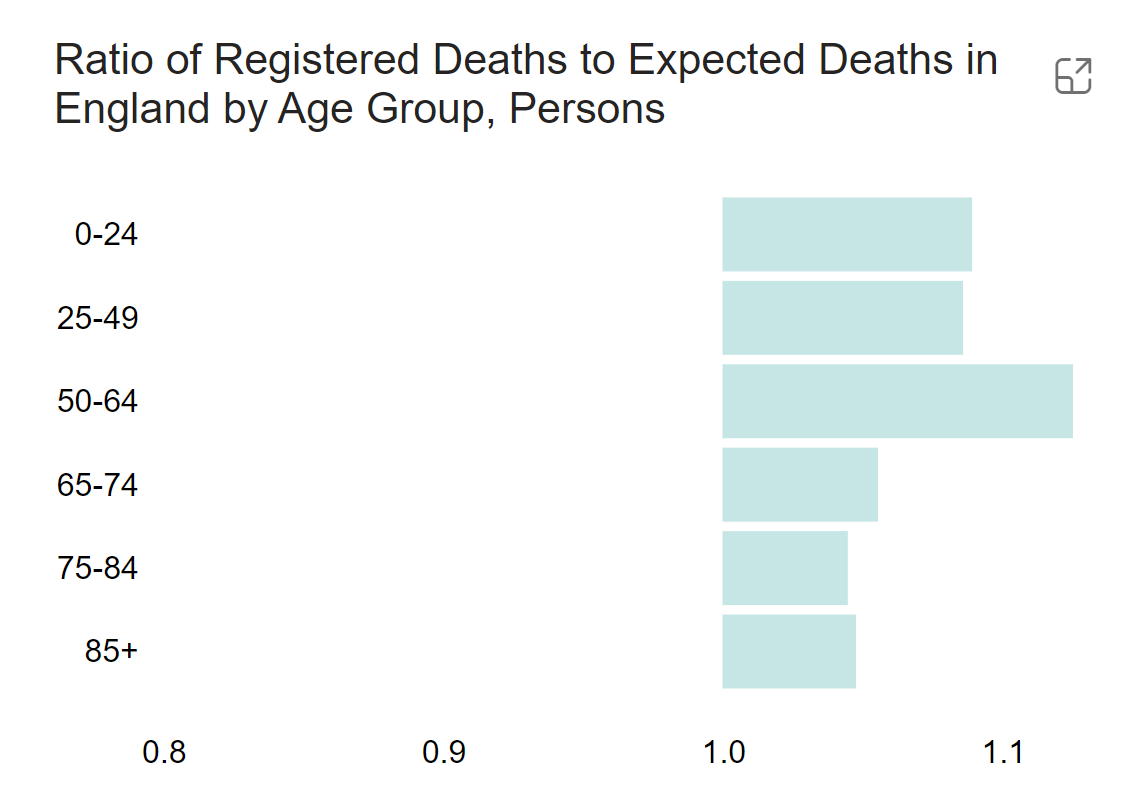
Figure 9. Ratio of actual deaths to expected deaths in England by age bands since 2022
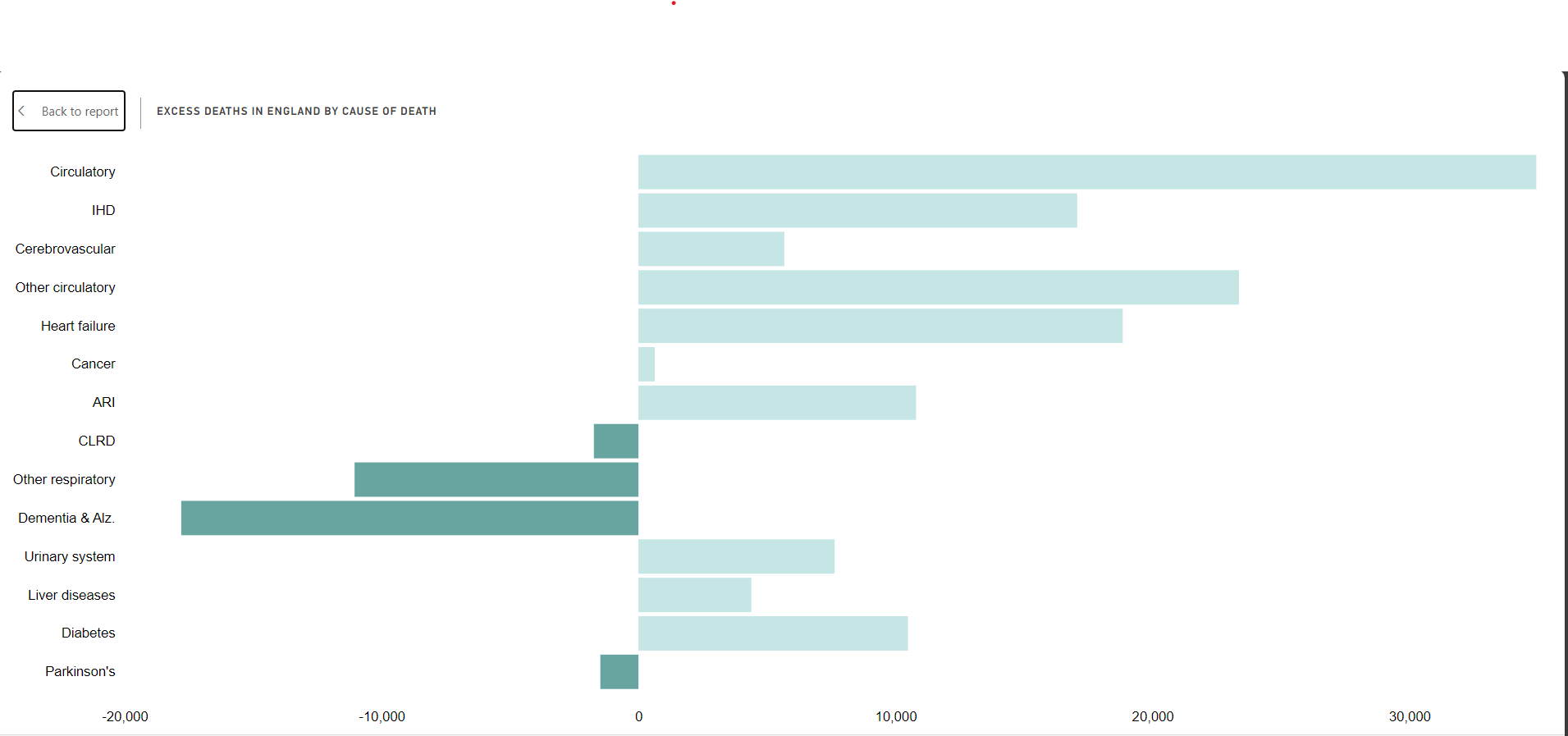
Figure 10. Ratio of actual deaths to expected deaths in England by cause since 2022
ONS for 0-14s also show a very worrying rise in excess deaths in 2022 and 2023 (Fig 11).157
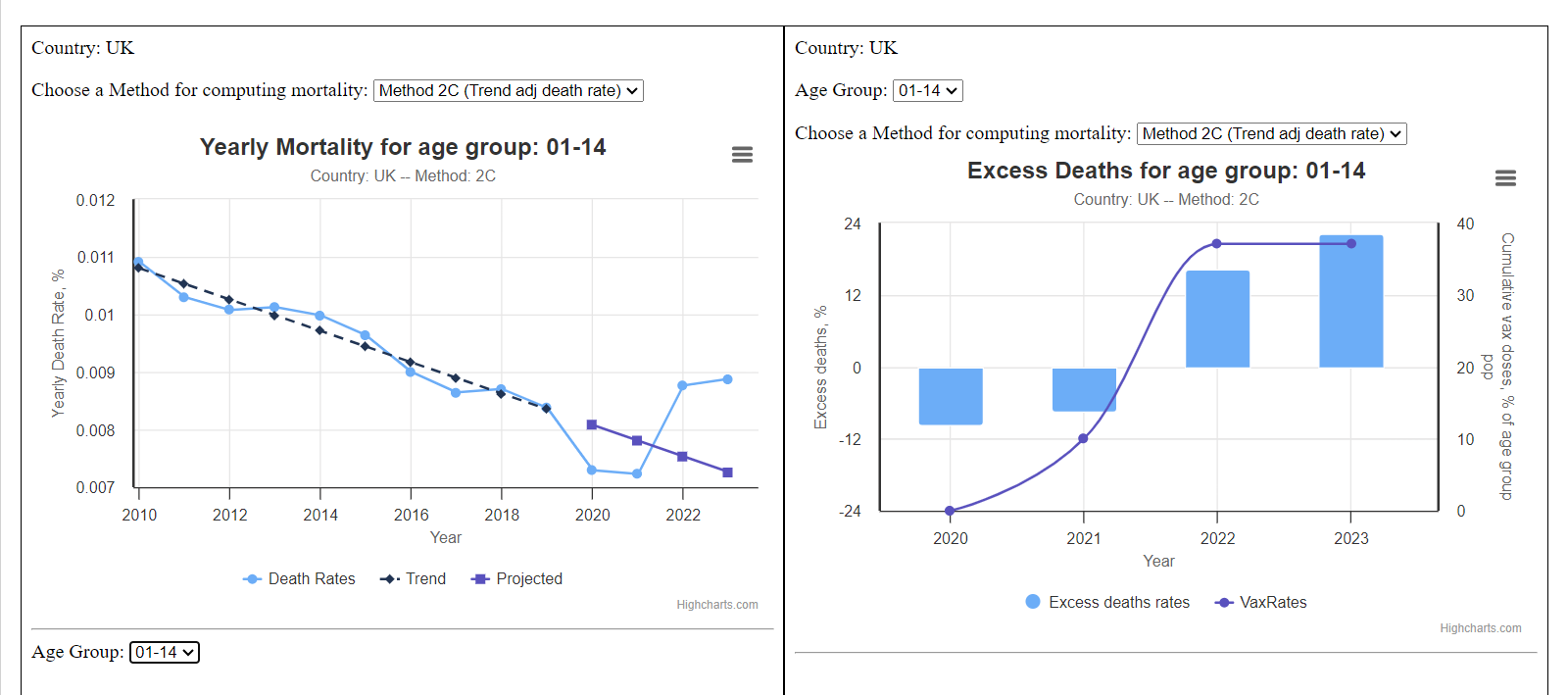
Figure 11. Cumulative Excess mortality for 0-14s and Covid vaccination uptake
127. Immune effects from repeated doses: There is good evidence of an increased risk of infection with increasing numbers of doses as the immunological response changes from IgG1 (an antibody that could provide protection) to IgG4 (a suppressive antibody that enables the body to ignore an antigen so as to prevent inappropriate reactions e.g. allergies).158 The clinical implications of this are unclear but may be relevant to the increasing number of Covid infections in the multiply vaccinated. In vitro studies using blood taken from children, have shown failure to handle other organisms.159 Bloods were taken before and then 1 month and 6 months after a second dose of Pfizer vaccine and showed “sustained decreases in cytokine responses to viral, but not bacterial, stimulants six months after BNT162b2 vaccination.” Again the clinical implications of this are not clear.
128. There have been reports of vaccinated children having a higher than expected rate of other respiratory illnesses. For example, a CDC report160 from seven centres in the US, looked at 7,434 children aged 6 months–4 years attending hospital emergency departments with acute respiratory illnesses. Overall 86% were unvaccinated. SARSCoV-2 infections were low (only 5% of attendees had a positive test), which the authors attribute to “Despite low vaccination coverage and the circulation of several Omicron subvariants, COVID-19– associated ED visits and hospitalization among children with ARI enrolled in NVSN were rare, suggesting most children in this age group experience mild illness from these subvariants or have immune protection from previous SARSCoV-2 exposure”. They make no mention of their findings that fully vaccinated children (10.5% of the total study group) were over-represented in need for hospitalisation (12.7%), supplemental oxygen (13%), or intensive care (13.3%). This may be in part related to the vaccinated group having a more comorbidities but highlights the lack of adequately powered randomised trials of sufficient duration. It was noted in the systematic review of trial data discussed in paragraph 120 above, that there was an increase in LRTIs in the vaccinated pre-school age group.
129. There are increasing concerns in adults about aggressive cancers, both new and relapsing and how these are also related to impaired immune function after multiple doses of vaccine.161 ONS data has revealed 13% excess cancer deaths in 15-44s in 2021 rising to 43% in 2022, with Z-scores shown in Figure 12.162
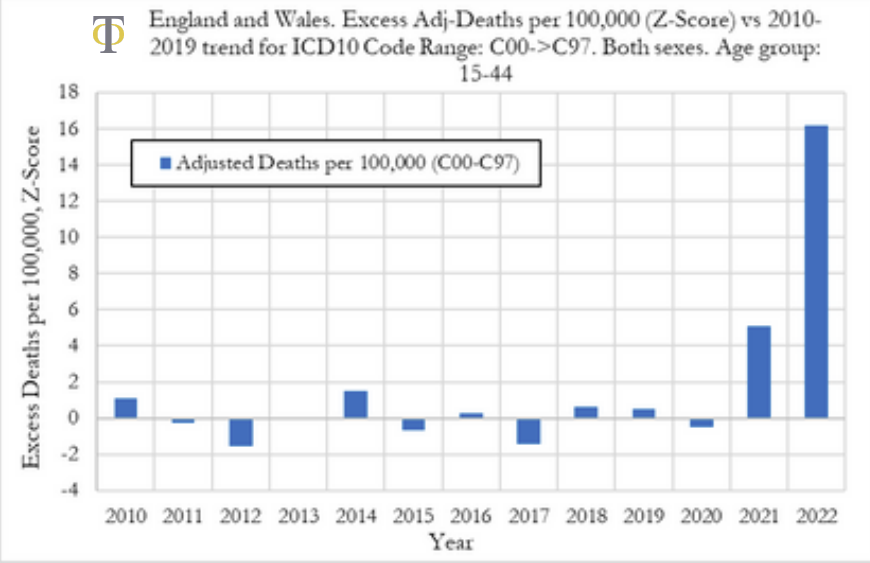
Figure 12. Excess cancer deaths age 15-44 years (ONS data)
For the 15-44-year-old age group in 2022, the 43% overall rise in cancer deaths includes: 22% rise in breast cancer deaths, 80% rise in pancreatic cancer deaths for men and 60% for women, colon cancers 55% for men 45% for women, melanoma 120% for men and 35% for women, brain cancers 35% for men and 12% for women, cancers with no known site 60 % for men and 55% for women. The total numbers are not high because cancer in this age group is rare but that is what makes it so striking. These individuals are typically below the age range for screening programmes and are of an age cohort likely to include young parents, adding to the human cost.
130. Notably, there was a sharp rise in cancer deaths of unspecified site. These were close to zero in 2020, then rose to about +32% in 2021 and +59% in 2022%. These are the rapidly spreading tumours which have already spread to multiple organs at the time of presentation.163
131. The lipid nanoparticles are also known to be cytotoxic.164 Other potential mechanisms are fully discussed here.165
132. There has been a major reluctance to discuss excess deaths, despite now two Parliamentary debates. MP Andrew Bridgen’s speech from November 2023 is reported in Hansard166 and with all the supporting evidence is available on the HART website.167 A further debate took place on 16th January, with several more MPs expressing concern at the lack of answers.168 There is a constant repeat of ‘Correlation doesn’t equal causation’ which is of course correct, but correlation does equal a serious safety red flag.
MARKETING TO CHILDREN
133. From the start of the pandemic there was an overwhelming use of the mainstream media to produce a campaign of fear in an attempt to increase compliance with government rules. “All in, all together” was a UK government partnership with the newspaper industry on Covid-19 ad campaign.169 Of itself, using the press to run government health messages seems reasonable so long as it is clear this is to provide a government message rather than as a censorship tool (see para 166).
134. However, it quickly became apparent that this was being used to present an appearance of consensus, even where no such consensus existed. Here is just one example from Metro Newspaper in October 2021,170 quoting “teen influencer, Amazing Arabella. ‘It’s a great thing for everyone to have, and it’s keeping everyone safe, which is good as well,’ says Arabella, 17. ‘I think people want to get back to normality, just like I do. There are loads of cool events coming up, such as Halloween, Christmas, and we all want to go to them. We don’t want to miss them. We want to spend time with our families, too.’ ‘I have my birthday coming up in December. I hope we’ll be vaccinated in time for that so we can have a bit of a party.’” A consultant paediatrician interviewed said, “The side effects you get from the vaccine are, essentially, a sore arm. Maybe you might feel a bit shiveryshaky. There are some very rare systemic side effects as well, but the common ones are just that” thus totally glossing over the possibility of serious adverse events in this age group. The article also stated, “no part of the medical trials was skipped – instead, all were run in parallel.” This is clearly not correct, as detailed above.
135. It was NOT made clear that these were paid government promotions until after several complaints and FOIs. Here is an article on Mumsnet from a web archive 171[RJ/169 INQ000000] and now the currently available article with its warning of financial incentive.172
136. Messaging was clearly aimed at children and their parents, for example the alarming line: ‘Don’t Kill Your Granny’ and strong ‘prosocial’ messaging such as ‘No-one is safe until everyone is safe’ being used to increase vaccine uptake. Many of the advertisements for the children’s vaccines implied that by taking the vaccine, children could protect older or more vulnerable members of their community, despite it being clear that the vaccines could not prevent infection and transmission. Children were then used in advertisements to increase the peer pressure to conform.
137. Pictures were also used to link to popular cartoon characters such as Peppa Pig and Superheroes.
The teaching materials from the Stephen Hawking Foundation in use in London Schools and discussed in para 77 above, illustrate the pressure exerted on children with questions such as, “Should we act as a community for the good of all?” It would be a brave child to be the only one in their class to decline vaccination.
138. Vaccination pop-up sessions were advertised at Thorpe Park Theme Park. Petting animals were available for some clinics, plus free ice creams and doughnuts. Invitations from the school vaccination services have been sent addressed directly to children, enclosing ‘party’ style letters and even one with enclosed sunflower seeds.
139. In my entire career as a paediatrician, I have never seen a campaign run in this manner. It seriously calls into question the principles of informed consent, which specifically say that inducements must not be used.173
140. An item presented on CBBC’s Newsround programme in June 2021 i.e. before the vaccine had even been recommended for children, was highly misleading, claiming that the children’s vaccines were 100% safe.174 Complaints to the BBC led to a change to the wording but not before the programme had been shown in many schools around the country.
141. The MHRA’s guidance to the UK Regulations governing the advertising of medicines, the Blue Guide,175 very specifically states that the use of the word ‘Safe’, when marketing any medicinal product, is unacceptable. Section 6.6. states, “Advertising which states or implies that a product is “safe” is unacceptable. All medicines have the potential for sideeffects and no medicine is completely risk free as individual patients respond differently to treatment”. These rules apply to everyone in the UK, including the media and the government. Yet the Government, the regulators, and the media, in promoting the use of the Covid vaccines, regularly used the phrase “Safe and Effective” and continued to do so long after it became clear that these vaccines were far from safe. The Blue Guide makes brief mention of children in Section 5.4: “Advertising of medicines should not be directed exclusively or principally at children (under-16s)” but some of the examples shown above come very close to direct advertising.
142. Dr Albert Bourla, Chair and CEO of Pfizer said in November 2021 regarding vaccinating 5–11-year-olds:176 “So there is no doubt in my mind that the benefits, completely, are in favour of doing it.” Bourla stated this publicly in an interview broadcast by the BBC in early December 2021, prior to vaccine approvals being granted for that age group. At the time, the children’s campaigning group UsForThem raised a complaint with the Prescription Medicines Code of Practice Authority about Dr Bourla’s comments and ultimately, a full year later following a lengthy appeal process, the PMCPA’s Appeal Board found that the comments were misleading and incapable of substantiation.177 UsForThem was “asked by the [PMCPA] not to discuss the case until the appeal process was final. That took over a year, during which time the C19 jab roll-out to the [5-11] age cohort proceeded.”
143. NHS GPs were paid differing fees depending on whom they vaccinated, with almost double payments in August 2021 for injecting a child aged 12-15 years.178 Questions must be asked as to why an extra incentive was believed necessary for this age group. It is notable that the MHRA Blue Guide says: “The Bribery Act 2010 provides a legal framework to combat bribery in the public or private sectors. It includes offences covering the offering, promising or giving of an advantage, and requesting, agreeing to receive or accepting of an advantage. It is enforced by the Serious Fraud Office (SFO). The SFO has advised that this does not prevent proportionate promotional expenditure.” It is hard to see how this is a proportionate expense when compensation was twice as high for teenagers as adults. A higher fee for a domiciliary visit to a housebound high-risk patient is very different.
144. Guidelines179 were provided to vaccine clinic staff on different approaches to try and persuade people to be vaccinated, using personal risk for older adults but using fear of making other people sick when talking to younger people. Peer pressure is included as a positive tool. “Since young people tend to be more susceptible to peer influence, it is likely that social norms can be particularly effective when targeting this group.” “Use messengers that young people relate to deliver vaccine messages. These, for example, can be social media influencers that are in their age group.” This is contrary to GMC guidelines on obtaining informed consent.
145. Even now in 2024, the NHS guidance is that children aged 12-17 may be vaccinated if they have an immunocompromised household member.180 This is despite it being clear that these vaccines do not prevent infection or transmission; indeed there is clear evidence among regularly tested healthcare workers that more doses of vaccine are associated with higher rates of infection, as shown in Figure 2 (see paragraph 97 above).
146. A further letter with a Freedom of Information request was sent to the JCVI in September 2023181 (see Appendix A), asking for details as to how they have reached the decision to continue offering vaccines for healthy adolescents who are household contacts of someone immunocompromised, despite dropping the vaccines for all healthy under-65s. In reply they said they did not hold information on NNV (number needed to vaccinate) to prevent one serious case of Covid-19 in an immunocompromised contact, nor had they any information regarding legal advice. They referred us to the link where the minutes will be published “in due course” but no minutes on this topic have been identified.
VACCINES IN PREGNANT AND LACTATING WOMEN
147. Covid vaccines have been heavily promoted in pregnancy despite the fact that pregnant women were specifically excluded from all the trials.
148. Appropriate animal studies were not performed; not even pharmacokinetic studies to check if the mRNA vaccines crossed the placenta or entered breast milk. It was emphasised that IgG antibodies made by the mother would cross, thus protecting the baby. A death was reported to VAERS182 of a 5-month-old fully breastfed infant who developed a dangerously low platelet count 24-hours after his mother received her second dose of Pfizer Covid vaccine. The baby was admitted to hospital and died two days later with a major brain haemorrhage. A diagnosis of Thrombotic Thrombocytopenic Purpura was made. The VAERS report noted “No new exposures aside from the mother’s vaccination the previous day.”
149. In England and Wales, ONS data reveals stillbirth rates in 2021 have risen above the 5 year average. They have been above expected since July 2021, having been below expected in May to December 2020, as shown in Figure 13.183 Data for 2022 have yet to be published.
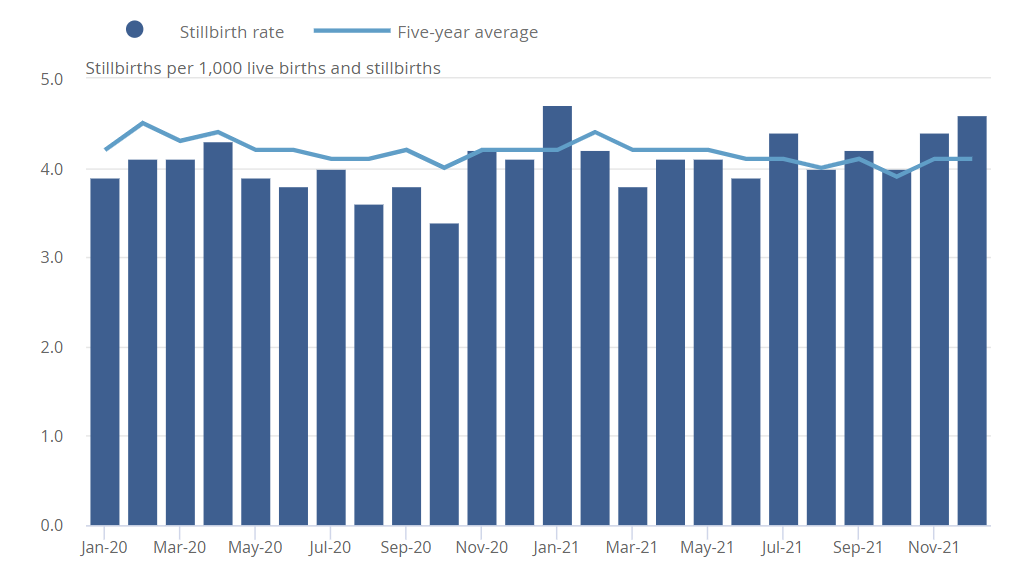
Figure 13. Stillbirth rates by month of occurrence, England & Wales, 2020 to 2021 (ONS data)
An FOI to all obstetric units in the UK has revealed that most units have not added Covid vaccination status to their electronic records and are therefore unable to check for any links with numbers of stillbirths or neonatal deaths.
150. Excess Neonatal deaths in Scotland: a public inquiry has been set up after two peaks in neonatal deaths in September 2021 and March 2022. Public Health Scotland have specifically stated it would not look at vaccination status despite a clear temporal link shown in Figure 14. The changes are even clearer if compared to data going back to 2010 (Figure 15.) showing a steady gradual decline in mortality rates up to and including 2020, before the obvious rise from mid-2021.
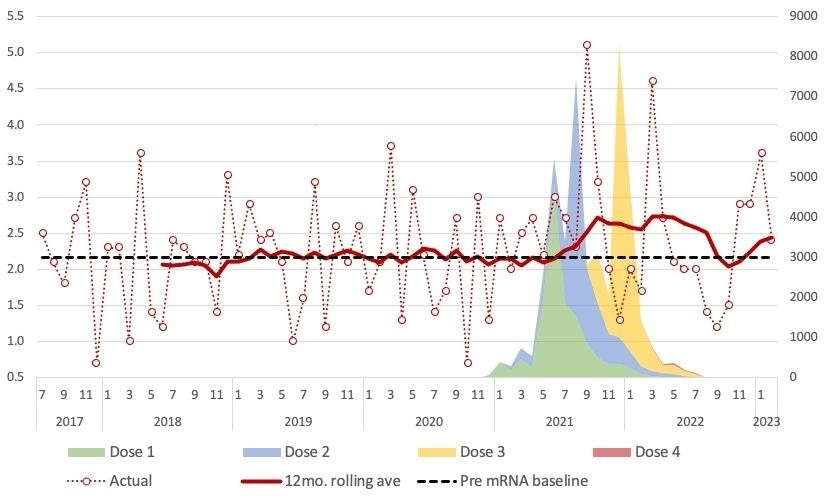
Figure 14. Weekly Neonatal Deaths per 1000 live births – Scotland 2017-2023
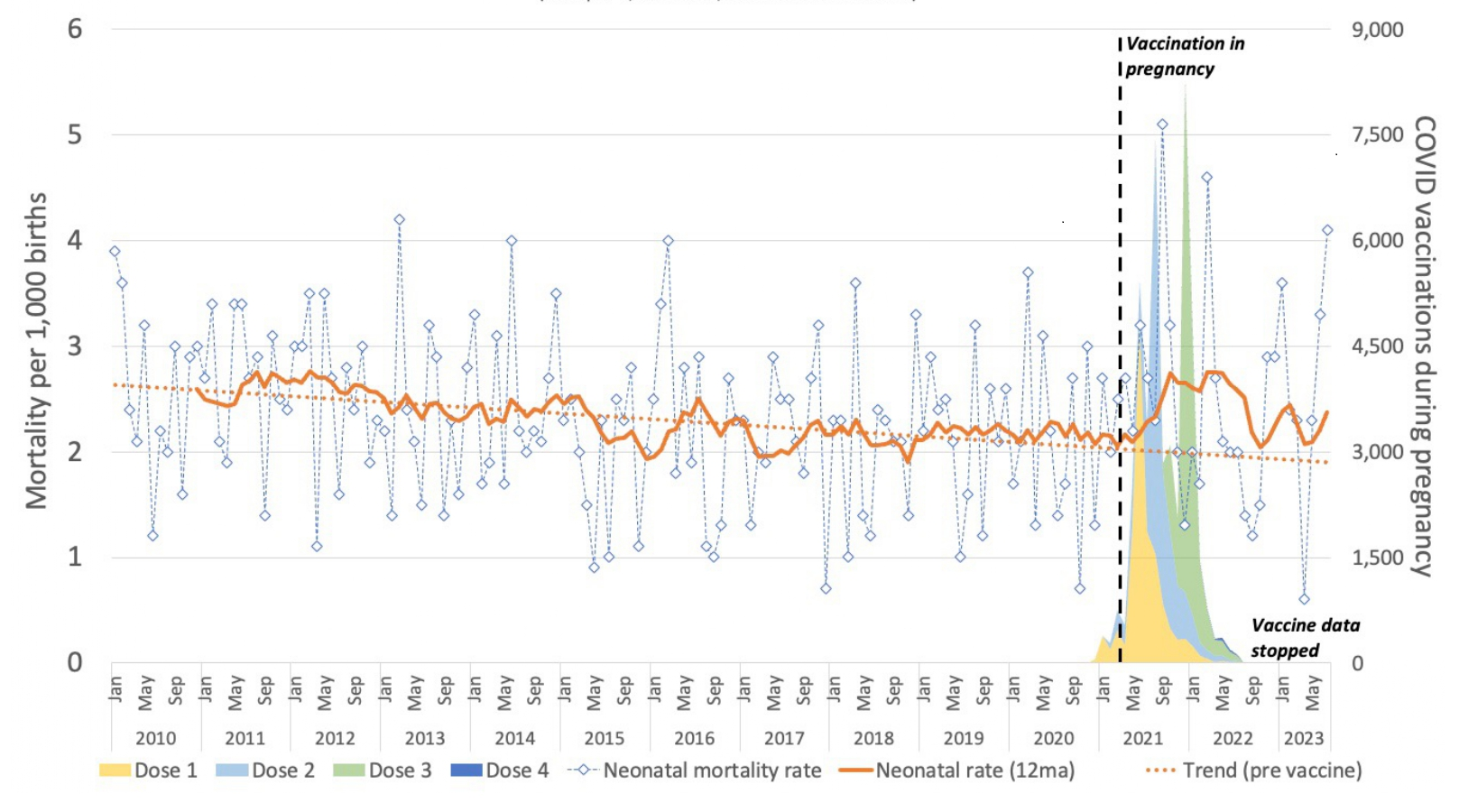
Figure 15. Weekly Neonatal Deaths per 1000 live births – Scotland 2010-2023, (PHS data)
151. Remarkably, the reason given for not looking was because it could increase vaccine hesitancy184 and that there was no known mechanism for harm, nor any public health action which might arise. Correspondence185 with the Inquiry Chair is included in Appendix A. The Inquiry has now reported and covid vaccination status was not investigated.186 Similar rises have been shown in Israel again with a peak in neonatal deaths coinciding with the initial vaccination of pregnant women and a second peak coinciding with the boosters.187
152. Data from Public Health Scotland have also revealed a rise in post-neonatal infant deaths (i.e. from 1 month of age to 12 months), shown in Figure 16.
Figure 16. Weekly Post-neonatal Deaths per 1000 live births – Scotland 2010-2023
Monthly data from 2016-2023 showing infant deaths (all deaths under 1 year of age) as a percentage of live births have shown a stepwise change from May 2021, which is still ongoing. Infant mortality from January 2016 to April 2021 was running at 0.323% ie 3.23 per 1000 births. In the 32 months since vaccination of pregnant women in Scotland began, infant mortality has averaged 0.374% or 3.74 per 1000. This would equate to 63 excess infant deaths.
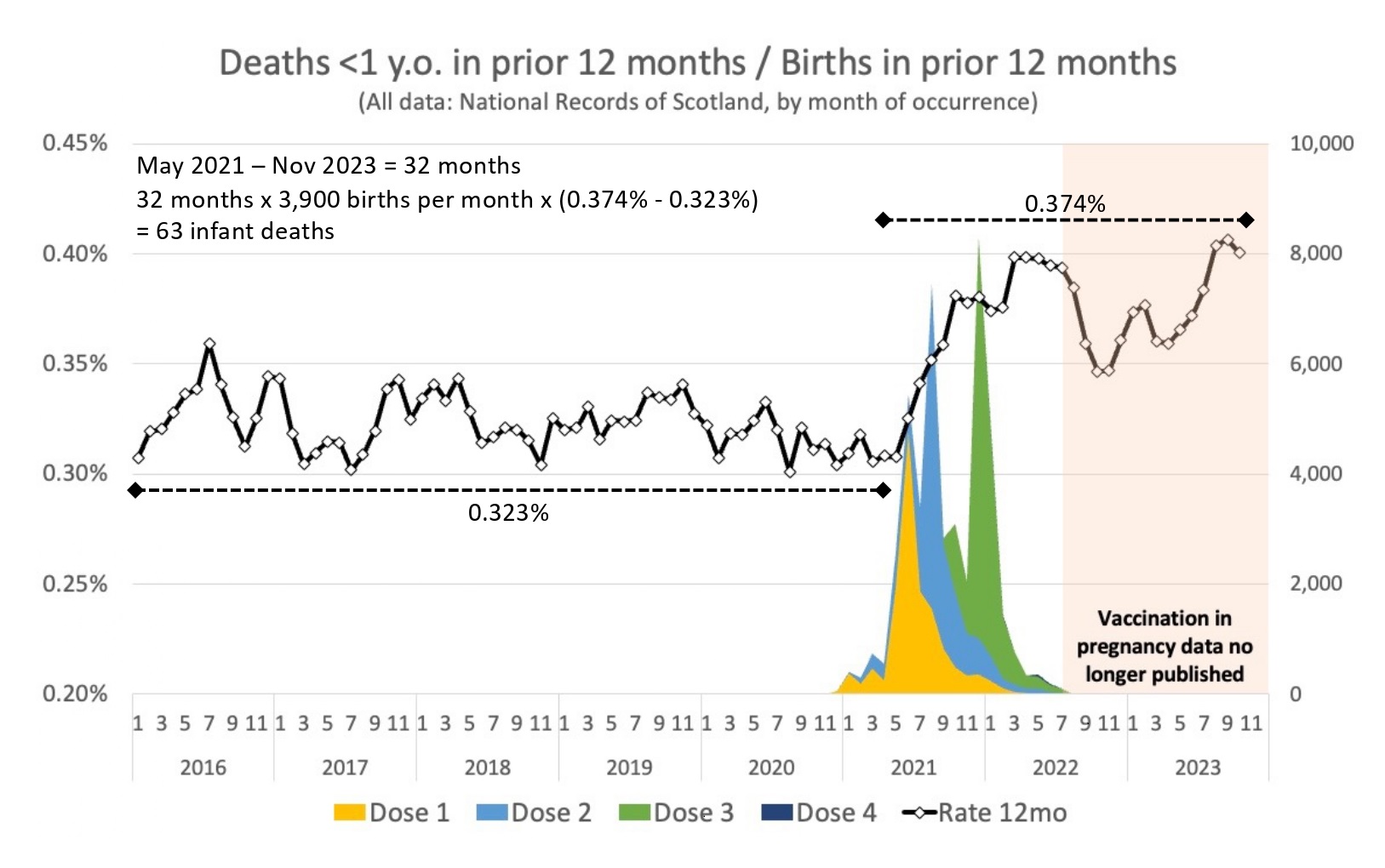
Figure 17. Monthly Infant Deaths per 100 live births – Scotland 2016-2023
153. Early in the vaccine rollout, a high rate of menstrual disorders was reported, including in young adolescents.188 This was especially concerning, given the known concentration of lipid nanoparticles (LNPs) in the ovaries of rats studied by Pfizer. A large study189 using the VAERS database, looked at the ratio of various relevant adverse event reports after Covid-19 vaccines in comparison to reports following influenza vaccines over 25 years. A significant ratio of more than 2:1 was found for the following conditions “menstrual abnormality, miscarriage, fetal chromosomal abnormalities, fetal malformation, fetal cystic hygroma, fetal cardiac disorders, fetal cardiac arrest, fetal arrhythmias, fetal vascular malperfusion, fetal growth abnormalities, fetal abnormal surveillance, placental thrombosis, fetal death/stillbirth, low amniotic fluid, preeclampsia, premature delivery, preterm premature rupture of membrane, and premature baby death”. For some conditions, the reporting ratio was hugely raised above the 2:1 safety signal: menstrual abnormality reports x 298, miscarriages x 15, congenital malformations x 15, still births x 9.5. This study has been strongly criticised particularly for potential reporting bias, but even if these findings overstate the true picture, they should nevertheless constitute a major red flag warranting a pause in vaccine rollout to pregnant women pending a full investigation.
154. In the interests of transparency, a legal challenge in the US eventually resulted in Pfizer releasing all their data. One item coming to light was a report to the FDA dated April 2021 looking at adverse event reports for pregnant or lactating women.190 A number of case reports are listed including 51 women suffering a spontaneous abortion and 6 going into preterm labour. A further 41 adverse events were in reported in breast-feeding infants shortly after their mothers’ Covid vaccination. Again, no denominator is given but this was at a time when most of the adverse events in this report were of vaccination being wrongly given in pregnancy. It highlights the importance of properly randomised trials.
155. It was also shown in sperm donors that motile sperm counts dropped significantly three months after Covid vaccination and remained low after 5 months when the study was discontinued.191
156. In addition to the concerns about increase in miscarriages, stillbirth rates and neonatal deaths, there has been a significant fall in live birth rates in several countries with high vaccination rates.192 No causal link has been established at the present time but if in the next decade it becomes apparent that the mRNA vaccines have affected fertility, then it will be a bit late to apologise to the numerous adolescents who took a medication in good faith for which totally inadequate reproductive testing had been undertaken.
ETHICAL & LEGAL ISSUES:
157. Guilt messaging regarding ‘Protecting Granny’ was discussed in paragraph 136 above. Even if these vaccines could prevent infection and transmission, there would still be an enormous ethical question over using children to protect adults, particularly with a new and experimental medicine with no information on long-term side-effects. More recently, all Covid vaccines have been dropped for healthy under-65s, yet they remained available for 12-17s if a household member is immunocompromised, as discussed above (paragraphs 145 & 146).
158. Using children in this way, even if it were ethical, had no hope of being effective, given the brevity of protection against infection and transmission, which was already apparent when childhood vaccination was promoted, and the later-appreciated increased risk of infection in the vaccinated.193
159. In summer 2023, children were recruited to a trial of a new Moderna booster vaccine- the NextCOVE study194 with a very concerning recruitment leaflet195 provided by Rotherham Doncaster and South Humber NHS Foundation Trust, which opens with this emotionally loaded paragraph:
“The COVID-19 pandemic is like nothing we’ve seen in more than a century and it has altered each and every one of our lives. Now, you or your child could be a part of important research on an investigational COVID-19 vaccine. By enrolling in the NextCOVE Study, you or your child will be contributing to a potential solution to the evolving COVID-19 pandemic, which has affected the entire world.” Further on it states:
“By taking part in this trial, you or your child could make a difference for your family, your community and people everywhere.”
160. This again raises concerns with contravening the Declaration of Helsinki196 and other UK and international laws given the impossibility of a benefit and the known harms. The Universal Declaration on Bioethics and Human Rights Article 4 and Article 7 make it clear that all medical interventions must be in the best interest of the individual concerned, particularly in the case of children who are not able to give consent. “All medical research involving human subjects must be preceded by careful assessment of predictable risks and burdens to the individuals and groups involved in the research in comparison with foreseeable benefits to them and to other individuals or groups affected by the condition under investigation.”
161. A letter was sent urgently to the CEOs and Chairmen of the 37 UK participating centres.197 Replies were mixed, with most centres having decided against recruiting children. Five centres had recruited between them a dozen adolescents. All these centres hid behind any responsibility being that of the sponsor, Moderna and the overarching approval of the MHRA and the Health Research Authority (HRA). FOIs to the latter have been refused on the basis of commercial sensitivity and are ongoing.
162. One participating centre was advertising on WhatsApp a payment of £1500 on trial completion.198 An FOI was submitted to ask if this was authorised and the response is most ambiguous.199 This is in clear breach of international guidance on payments and remuneration.200 After several emails to the Head of Information and Governance and an Internal Review,201 it transpired that the £1500 offered came from version 1 of the trial application, which had been rejected by the Research Ethics Committee(REC). According to the REC committee minutes202 obtained under an FOI, the Approvals Manager stated, “this amount seemed much higher that what would be considered a reasonable reimbursement and therefore would contravene clinical trial regulations. The Medicines for Human Use (Clinical Trials) Regulations (2004) explicitly prohibit the giving of incentives or financial inducements to children… or their parents.” A formal complaint has been submitted to the PMCPA, who have confirmed that they will investigate Moderna’s behaviour.
163. Honesty and transparency in public office is fundamental to maintaining trust. It is notable that in England by November 2022,203 one year after vaccines were first offered for 12-15s and 6 months after the 5-11s rollout, the uptake was low at 38% of 12-15s receiving the recommended 2 doses and only 6.7% of 5-11s completing their primary course. A survey commissioned earlier this year204 showed that most parents were unaware that the JCVI had initially recommended against Covid vaccines for healthy children.
164. The GMC’s Good Medical Practice guidelines205 which were in place throughout the pandemic, states as the top-most requirement for a good doctor that they must:
- Make the care of your patient your first concern.
In updated guidelines implemented from 30th January 2024,206 this fundamental tenet of the doctor-patient relationship has been inexplicably moved. The majority of the guidance is unchanged and still clearly requires doctors to:
- Respect every patient’s dignity and treat them as an individual.
- Act promptly if you think that patient safety ..may be seriously compromised.
- Protect and promote the health of patients and the public.
Yet the GMC and Royal Colleges have shown scant support for those doctors who have been trying to follow these requirements to protect the public from harm.
CENSORSHIP:
165. Censorship has been widespread, with governments colluding with social media platforms to remove any statements that questioned the official messaging on lockdowns, masks and, especially, vaccines.
166. This censorship affected the mainstream media, which possibly have also been influenced by the large amounts of government advertising revenue. Sarah Knapton of The Daily Telegraph, recently revealed that when she had reported on the thrombotic complications of AstraZeneca vaccine in young adults in Scandinavia in March 2021, the newspaper received a phone call from a senior staff member at the MHRA saying that if they did not modify their reporting, they would be excluded from MHRA press briefings.207 The Telegraph also published our first letter to the MHRA208 and a brief follow-up article but were unwilling to publish anything further.
167. We have since discovered through the efforts of Big Brother Watch,209 that our June 2021 letter to the Chief Medical Officer had been passed by the Department of Health and Social Care to the Counter Disinformation Unit (CDU).210
168. Another member of our group was reported to the CDU for saying, on Talk Radio, that vaccination of children against Covid-19 was unwarranted. This denigration of differing views was pervasive and like use of the word ‘Safe’, is in contravention of the Prescription Medicines Code of Practice Authority marketing guidelines,67 sub-clause 6.7 clearly stating, “The health professions and the clinical and scientific opinions of health professionals must not be disparaged.” This code of practice is aimed at the pharmaceutical industry, but meanwhile the Government and the Media, in promoting these products, strongly disparaged the views of doctors and scientists who argued, as we did, that the risk/benefit calculus did not favour the vaccination of younger demographics, particularly children.
169. Censorship within academia has also been problematic. One of our members, a professor with a large volume of peer reviewed publications, has recently been dropped from speaking at a conference on a topic totally unrelated to Covid-19 vaccines, on the basis that his “presence would be a distraction” but a subsequent response to a Subject Access Review yielded a different reason, namely: “It was felt comments made by [name] on Twitter, conflicted with NHS values regarding vaccination, and thus would not be in keeping with our values as an NHS organisation.” 211 Perhaps even more seriously, a whistle-blower from an academic department funded by a large UK charity, reported being asked to sign a non-disclosure agreement regarding some cardiac research, the results of which were suggesting a problem for the mRNA vaccines. There has been no response from the head of department. An open letter to the Charity Commission212 asking them to investigate urgently, but they replied that they “will not be contacting the charity regarding the issues raised”.
170. A recent report from Big Brother Watch has shown evidence of military involvement on the assessment of mis- or dis-information for the Cabinet Office.213
171. Other doctors and academics who are signatories to our letters have been reported to their heads of department for appearances on Talk Radio or merely for sharing information on Twitter. Others have been subject to disciplinary hearings. Several doctors have also been reported to the GMC, which has a chilling effect on other medics speaking out, despite their grave concerns. Two trainee doctors have only signed our letters anonymously using initials and qualifications only, because of fear of repercussions (personal communication).
SUMMARY:
172. In summary, we are a group of experienced health professionals and academics who have grave concerns about giving children mRNA vaccines from which they could not benefit and for which there were absolutely no data on long term safety.
173. The MHRA and JCVI failed to answer any of our questions with anything other than platitudes such as “Safe & Effective”.
174. The time has now come to stand back and acknowledge that there is no emergency for children and that for them the balance of benefit and risk clearly favours the development of natural immunity.
175. No child should be offered a vaccine with the express purpose of benefiting another person.
IMPORTANT QUESTIONS: For the MHRA & JCVI
176. Questions asked in May & June 2021 prior to authorisation
a. What calculations of the risk of myocarditis have you included when looking at benefit:risk balance?
b. Why have you not published the data delineated by age band so that young adults can make properly informed choices?
c. How have deaths in 12–17-year-olds from VAERs and other reporting systems been factored into your deliberations?
d. Have you seen any data which can predict the quantity and duration of spike protein produced by individuals following a specified dose of mRNA?
e. What potential long term side effects have been considered?
f. What is the number needed to treat for one individual to benefit have you used in your calculations?
g. Given that children are not seriously impacted by COVID-19, and there has never been an emergency situation regarding children’s health relating to SARS-Cov-2 infection, how have you defined ‘Emergency’ for the purposes of this authorisation?
177. Questions asked in February 2022 re 5-11s
a. Where are the minutes of the meetings at which these decisions were made?
b. What are your calculations of the number of healthy 12-17-year-olds (and of all household members aged 12-64) needed to vaccinate to prevent the hospitalisation of one vulnerable family member;
c. Did you take any legal advice on how these unnecessary booster doses to children comply with UK and international law?
178. Questions asked in Autumn 2023 regarding the ongoing vaccinations
a. Will JCVI agree that the time has come to pause and acknowledge that there is no emergency for children and that for them the balance of benefit and risk now clearly favours natural immunity.
b. Will they provide their number of 12-17-year-olds needed to Vaccinate (NNV) to prevent Covid-19 hospitalisation of an immunocompromised household member with evidence (not modelling) to defend the assumptions in that calculation?
Statement of Truth
I believe that the facts stated in this witness statement are true. I understand that proceedings may be brought against anyone who makes, or causes to be made, a false statement in a document verified by a statement of truth without an honest belief of its truth.
Rosamond A K Jones
Dr Rosamond A K Jones, MBBS (Hons), DRCOG, MD, FRCPCH
retired Consultant Paediatrician. GMC No 1485616
APPENDIX A
- Letter to Chief Medical Officer regarding masking of children in school, 8 August 2020.25
- Letter to Professor Andrew Pollard re the children’s AstraZenenca trial, 16 February 2021, and his reply.74
- Letter to MHRA re Covid vaccines for 12-15s, 17 May 2021.96
- Full supporting paper for MHRA, 17 May 2021.214
- Response from MHRA, 4 June 2021.215
- Further letter to MHRA, 6 June 2021.216
- Letter to JCVI & CMO regarding their duty of care to assess safety, 6th June 2021.101
- Further letter to JCVI, 19th August 2021.217
- Follow-up letter to MHRA, 23August 2021.218
- Letter to the four Chief Medical Officers of the UK, 6th September 2021.219
- Letter to MHRA, JCVI & UKHSA re myocarditis in adolescents, 14 November 2021.220
- Letter to JCVI about 2nd dose for adolescents, 9 December 2021 and their reply 9 March 2022.141
- Letter to GMC about matters of informed consent. 10 December 2021. [RJ_68 INQ000000]
- Reply from GMC, 7 January 2022.221
- Letter to MHRA re excess deaths data for adolescent males, 19 January 2022.222
- Letter to JCVI calling for halt to Covid vaccines for children pending urgent safety review, 10th February 2022.121
- Letter to FDA vaccines committee re Covid vaccines in 0-4s, 29 March 2022.223
- Further letter to FDA on vaccines for 0-4s, 6 June 2022.224
- Letter to new Secretary of State for Health, 12 July 2022.225
- Reply from DHSC 9 August 2022 and further letter 11 August, 2022.226,227
- Letter Dr Jenny Harries, UKHSA re new myocarditis guidelines, 14 August 2022.228
- Letter to Medical Defence Union on informed consent 22 August 2022.69
- Letter to Professor Matthew Snape, Chief Investigator & Chair of Berkshire Research Ethics Committee re ‘com-cov-3’, a new trial of boosters in adolescents, 12 August 2022.229
- Letter to Prime Minister Liz Truss, 26 September 2022.230
- Letter to President, Royal College of Obstetricians and Gynaecologists re vaccines in pregnancy, 13 November 2022.231
- Letter to latest Prime Minister, Rishi Sunak, 22 November 2022.232
- Reply from President of RCOG, 29 November 2022.233
- Further letter to RCOG, 2 December 2022.234
- Letter to MHRA regarding vaccines for 0-4s, 4 December 2022.235
- Letter to JCVI regarding vaccines of 0-4s, 6 December 2022.236
- Letter calling for an independent review of vaccines safety, 31 January 2023.237
- Letter to Chair of Independent Inquiry into Scottish Neonatal Deaths and subsequent correspondence, 22 February 2023.184
- Further letter re vaccination in pregnancy, 23 February 2023.238
- Letter to MHRA & HRA re new Moderna booster trial in adolescents. 16 July 2023.239
- Letter to JCVI re vaccination of adolescents to protect vulnerable household members, 4 September 2023.240
APPENDIX B
1. CCVAC LEADERSHIP TEAM – www.ccvac.org.uk
1.1. Dr Rosamond Jones, MBBS, DRCOG, MD, FRCPCH
Dr Rosamond Jones was a Consultant Paediatrician with over 40 years’ experience in the NHS and with a special interest in neonatal intensive care and paediatric HIV. She has served on the Advisory Committee of the National Perinatal Epidemiology Unit and on the Education & Training committee of the RCPCH. An active member for many years in the British Perinatal Trials Group, she was also involved in reviewing NICE guidelines alongside some editorial work. Since retiring from the NHS, she has undertaken several tours teaching on SAFE Obstetrics courses in countries in Africa.
At the outset of the pandemic she renewed her GMC registration, aiming to return to work, but children were so little affected that retired paediatricians were not needed. She turned her time to campaigning for children particularly for reopening of schools. She is a spokesperson for the Health Advisory & Recovery Team (HART) and leads a group of health professionals and scientists in writing letters to the regulatory authorities about the balance of benefit and risks for covid-19 vaccines in childhood.
1.2. Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMed Sci
Professor Angus Dalgleish is Professor Emeritus of Oncology, University of London and Principal, Institute for Cancer Vaccines & Immunotherapy. He was previously Professor of Oncology at St Georges Hospital.
He qualified in medicine from University College and Hospital with an intercalated Hons BSc in Anatomy with Prof JZ Young, FRS. He graduated at UCL/UCH in 1974 and was a flying doctor in Mount Isa in Australia before training in Medicine in Brisbane and Oncology in Sydney. He did an MD on retrovirus with Professor R Weiss, FRS, at the ICR, where he published a seminal paper on HIV, its receptors and pathogenesis.
He was appointed Foundation Chair in Oncology at St. George’s University of London in 1991. His work has focussed on tumour immunology; he developed the Thalidomide programme with Celgene, resulting in Lenalidomide, for which he received the Joshua Lederberg Prize. After trialling over a dozen different cancer vaccines he focussed on IMM-101 combinations as the most effective for future development.
In the last year, he has become increasingly concerned at aggressive relapses in several of his melanoma patients following their third or fourth dose of Covid vaccine.
1.3. Professor David Livermore, BSc, PhD
David Livermore began his career in 1980 as Research Assistant at the London Hospital Medical College, writing a PhD ‘On the side’. By 1994 he’d risen to Senior Lecturer in Medical Microbiology. In 1997 he moved to the Public Health Laboratory Service, now Public Health England, swiftly becoming Director of its Antimicrobial Resistance Monitoring and Reference Laboratory. He remained until 2011, when he transferred to the University of East Anglia as Professor of Medical Microbiology. He has recently retired and continues as a Professorial Fellow.
Across 40 years he has belonged and led teams that have defined the evolving epidemiology and molecular nature of antimicrobial resistance. He has authored over 500 papers and has served on UK government advisory committees on antimicrobial resistance and healthcare-infection.
1.4. Dr David Critchley, BSc, PhD
Dr Critchley’s PhD in pharmacology was sponsored by Pfizer. He has more than 30 years experience in drug discovery and development in roles covering preclinical pharmacology, drug metabolism & pharmacokinetics and clinical pharmacology. He has worked on antiviral projects for HIV for Roche and has anti-infective experience in antiparasitic, antifungal and antibiotic drug discovery. As Eisai’s Global Head of Clinical Pharmacology he supported many new drug approvals including diethylcarbamazine (WHO), rufinamide, perampanel, zonisamide, lenvatinib and eribulin, as well as approvals for cannabidiol for the treatment of childhood epilepsy syndromes at GW.
1.5. Dr John Flack, BPharm, PhD.
Dr Flack has 40 years’ experience in senior R&D and executive positions in pharmaceuticals and biotechnology. He attained a PhD in the Dept. of Pharmacology, School of Pharmacy, London University and a post-doctoral fellowship at the Worcester Foundation for Experimental Biology in Massachusetts, U.S.A.
He was Director of Safety Evaluation at Beecham Pharmaceuticals and Senior Vicepresident for Drug Discovery at SmithKline Beecham, during which time Nabumetone (an anti-inflammatory), Paroxetine (an anti-depressant), Granisetron (an anti-emetic), Eminase (a thrombolytic), Augmentin (an oral anti-bacterial), Timentin (an injectable anti-bacterial), penciclovir/famciclovir (injectable/oral antivirals), Bactroban (a topical anti-bacterial) were discovered, developed and registered for marketing.
More recently, he volunteered at his local vaccination centre helping the NHS roll out COVID-19 vaccines in the community, but resigned when the rollout started extending to younger and younger age groups for whom he felt there was insufficient safety data.
2. Members of CCVAC
▪ Dr Rosamond Jones, MBBS, DRCOG, MD, FRCPCH, retired consultant paediatrician, convenor CCVAC (Children’s Covid Vaccines Advisory Council)
▪ Professor Anthony J Brookes, Professor of Genomics and Health Data Science, University of Leicester
▪ Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMed Sci, Professor Emeritus of Oncology, University of London
▪ Professor Richard Ennos, MA, PhD. Honorary Professorial Fellow, University of Edinburgh
▪ Professor John Fairclough FRCS FFSEM retired Honorary Consultant Surgeon
▪ Professor Norman Fenton, CEng, CMath, PhD, FBCS, MIET, Emeritus Professor of Risk Information Management, Queen Mary University of London
▪ Professor David Livermore, BSc, PhD, Emeritus Professor of Medical Microbiology, University of East Anglia
▪ Professor Martin Neil, BSc PhD, Professor of Computer Science and Statistics
▪ Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Honorary Professor of Professional Practice, Buckingham University
▪ Professor Roger Watson, FRCP Edin, FRCN, FAAN, Honorary Professor of Nursing, University of Hull
▪ Professor Keith Willison, PhD, Professor of Chemical Biology, Imperial, London
▪ Lord Moonie, MBChB, MRCPsych, MFCM, MSc, House of Lords, former parliamentary under-secretary of state 2001-2003, former consultant in Public Health Medicine
▪ Dr Najmiah K Ahmad, BM MRCA FCARCSI, Consultant Anaesthetist
▪ Dr Ali Ajaz, Consultant Psychiatrist
▪ Dr Shiraz Akram, BDS, Dental surgeon
▪ Dr Victoria Anderson, MBChB, MRCGP, MRCPCH, DRCOG, General Practitioner
▪ Julie Annakin, RN, Immunisation Specialist Nurse
▪ Wendy Armstrong, Practice Nurse
▪ Helen Auburn, Dip ION, MBANT, CNHC, Registered Nutritional Therapist
▪ Dr Michael Bazlinton, MBCHB MRCGP DCH
▪ Dr David Bell, MBBS, PhD, FRCP(UK), Public Health Physician
▪ Dr Michael D Bell, MBChB, MRCGP, retired General Practitioner
▪ Dr Alan Black, MBBS, MSc, DipPharmMed, retired pharmaceutical physician
▪ Dr David Bramble, MBChB, MRCPsych, MD, Consultant Psychiatrist
▪ Dr Ancha Bala Joof, MBChB, MRCGP, General Practitioner
▪ Dr Elyse Baril-Guerard, MD, CCFP, MRCGP, General Practitioner
▪ Dr Ian Barros D’Sa, BM, MRCS, FRCR, PGCMEd, Consultant Radiologist
▪ Dr Mark A Bell, MBChB, MRCP(UK), FRCEM, Consultant in Emergency Medicine, UK
▪ Dr Ashvy Bhardwaj, MBBS, DRCOG, MRCGP (2018)
▪ Dr Gillian Breese, BSc, MB ChB, DFFP, DTM&H, General Practitioner
▪ Dr Ian Bridges, MBBS, retired General Practitioner
▪ Dr Emma Brierly, MBBS, MRCGP, General Practitioner
▪ Dr Rachel Brown, MBChB, LLM, CFMP, MRCPsych
▪ Kim Bull, Foundation Degree in Paramedic Science, Paramedic
▪ Mr John Bunni, MBChB (Hons), Dip Lap Surg, FRCS [ASGBI Medal], Consultant Colorectal and General Surgeon
▪ Dr Elizabeth Burton, MBChB, Retired General Practitioner
▪ Dr David Cartland, MBChB, BMedSci, General practitioner
▪ Catherine Cassell, RGN, Practice Nurse
▪ Angela Chamberlain, BSc (hons), Midwife
▪ Dr Peter Chan, BM, MRCS, MRCGP, NLP, General Practitioner, Functional medicine practitioner
▪ Dr Selena Chester, MBBS, Medical Practitioner
Dr Marco Chiesa, MD, FRCPsych, Consultant Psychiatrist & Visiting Professor, UCL
Dr Bernard Choi MBBS MRCGP DCH DRCOG General Practitioner
Mr Patrick Chong, MBBS (London) FRCS (Eng) FRCS (Gen Surg), Consultant Vascular Surgeon
▪ Michael Cockayne, MSc, PGDip, SCPHNOH, BA, RN, Occupational Health Practitioner
▪ James Cook, NHS Registered Nurse, Bachelor of Nursing (Hons), Master of Public Health (MPH)
▪ Mr Ian F Comaish, MA, BMBCh, FRCOphth, FRANZCO, Consultant ophthalmologist
▪ Dr Zac Cox, BDS, LCPH, Dental Practitioner
▪ Dr Clare Craig, BMBCh, FRCPath, Pathologist
▪ Dr David Critchley, BSc, PhD in Pharmacology, 32 years’ experience in Pharmaceutical R&D
▪ Dr Sue de Lacy, MBBS, MRCGP, AFMCP UK, Integrative Medicine Doctor
▪ Dr Matthew Dennison, MBBS, MRCGP, Dip IBLM, General Practitioner
▪ Dr Christine Dewbury, MBBS, retired General Practitioner
▪ Dr Keith Dewbury, MBBS, FRCR, retired Consultant Radiologist
▪ Dr Phuoc-Tan Diep, MBChB, FRCPath, Consultant Histopathologist
▪ Dr Jayne LM Donegan, MBBS, DRCOG, DCH, DFFP, MRCGP, General Practitioner
▪ Dr Damien Downing, MBBS, MRSB, private physician
▪ Dr James Dyson, MRCS LRCP, MA, retired Medical Practitioner
▪ Dr Jonathan Eastwood, BSc, MBChB, MRCGP, General Practitioner
▪ Dr Jonathan Engler, MBChB, LlB (Hons), DipPharmMed
▪ Dr Elizabeth Evans, MA(Cantab), MBBS, DRCOG, Retired Doctor
▪ Dr Christopher Exley, PhD, FRSB, Bioinoganic Chemist
▪ Dr Edwin M Field, MBChB, NHS SAS general medicine
▪ Dr Brian Fitzsimons, MBChB, DipOccMed, FRCGP, General Practitioner, Occupational Health Physician, Pre-Hospital Emergency Care Practitioner
▪ Dr John Flack, BPharm, PhD, Retired Director of Safety Evaluation, Beecham Pharmaceuticals 1980-1989 and Senior Vice-president for Drug Discovery 1990-92 SmithKline Beecham
▪ Dr Nick Flatt, BMSc(Hons), MBChB, FRCSEd, FRCA, FFPMRCA, retired Consultant Anaesthetist
Dr Charles Forsyth, MBBS, FFHom, Ecological and Homeopathic Physician (Retired)
Dr Sheena Fraser, MBChB, MRCGP (2003), Dip BSLM, General Practitioner
Dr Emma Fuller, MBChB, MRCGP, General Practioner
▪ Gayle Gerry, BSc Hons, RGN, NHS registered Nurse
▪ Sophie Gidet, RM, Midwife
▪ Dr Henry Goodall, MBBS, FFOM, retired Consultant Occupational Health Physician, President of the Society of Occupational Medicine, 2011-12
▪ Dr Jenny Goodman, MA, MBChB, Ecological Medicine
▪ Cheryl Grainger, BSc, Pharma Training Consultant
▪ Dr Cathy Greig, MBChB (hons), General Practitioner
▪ Dr Fernando M Gundin, MRCGP (2017), General Practitioner
▪ Dr Ali Haggett, Mental health community work, 3rd sector, former lecturer in the history of medicine
▪ Mr David Halpin, MBBS, FRCS, Orthopaedic and trauma surgeon, retired
▪ Dr Catherine Hatton, MBChB, General Practitioner
▪ Mr Anthony Hinton, MBChB, FRCS, Consultant ENT surgeon, London
▪ Dr Renee Hoenderkamp, MBBS, General Practitioner
▪ Dr Richard House, PhD, CPsychol, AFBPsS, CertCouns, Chartered Psychologist, former senior lecturer in Psychology (Roehampton) and Early Childhood (Winchester), retired psychotherapist
▪ Dr Andrew Isaac, MBBCh, Physician, retired
▪ Dr Keith Johnson, BA, DPhil (Oxon), IP Consultant for Diagnostic Testing
▪ Fiona Jones, BScHons, DipPreSci, PgCertMed Ed, MFRPSII, FRPharmS, retired Clinical lead pharmacist
▪ Dr Pauline Jones, MBBS, Retired General Practitioner
▪ Dr Timothy Kelly, MBBCh, BSc, NHS doctor
▪ Dr Gemma Kemp, MBBS FRCPath, Consultant Forensic Pathologist
▪ Eshani King BSc (Hons) FCA CTA BFP – Evidence Based Research in Immunology and Health
▪ Dr Tanya Klymenko, PhD, FHEA, FIBMS, Senior lecturer in Biomedical Sciences
▪ Dr Flora Kogera, MBBS, hospital trainee doctor
▪ Dr Charles Lane, OBE, Molecular Biologist
▪ Dr Caroline Lapworth, MB ChB, General Practitioner
▪ Dr Branko Latinkic, BSc, PhD, Reader in Biosciences
▪ Dr Theresa Lawrie, MBBCh, PhD, Director, Evidence-Based Medicine Consultancy Ltd, Bath
▪ Dr Andrew Lees, MB BS, MRCGP, DCH, retired General Practitioner
▪ Dr Jason Lester, MRCP, FRCR, Consultant Clinical Oncologist
▪ Dr Felicity Lillingstone, IMD DHS PhD ANP, Doctor, Urgent Care, Research Fellow
▪ Dr Nichola Ling, MBBS, MRCOG, Consultant obstetrician and digital advisor to NHS England
▪ Mr Malcolm Loudon, MBChB, MD, FRCSEd, FRCS(Gen Surg), MIHM,VR, Consultant Surgeon
▪ Katherine MacGilchrist, BSc(Hons), MSc, CEO/Systematic Review Director, Epidemica Ltd.
▪ Dr Geoffrey Maidment, MBBS, DRCOG, MD, FRCP, retired consultant physician
▪ Mr Ahmad K Malik, FRCS(Tr & Orth), Dip Med Sport, Consultant Trauma & Orthopaedic Surgeon
▪ Dr Ayiesha Malik, MBChB, MRCGP(2014), General Practitioner
▪ Dr Imran Malik, MBBS, MRCP, MRCGP, General Practitioner
▪ Dr Kulvinder S Manik, MBChB, MRCGP, MA(Cantab), LLM, Gray’s Inn
▪ Dr Fiona Martindale, MBChB, MRCGP, General Practitioner in out-of-hours
▪ Julie Maxwell, MBBCh, MRCPCH, Associate Specialist Community Paediatrician
▪ Dr Fatou Mbow, MD(Italy), MRCGP, DFFP, General Practitioner
▪ Dr Samuel McBride, MBBCh, BAO, BSc, MSc, MRCP (UK) FRCEM, FRCP (Edinburgh), NHS Emergency Medicine & geriatrics
▪ Kaira McCallum, BSc, retired pharmacist, Director of strategy UKMFA
▪ Mr Ian McDermott, MBBS, MS, FRCS(Tr&Orth), FFSEM(UK), Consultant Orthopaedic Surgeon
▪ Dr Janet Menage, MA, MBChB, retired General Practitioner
▪ Dr Kulvinder S. Manik, MBChB, MRCGP, MA(Cantab), LLM, Gray’s Inn
▪ Dr Franziska Meuschel, MD, ND, PhD, LFHom, BSEM, Nutritional, Environmental and Integrated Medicine
▪ Dr Graham Milne, MBChB, MRCGP, DRCOG, General Practitioner
▪ Dr Scott Mitchell, MBChB, MRCS, Associate Specialist, Emergency Medicine
▪ Dr Alistair J Montgomery, MBChB, MRCGP, DRCOG, retired General Practitioner
▪ Dr Alan Mordue, MBChB, FFPH. Retired Consultant in Public Health Medicine & Epidemiology
▪ Dr David Morris, MBChB, MRCP (UK), General Practitioner
▪ Dr Graham Morris, MBChB, MRCP(UK), General Practitioner
▪ Margaret Moss, MA (Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
▪ Dr Claire Mottram, BSc Hons, MBChB, Doctor in General Practice
▪ Theresa Ann Mounsey, RM, BSc (hons), Registered Midwife
▪ Dr Alice Murkies, MBBS, MD, FRACGP, general practitioner and medical researcher
▪ Dr Greta Mushet, MBChB, MRCPsych, retired Consultant Psychiatrist in Psychotherapy
▪ Dr Angela Musso, MD, MRCGP, DRCOG, FRACGP, MFPC, General Practitioner
▪ Dr Sarah Myhill, MBBS, Retired General Practitioner
▪ Mr Colin Natali, BSc(hons) MBBS, FRCS (Orth), Consultant Spinal Surgeon
▪ Dr Chris Newton, PhD, Biochemist working in immuno-metabolism
▪ Julie Nicholls, LCSP(Phys), IEMT, former RGN, Body-Mind Coach
▪ Dr Rachel Nicoll, PhD, Medical researcher
▪ Tim Nike, Specialist Neurological Physiotherapist
▪ Sue Parker Hall, CTA, MSc (Counselling & Supervision), MBACP, EMDR. Psychotherapist
▪ Dr Dean Patterson, MBChB FRCP, Consultant Cardiologist
▪ Dr Christina Peers, MBBS, DRCOG, DFSRH, FFSRH, Menopause Specialist
▪ Rev Dr William J U Philip, MBChB, MRCP, BD, Senior Minister The Tron Church, Glasgow, formerly physician specialising in cardiology
▪ Anna Phillips, RSCN, BSc Hons, Clinical Lead Trainer Clinical Systems (Paediatric Intensive Care)
▪ Dr Julia Piper, FRCGP, BM BS, BMedSci, DFFP, AFMCP, DipOccMed, DipMedAcc
▪ Dr Angharad Powell, MBChB, General Practitioner
▪ Dr Gerry Quinn, PhD, Postdoctoral researcher in microbiology and immunology
▪ Dr Naomi Riddel, MBBCh, MSc, MRCPsych, Consultant Child Psychiatrist
▪ Jessica Righart, MSc, Senior Biomedical Scientist
▪ Mr Angus Robertson, BSc(Med Sci), MBChB, FRCS(Ed), FFSEM(UK), Consultant Orthopaedic Surgeon
▪ Dr Jessica Robinson, BSc(Hons), MBBS, MRCPsych, MFHom, Integrative Medicine Doctor
▪ Dr Jon Rogers, MBChB(Bristol), MRCGP, DRCOG, Retired NHS General Practitioner
▪ Mr James Royle, MBChB, FRCS, MMedEd, Colorectal surgeon
▪ Dr Alison Sabine, MBChB, MRCP, Consultant Rheumatologist
▪ Dr Salmaan Saleem, MBBS, BMedSci, General Practitioner
▪ Dr Roland Salmon, MBBS, MRCGP, FFPH, Former Director, Communicable Disease Surveillance Centre Wales
▪ Dr Alia Sarwar, MBChB, General Practitioner Dr Salmaan Saleem, MBBS, BMedSci, MRCGP, General Practitioner
▪ Dr Charlie Sayer, MBBS, FRCR, Consultant Radiologist
▪ Sorrel Scott, Grad Dip Phys, Specialist Physiotherapist in Neurology, 30 years in NHS
▪ Dr Rohaan Seth, BSc(hons), MBChB (hons), MRCGP, Retired General Practitioner
▪ Dr Rajendra Sharma, MBBCh, BAO, LRCP&S(Ire), MFHom, Private Doctor, Medical Director, Dr Sharma Diagnostics
▪ Dr Haleema Sheikh, MRCGP, General Practitioner
▪ Dr Magdalena Stasiak-Horkan MBBS, MRCGP (2017), DCH, General Practitioner
▪ Natalie Stephenson, BSc (Hons) Paediatric Audiologist
▪ Marco Tullio Suadoni, RN, BSc (Hons) Adult Nursing, MSc, Specialist Palliative Care Lead
▪ Matthew Taylor, retired Paramedic
▪ Dr Jasmine Thomas, MBBS, NHS doctor
▪ Dr Noel Thomas, MA, MBChB, DObsRCOG, DTM&H, MFHom, Retired Doctor
▪ Dr Stephen Ting, MBCHB, MRCP, PhD, Consultant Physician
▪ Dr Julian Tomkinson, MBChB, MRCGP, PCME, General Practitioner, GP Trainer
▪ Suzanne Tomkinson, BSc, MSc, CSci, FIBMS, Senior Biomedical Scientist (Clinical Biochemistry)
▪ Dr Livia Tossici-Bolt, PhD, retired Clinical Scientist
▪ Dr Fodhla Treacy, MBBS, MRCGP, General Practitioner
▪ Dr Jannah van der Pol, iBSc, MBBS, MRCGP, General Practitioner
▪ Dr Helen Westwood, MBChB, MRCGP, DCH, DRCOG, General Practitioner
▪ Dr Carmen Wheatley, DPhil, Orthomolecular Oncology
▪ Dr Samuel White, MBChB, MRCGP, Functional Medicine Specialist, former General Practitioner
▪ Mr Lasantha Wijesinghe, FRCS, Consultant Vascular Surgeon
▪ Dr Ruth Wilde, MBBCh, MRCEM, AFMCP, Integrative & Functional Medicine Doctor
▪ Dr Lucie Wilk, MD, MRCP, Rheumatologist
▪ Dr Julia Wilkens, FRCOG, MD, Consultant in Obstetrics & Gynaecology
▪ Dr David Williams, retired General Practitioner
▪ Dr Stefanie Williams, MD, Dermatologist
▪ Dr Anne Wynne-Simmons, MBBS, MRCGP, General Practitioner, retired
▪ Dr Holly Young, BSc, MBChB, MRCP, Consultant Palliative Care Medicine
▪ Dr AZ, MBChB, NHS Specialty doctor
▪ Dr Ruqia Zafar, MBChB, MRCGP, General Practitioner
REFERENCES
- https://ccvac.org.uk
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: the epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Weekly. Accessed February 20, 2020. http://weekly.chinacdc.cn/en/article/id/e53946e2–c6c4–41e9–9a9b–fea8db1a8f51
- Deaths in Children and Young People in England following SARS-CoV-2 infection during the first pandemic year: a national study using linked mandatory child death reporting data. C Smith, D Odd, R Harwood et al. medRxiv 2021.07.07.21259779; doi: https://doi.org/10.1101/2021.07.07.21259779
- Predicted COVID-19 fatality rates based on age, sex, comorbidities and health system capacity Ghisolfi S, et al. https://gh.bmj.com/content/bmjgh/5/9/e003094.full.pdf
- Children and young people remain at low risk from COVID-19 mortality: updated time trends from USA, United Kingdom, Italy, Germany, Spain, France and South Korea. Bhopal SS, Bagaria J, Olabi B, Bhopal R. https://www.thelancet.com/action/showPdf?pii=S2352-4642%2821%2900066-3
- https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/we eklyprovisionalfiguresondeathsregisteredinenglandandwales/2020 (published 12th January 2021)
- https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/d atasets/analysisofpopulationestimatestoolforuk
- Clinical characteristics of children and young people admitted to hospital with covid-19 in United Kingdom: prospective multicentre observational cohort study. Swann O V, Holden K A, Turtle L et al. BMJ 2020; 370 :m3249 https://www.bmj.com/content/370/bmj.m3249
- Risk factors for intensive care admission and death amongst children and young people admitted to hospital with COVID-19 and PIMS-TS in England during the first pandemic year. Ward JL, Harwood R, Smith C et al. Nat Med 28, 193–200 (2022). https://doi.org/10.1038/s41591-021-01627-9
- SARS-CoV-2 infection in the context of Kawasaki disease and multisystem inflammatory syndrome in children. Folga BA, Karpenko CJ, Grygiel-Górniak B. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9672612/
- Assessment of 135 794 Pediatric Patients Tested for Severe Acute Respiratory Syndrome Coronavirus 2 Across the United States. Bailey LC, Razzaghi H, Burrows EK, et al. JAMA Pediatr. 2021;175(2):176–184. doi:10.1001/jamapediatrics.2020.5052
- Illness duration and symptom profile in symptomatic UK school-aged children tested for SARS-CoV2. Molteni E, Sudre CH, anas LS et al. 2021. The Lancet Child & Adolescent Health. 5: 708-718 https://doi.org/10.1016/S2352–4642(21)00198–X
- Mental health of Adolescents in the Pandemic: Long-COVID19 or Long-Pandemic Syndrome? Blankenburg J, Wekenborg MK, Reichert J et al. medRxiv 2021.05.11.21257037; doi: https://doi.org/10.1101/2021.05.11.21257037
- Fan Yang et al. Shared B cell memory to coronaviruses and other pathogens varies in human age groups and tissues. Science 372,738-741(2021). https://doi.org/10.1126/science.abf6648
- Pre-activated antiviral innate immunity in the upper airways controls early SARS-CoV-2 infection in children. Loske J, Röhmel J, Lukassen S et al. Nat Biotechnol 40, 319–324 (2022). https://doi.org/10.1038/s41587-021-01037-9
- Why is COVID-19 less severe in children? A review of the proposed mechanisms underlying the agerelated difference in severity of SARS-CoV-2 infections. Zimmermann P, Curtis N. Archives of Disease in Childhood 2021;106:429-439. https://adc.bmj.com/content/106/5/429
- https://www.gov.uk/government/publications/ofsted-annual-report-201920-education-childrensservices-and-skills/the-annual-report-of-her-majestys-chief-inspector-of-education-childrens-servicesand-skills-201920
- Children in the Time of Covid. Anne Longfield OBE Children’s Commissioner for England (2020). https://assets.childrenscommissioner.gov.uk/wpuploads/2020/09/cco-childhood-in-the-time-of-covid.pdf
- Impacts of school closures on physical and mental health of children and young people: a systematic review. Viner R et al. 11/02/2021. https://assets.publishing.service.gov.uk/media/60dee6dbd3bf7f7c2f6d7bb5/s1114_school_closure.pdf
- ‘SAFEST PLACE FOR THEM’ Gavin Williamson slaps down unions who don’t want schools to reopen warning there ‘will be consequences’ 16th May 2020. https://www.thesun.co.uk/news/11639145/gavin-williamson-slaps-down-teaching-unions
- SARS-CoV-2 infection and transmission in educational settings: cross-sectional analysis of clusters and outbreaks in England. Ismail SA, Saliba V, Lopez Bernal J, Ramsay ME, Ladhani SN. Lancet Infect Dis. 2021 Mar;21(3):344-353. doi: 10.1016/S1473-3099(20)30882-3
- Risk of hospital admission with covid-19 among teachers compared with healthcare workers and other adults of working age in Scotland, March 2020 to July 2021: population based case-control study. Fenton L, Gribben C, Caldwell D et al. BMJ 2021;374:n2060. http://dx.doi.org/10.1136/bmj.n2060
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1018607/S1374_Supplementary_Information_-Comparison_of_children_and_young_people_admitted_with_SARS-CoV-2.pdf
- Physical interventions to interrupt or reduce the spread of respiratory viruses. Jefferson T, Del Mar CB, Dooley L et al. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006207.pub5/full
- https://www.hartgroup.org/letter-to-cmo-chief-scientist/
- Face masks introduced in English secondary schools to avoid ‘argument’ with Sturgeon. The Lockdown Files. https://www.telegraph.co.uk/news/2023/03/01/nicola-sturgeon-boris-johnson-school-face-mask-rowwhatsapp
- Child mask mandates for COVID-19: a systematic review. Sandlund J, Duriseti R, Ladhani SN, et al Archives of Disease in Childhood Published Online First: 02 December 2023. https://doi.org/10.1136/archdischild-2023-326215
- Is the Liverpool Sars-Cov-2 screening project a true pilot study or the start of mass screening? Jones RAK, 11/11/2020, https://www.bmj.com/content/371/bmj.m4268/rr
- Screening the healthy population for covid-19 is of unknown value, but is being introduced nationwide. Raffle AE, 09/11/2020, https://blogs.bmj.com/bmj/2020/11/09/screening–the–healthypopulation–for–covid–19–is–of–unknown–value–but–is–being–introduced–nationwide/
- https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006207.pub4/full
- https://www.who.int/publications/i/item/non-pharmaceutical-public-health-measuresformitigating-the-risk-and-impact-of-epidemic-and-pandemic-influenza
- Closing schools is not evidence based and harms children. Lewis SJ, Munro APS, Smith GD, Pollock AM. 23.02.2021. https://doi.org/10.1136/bmj.n521
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/882722/25-options-for-increasing-adherence-to-social-distancing-measures-22032020.pdf
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/888572/4c._200420_SPI-B_return_to_SAGE_CMO_on_facemasks_FINAL_S0208.pdf
- Face coverings for covid-19: from medical intervention to social practice. van der Westhuizen H, Kotze K, Tonkin-Crine S, Gobat N, Greenhalgh T. https://www.bmj.com/content/370/bmj.m3021
- ‘Don’t kill your gran’: Matt Hancock urges young people to stop flouting coronavirus restrictions. 07.09.2020.https://www.dailymail.co.uk/news/article-8705361/Coronavirus-NOT-control-Britain-MattHancock-claims.html
- The longitudinal kinetics of antibodies in COVID-19 recovered patients over 14 months. Eyran T, Vaisman-Mentesh A, Dror Y et al. https://doi.org/10.1101/2021.09.16.21263693
- Children develop robust and sustained cross-reactive spike-specific immune responses to SARSCoV-2 infection. Dowell AC, Butler MS, Jinks E et al. Nat Immunol 23, 40–49 (2022). https://doi.org/10.1038/s41590–021–01089–8
- Pre-activated antiviral innate immunity in the upper airways controls early SARS-CoV-2 infection in children. Loske, J., Röhmel, J., Lukassen, S. et al https://doi.org/10.1038/s41587-021-01037-9
- SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Le Bert N, Tan AT, Kunasegaran K et al. Nature 584, 457–462 (2020). https://doi.org/10.1038/s41586-0202550-z
- Will vaccines provide the way out of lockdown? https://www.standard.co.uk/news/health/vaccineslockdown–covid19–boris–johnson–b704753.html
- https://www.walesonline.co.uk/news/wales–news/full–mark–drakeford–interview–indian–20595866
- https://www.independent.co.uk/news/uk/politics/covid–vaccinated–nightclubs–boris–johnsonb1886734.html
- https://dailysceptic.org/2023/03/08/covid–not–deadly–enough–to–justify–risk–of–fast–track–vaccines–chriswhitty–told–government/
- WHO informal consultation on the guidelines for evaluation of the quality, safety, and efficacy of DNA vaccines, Geneva, Switzerland, December 2019 | npj Vaccines (nature.com)
- reg–considerations–on–rna–vaccines_1st–draft_pc_tz_22122020.pdf (who.int)
- Guidelines on clinical evaluation of vaccines: regulatory expectations, Annex 9. WHO Expert Committee on Biological Standardization Sixty-seventh report. https://cdn.who.int/media/docs/defaultsource/prequal/vaccines/who-trs-1004-web-annex-9.pdf?sfvrsn=9c8f4704_2&download=true
- WHO guidelines on nonclinical evaluation of vaccines, Annex 1. WHO Technical Report Series, No. 927, 2005. https://cdn.who.int/media/docs/default-source/biologicals/annex1nonclinical.p3163.pdf?sfvrsn=d11d7789_3&download=true
- Annual report https://investors.biontech.de/node/7381/html
- Moderna Inc Quarterly report to United States Securities & Exchange Commission. See p69-70. https://www.sec.gov/Archives/edgar/data/1682852/000168285220000017/mrna20200630.htm#i8ebe2c9c2ccd487c851f72dd23b1630b_118
- Nonclinical Evaluation Report, BNT162b2 [mRNA] COVID-19 vaccine (COMIRNATYTM), January 2021. https://www.tga.gov.au/sites/default/files/foi-2389-06.pdf (see Table 4.2, page 45)
- Prenatal Exposure to COVID-19 mRNA Vaccine BNT162b2 Induces Autism-Like Behaviors in Male Neonatal Rats: Insights into WNT and BDNF Signaling Perturbations. Erdogan MA, Gurbuz O, Bozkurt MF et al. https://doi.org/10.1007/s11064-023-04089-2
- WHO good manufacturing practices for biological products.WHO Expert Committee on Specifications for Pharmaceutical Preparations. (2016). https://www.who.int/publications/m/item/trs996-annex3
- Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Schmeling M, Manniche V, Hansen PR. https://doi.org/10.1111/eci.13998
- The EMA covid-19 data leak, and what it tells us about mRNA instability. Serena Tinari. 10-03-2021. https://www.bmj.com/content/372/bmj.n627
- Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Aldén M, Olofsson Falla F, Yang D et al. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8946961/
- https://www.researchgate.net/profile/Jessica-Rose-24/publication/374870815_Speicher_DJ_et_al_DNA_fragments_detected_in_COVID-19_vaccines_in_Canada_DNA_fragments_detected_in_monovalent_and_bivalent/links/653754ee24bbe32d9 a69c6b9/Speicher-DJ-et-al-DNA-fragments-detected-in-COVID-19-vaccines-in-Canada-DNA-fragmentsdetected-in-monovalent-and-bivalent.pdf?_tp=eyJjb250ZXh0Ijp7ImZpcnN0UGFnZSI6InB1YmxpY2F0aW9uIiwicGFnZSI6InB1YmxpY2F0a W9uIn19
- Characterization and Qualification of Cell Substrates and Other Biological Materials Used in the Production of Viral Vaccines for Infectious Disease Indications. https://www.fda.gov/media/78428/download (page 37)
- N1-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting. Mulroney, T.E., Pöyry, T., Yam-Puc, J.C. et al. Nature (2023). https://doi.org/10.1038/s41586-023-06800-3
- Understanding the Pharmacology of COVID-19 mRNA Vaccines: Playing Dice with the Spike? Cosentino M, Marino F. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9502275/
- Summary Basis for Regulatory Action https://www.fda.gov/media/151733/download (page 17, para 3)
- https://www.icmra.info/drupal/en/covid–19/statement_on_continuation_of_vaccine_trials
- https://www.nejm.org/doi/suppl/10.1056/NEJMoa2110345/suppl_file/nejmoa2110345_appendix.pdf (Table S4 on page 11)
- https://openvaers.com/covid–data
- https://web.archive.org/web/20210822073312/https://www.gov.uk/government/publications/c oronavirus–covid–19–vaccine–adverse–reactions/coronavirus–vaccine–summary–of–yellow–cardreporting
- https://community.covidvaccineinjuries.com/compilation–peer–reviewed–medical–papers–ofcovid–vaccine–injuries/
- ABPI Code Of Practice For The Pharmaceutical Industry 2021. https://www.pmcpa.org.uk/media/3406/2021-abpi-code-of-practice.pdf
- https://www.gmc–uk.org/–/media/documents/gmc–guidance–for–doctors—decision–making–andconsent–english_pdf–84191055.pdf?la=en&hash=BE327A1C584627D12BC51F66E790443F0E0651DA
- https://www.hartgroup.org/open–letter–to–the–gmc/
- https://www.hartgroup.org/how–do–doctors–stand–legally–if–a–patient–is–vaccine–injured/
- The Medicines for Human Use (Clinical Trials) Regulations 2004. https://www.legislation.gov.uk/uksi/2004/1031/pdfs/uksi_20041031_en.pdf
- http://portal.unesco.org/en/ev.php–URL_ID=31058&URL_DO=DO_TOPIC&URL_SECTION=201.html
- Children and clinical research: Ethical issues. Nuffield Council on Bioethics. May 2015. https://www.nuffieldbioethics.org/publications/children-and-clinical-research
- Oxford Vaccine Group on Twitter: “We have a new COVID-19 study open for recruitment. If your child is aged 6-17 years and in good health they may be eligible to participate. Click on the link to find out more.”13 February 2021 https://twitter.com/OxfordVacGroup/status/1360515657910136833
- AstraZeneca children’s trial breaches Helsinki, https://www.hartgroup.org/az-trial-breaches-helsinki/
- Incidents after vaccination with AstraZeneca’s COVID-19 vaccine. 07/03/2021. https://www.basg.gv.at/en/market-surveillance/official-announcements/detail/zwischenfaelle-nachimpfung-mit-covid-19-impfstoff-von-astrazeneca
- https://www.businessinsider.com/astrazeneca–covid–vaccine–countries–suspend–denmark–thailandbatch–blood–clots–2021–3?r=US&IR=T
- https://www.gov.uk/government/publications/use–of–the–astrazeneca–covid–19–vaccine–jcvistatement/jcvi–statement–on–use–of–the–astrazeneca–covid–19–vaccine–7–april–2021
- https://www.gov.uk/government/news/jcvi–advises–on–covid–19–vaccine–for–people–aged–under–40
- Intravenous administration of recombinant adenoviruses causes thrombocytopenia, anemia and erythroblastosis in rabbits. Cichon G, Schmidt HH, Benhidjeb T et al. (1999). https://pubmed.ncbi.nlm.nih.gov/10738553
- https://www.isrctn.com/ISRCTN15638344?q=&filters=ageRange:Child,recruitmentCountry:England&s ort=&offset=134&totalResults=955&page=2&pageSize=100
- Li G, Cappuccini F, Marchevsk NG et al.Safety and immunogenicity of the ChAdOx1 nCoV-19 (AZD1222) vaccine in children aged 6–17 years: a preliminary report of COV006, a phase 2 singleblind, randomised, controlled trial. June 2022. https://doi.org/10.1016/S0140-6736(22)00770-X
- Emergency Use Authorization (EUA) Amendment for an Unapproved Product Review Memorandum. 09/04/2021. https://www.fda.gov/media/148542/download
- Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. https://www.nejm.org/doi/full/10.1056/NEJMoa2116298
- https://www.nejm.org/doi/suppl/10.1056/NEJMoa2116298/suppl_file/nejmoa2116298_protocol.pdf
- EUA amendment request for Pfizer-BioNTech COVID-19 Vaccine for use in children 6 months through 4 years of age. https://www.fda.gov/media/159195/download
- Evaluation of mRNA-1273 Vaccine in Children 6 Months to 5 Years of Age. https://www.nejm.org/doi/full/10.1056/NEJMoa2209367
- https://www.nejm.org/doi/suppl/10.1056/NEJMoa2209367/suppl_file/nejmoa2209367_appendix.pdf (Table S26)
- Less than half UK population to receive coronavirus vaccine, says task force head. 04/10/2020. https://www.ft.com/content/d2e00128–7889–4d5d–84a3–43e51355a751
- https://hansard.parliament.uk/commons/2020–11–10/debates/FB5296EC–628D–4C17–9C284863AC8C07C9/Covid–19Update (Hansard, Column 748)
- BBC One – The Andrew Marr Show, 21/02/2021, Prof John Edmunds: ‘Rapid lockdown easing would cause deaths’ https://www.bbc.co.uk/programmes/p097mrhz (from 6 minutes)
- https://www.telegraph.co.uk/politics/2021/03/23/exclusive–children–line–covid–vaccinesaugust/?WT.mc_id=tmgliveapp_androidshare_Aw3SDXQRqSVx
- https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fstephenhawkingfoundation.org%2Fwp-content%2Fuploads%2F2021%2F03%2FStephen-Hawking-Foundation-Vaccine-
- Schools back mass vaccinations for children as headteachers say ‘peer pressure’ will boost take up. 02.05.2021.https://www.telegraph.co.uk/news/2021/05/02/schools–back–mass–vaccinations–childrenheadteachers–say–peer/
- https://www.dailyrecord.co.uk/news/politics/covid–vaccines–high–school–pupils–24023286
- Vaccinating children against SARS-CoV-2. Lavine J S, Bjornstad O, Antia R. May 2021. https://www.bmj.com/content/373/bmj.n1197
- Dr Rosamond Jones et al. Safety and Ethical Concerns Surrounding COVID-19 Vaccination in Children. 17/05/2021. https://www.hartgroup.org/open–letter–to–mhra–17–05–2021/
- https://openvaers.com/covid–data/child–summaries
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/111 2667/COVID–19_mRNA_Vaccine_BNT162b2__UKPAR___PFIZER_BIONTECH_ext_of_indication_11.6.2021.pdf
- https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/876043/Moral_and_Ethical_Advisory_Group_-_terms_of_reference.pdf
- https://dhexchange.kahootz.com/MEAGpublications/view?objectID=128443589#
- https://www.hartgroup.org/open–letter–to–jcvi–6th–june–2021/
- https://www.gov.uk/government/news/jcvi–issues–advice–on–covid–19–vaccination–of–children–andyoung–people
- https://www.gov.uk/government/publications/covid–19–vaccination–of–children–and–young–peopleaged–12–to–17–years–jcvi–statement/jvci–statement–on–covid–19–vaccination–of–children–and–youngpeople–aged–12–to–17–years–15–july–2021
- Minute of the JCVI Extraordinary Meeting on COVID-19 Immunisation 29 July 2021. https://app.box.com/s/acvlrtpiom6l7krf7szzl2jg5da69sm9/file/1313432054361
- Israel reports link between rare cases of heart inflammation and COVID-19 vaccination in young men. Vogel G & Couzin-Frankel J. https://www.science.org/content/article/israel–reports–link–betweenrare–cases–heart–inflammation–and–covid–19–vaccination
- COVID-19 Vaccination-Associated Myocarditis in Adolescents. Jain SS, Steele JM, Fonseca B et al. 14/08/2021. https://pubmed.ncbi.nlm.nih.gov/34389692/
- Minute of the JCVI Extraordinary Meeting on COVID-19 Immunisation – extraordinary meeting with cardiologists. 01 September 2021. https://app.box.com/s/acvlrtpiom6l7krf7szzl2jg5da69sm9/file/1313437151314
- Long-term follow-up after viral myocarditis established by endomyocardical biopsy: Predictors of mortality. Grün S, Schäufele T, Derin T, Kispert EM, Klingel K, Kandolf R, Sechtem U, Mahrholdt H. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3106486/
- https://www.nymc.edu/news–and–events/news–archives/us–fda–awards–dr–supriya–jain–19–million–tosupport–research–on–covid–19–vaccine–associated–myocarditis.php
- Cardiac manifestations and outcomes of COVID-19 vaccine-associated myocarditis in the young in the USA: longitudinal results from the Myocarditis After COVID Vaccination (MACiV) multicenter study. https://www.thelancet.com/journals/eclinm/article/PIIS2589–5370(24)00388–2/fulltext
- https://www.gov.uk/government/publications/jcvi–statement–september–2021–covid–19–vaccination–ofchildren–aged–12–to–15–years/jcvi–statement–on–covid–19–vaccination–of–children–aged–12–to–15–years–3september–2021
- https://www.gov.uk/government/publications/universal–vaccination–of–children–and–young–peopleaged–12–to–15–years–against–covid–19/universal–vaccination–of–children–and–young–people–aged–12–to15–years–against–covid–19
- https://web.archive.org/web/20210719124031/https://www.gov.uk/government/publications/actionsfor–schools–during–the–coronavirus–outbreak/schools–covid–19–operational–guidance
- https://www.gov.uk/government/publications/impact–on–school–absence–from–covid–19–vaccination–ofhealthy–12–to–15–year–old–children/impact–on–school–absence–from–covid–19–vaccination–of–healthy–12to–15–year–old–children
- https://www.mrc–bsu.cam.ac.uk/now–casting/report–on–nowcasting–and–forecasting–16th–september2021/
- SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: a large, multicentre, prospective cohort study (SIREN). Hall VJ, Foulkes S, Charlett A et al. 09/04/2021 https://doi.org/10.1016/S0140–6736(21)00675–9
- Efrati, S., Catalogna, M., Abu Hamad, R. et al. Safety and humoral responses to BNT162b2 mRNA vaccination of SARS-CoV-2 previously infected and naive populations. Sci Rep 11, 16543 (2021). https://doi.org/10.1038/s41598–021–96129–6
- Education Select Committee, Covid-19 vaccines in Children 22-09-2021. https://committees.parliament.uk/oralevidence/2767/pdf/
- https://theconversation.com/covid–vaccines–for–under–16s–why–competent–children–in–the–uk–canlegally–decide–for–themselves–168047
- https://www.gov.uk/government/news/uk–regulator–approves–use–of–pfizerbiontech–vaccine–in–5–to11–year–olds
- https://www.gov.uk/government/publications/jcvi–update–on–advice–for–covid–19–vaccination–ofchildren–aged–5–to–11/jcvi–statement–on–vaccination–of–children–aged–5–to–11–years–old
- More than 650 British health professionals call for “pause” to child covid roll-out. https://childrensunion.org/ccvac–pause–covid–roll–out/
- https://bnf.nice.org.uk/drugs/covid–19–vaccine/
- Vaccine effectiveness of the first dose of ChAdOx1 nCoV-19 and BNT162b2 against SARS-CoV-2 infection in residents of long-term care facilities in England (VIVALDI): a prospective cohort study. Shrotri M, Krutikov M, Palmer T et al. doi.org/10.1016/S1473–3099(21)00289–9
- Protection by a Fourth Dose of BNT162b2 against Omicron in Israel. Bar-On YM, Goldberg Y, Micha, M et al. https://www.nejm.org/doi/full/10.1056/NEJMoa2201570
- Shrestha NK, Burke PC, Nowacki AS, Simon JF, Hagen A, Gordon SG. Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine. (April 2023) https://doi.org/10.1093/ofid/ofad209
- Effectiveness of the BNT162b2 vaccine among children 5-11 and 12-17 years in New York after the Emergence of the Omicron Variant. Dorabawila V, Hoefer D, Bauer UE, Bassett MT, Lutterloh E, Rosenberg ES. https://doi.org/10.1101/2022.02.25.22271454
- León TM, Dorabawila V, Nelson L, et al. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis — California and New York, May–November 2021. http://dx.doi.org/10.15585/mmwr.mm7104e1
- Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Naturally Acquired Immunity versus Vaccine-induced Immunity, Reinfections versus Breakthrough Infections: A Retrospective Cohort Study, Gazit S, Shlezinger R, Perez G et al. https://doi.org/10.1093/cid/ciac262
- Protection of prior natural infection compared to mRNA vaccination against SARS-CoV-2 infection and severe COVID-19 in Qatar. https://www.medrxiv.org/content/10.1101/2022.03.17.22272529v1.full.pdf
- Shenai MB, Rahme R, Noorchashm H. Equivalency of Protection From Natural Immunity in COVID19 Recovered Versus Fully Vaccinated Persons: A Systematic Review and Pooled Analysis. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8627252/
- https://medicalxpress.com/news/2022–01–sweden–opts–vaccinating–children–aged.html
- https://www.regjeringen.no/en/aktuelt/vaccination–of–children–and–adolescents–against–covid19/id2895513/
- Corona shot for Children https://www.rijksoverheid.nl/onderwerpen/coronavirus–vaccinatie/kinderen
- 107 reports of side effects in children, 11 of which were serious – what does that really mean? https://frettin.is/2022/07/22/107–tilkynningar–um–aukaverkanir–medal–barna–thar–af–11–alvarlegar–hvadthydir–thad–i–raun/
- danish national board of health admits vaccinating kids for covid was a mistake. https://nyheder.tv2.dk/samfund/2022–06–22–set–i–bakspejlet–fik–vi–ikke–meget–ud–af–at–vaccinereboernene–erkender–brostroem
- Under-reporting of adverse drug reactions : a systematic review. Hazell L, Shakir SA. https://pubmed.ncbi.nlm.nih.gov/16689555/
- The Israeli Ministry of Health Actually Did a Survey of Adverse Events after The Booster Dose. Guetzkow J. 18/02/2022. https://jackanapes.substack.com/p/the–israeli–ministry–of–health–actually–db7
- Epidemiology of Acute Myocarditis/Pericarditis in Hong Kong Adolescents Following Comirnaty Vaccination. Chua GT, Kwan MYW, Chui CSL et al. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8767823/
- Myocarditis Following COVID-19 BNT162b2 Vaccination Among Adolescents in Hong Kong.Li X, Lai FTT, Chua GT, et al. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2789584
- https://www.gov.uk/government/publications/covid-19-vaccination-in-children-and-young-peopleaged-16-to-17-years-jcvi-statement-november-2021/joint-committee-on-vaccination-and-immunisationjcvi-advice-on-covid-19-vaccination-in-people-aged-16-to-17-years-15-november-2021
- https://www. /open-letter-to-jcvi-9th-december-2021/
- Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Mansanguan S, Charunwatthana P, Piyaphanee W et al. https://doi.org/10.3390/tropicalmed7080196
- Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination. Buergin N, Lopez-Ayala P, Hirsiger JR et al. https://doi.org/10.1002/ejhf.2978
- BNT162b2 Vaccine-Associated Myo/Pericarditis in Adolescents: A Stratified Risk-Benefit Analysis. Krug A, Stevenson J, Høeg TB. https://doi.org/10.1111/eci.13759
- https://www.gov.uk/government/publications/myocarditis-and-pericarditis-after-covid-19vaccination/myocarditis-and-pericarditis-after-covid-19-vaccination-guidance-for-healthcareprofessionals#further-vaccination
- https://thenationalpulse.com/2023/12/03/watch–dod–whistleblower–says–pilot–heart–failure–spiked1000–after–vax–mandate/
- Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Fraiman J, Erviti J, Mark Jones M et al. https://doi.org/10.1016/j.vaccine.2022.08.036.
- COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities. Bardosh K, Krug A, Jamrozik E, et al. Journal of Medical Ethics Published Online First: 05 December 2022. https://jme.bmj.com/content/early/2022/12/05/jme2022-108449
- A comparative analysis on serious adverse events reported for COVID-19 vaccines in adolescents and young adults. Cappelletti-Montano B, Demuru G, Laconi E, Musio M. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10291619/
- Overall Health Effects of mRNA COVID-19 Vaccines in Children and Adolescents: A Systematic Review and Meta-Analysis. Hoffmann SS, NielsenS, Thysen SM, Duriseti R, Benn CS. https://doi.org/10.1101/2023.12.07.23298573
- In the matter of The Queen (on the application of AB and CD, by their mother and Litigation Friend EF) v The Secretary of State for Health and Social Care and The Joint Committee Vaccination and Immunisation, CO-3001-2021, a non-party application was made for provision by the ONS of disclosure of information as set out in this letter.(pdf provided)
- https://web.archive.org/web/20220824103840/https://www.gov.uk/government/publications/coronavir us–covid–19–vaccine–adverse–reactions/coronavirus–vaccine–summary–of–yellow–card–reporting (table 11)
- Child Death Review to March 2023 https://www.ncmd.info/publications/child–death–data–2023/
- Office for Health Improvement and Disparities. https://app.powerbi.com/view?r=eyJrIjoiYmUwNmFhMjYtNGZhYS00NDk2LWFlMTAtOTg0OGNhNmFiNGM0IiwidCI6ImVlNGUxNDk5LTRhMzUtNGIyZS1hZDQ3LTVmM2NmOWRlODY2NiIsImMiOjh9
- UK Yearly Excess Deaths. https://phinancetechnologies.com/HumanityProjects/yearly%20Excess%20Death%20Rate%20Analysis%20-%20UK.htm
- Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs.Senneff S & McCullough P. https://www.sciencedirect.com/science/article/pii/S027869152200206X
- BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists. Noé A, Dang TH, Axelrad C et al.23/08/2023. https://www.frontiersin.org/articles/10.3389/fimmu.2023.1242380/full
- SARS-CoV-2 Epidemiology and COVID-19 mRNA Vaccine Effectiveness Among Infants and Children Aged 6 Months–4 Years — New Vaccine Surveillance Network, United States, July 2022– September 2023. Tannis A, Englund JA, Perez A, et al. MMWR Morb Mortal Wkly Rep 2023;72:1300–1306. http://dx.doi.org/10.15585/mmwr.mm7248a2
- As an Oncologist I Am Seeing People With Stable Cancer Rapidly Progress After Being Forced to Have a Booster. Professor Angus Dalgleish, November 2023, The Daily Sceptic. https://dailysceptic.org/2022/11/26/as–an–oncologist–i–am–seeing–people–with–stable–cancer–rapidlyprogress–after–being–forced–to–have–a–booster/?highlight=angus%20dalgleish
- UKCauseof DeathProject Death&DisabilityTrends,Ages 15-44:MalignantNeoplasms. October 2023. Carlos Alegria. https://phinancetechnologies.com/HumanityProjects/Resources/Project%20Brief%20-%20UK%20Malignant%20Neoplasms%2015-44_101823.pdf
- UK Death Rate Trends for Malignant Neoplasm: Without Specification of Site (TurboCancers?) November 2023. Carlos Alegria. https://phinancetechnologies.com/HumanityProjects/Resources/UK%20Malignant%20Neoplasms%20-%20Cause%20-%20No%20Site_110723.pdf
- Biological response and cytotoxicity induced by lipid nanocapsules. Szwed M, Torgersen ML, Kumari RV et al. J Nanobiotechnol 18, 5 (2020). https://doi.org/10.1186/s12951-019-0567-y
- SARS-CoV-2 Vaccination and the Multi-Hit Hypothesis of Oncogenesis. Valdes Angues R, Perea Bustos Y (December 17, 2023) https://www.cureus.com/articles/209584–sars–cov–2–vaccination–andthe–multi–hit–hypothesis–of–oncogenesis#!/
- https://hansard.parliament.uk/Commons/2023–10–20/debates/69C5A514–9A04–4ED7–B56B61A3D40E3226/TrendsInExcessDeaths
- https://www.hartgroup.org/trends–in–excess–deaths–20th–october–2023/
- https://hansard.parliament.uk/commons/2024-01-16/debates/152B485D-812D-43CC-9D25-C2B651564810/ExcessDeathTrends
- https://www.societyofeditors.org/soe_news/all-in-all-together-uk-government-partners-withnewspaper-industry-on-covid-19-ad-campaign/
- Don’t miss out! Why young people should get their Covid jab. October 2021. https://metro.co.uk/2021/10/01/dont-miss-out-why-young-people-should-get-their-covid-jab-15337792/
- https://web.archive.org/web/20230213171233/https://www.netmums.com/life/what-this-gp-wantsevery-parent-to-know-about-the-covid-vaccine-and-their-child
- https://www.netmums.com/life/what–this–gp–wants–every–parent–to–know–about–the–covid–vaccineand–their–child
- Decision making and consent. General Medical Council (2020). https://www.gmc-uk.org/-/media/documents/gmc-guidance-for-doctors—decision-making-and-consent-english_pdf-84191055.pdf
- https://www.bbc.co.uk/newsround/57389353.amp
- https://assets.publishing.service.gov.uk/media/6012d7f2d3bf7f05b92f6cfc/BG_2020_Brexit_Final_ver sion.pdf
- https://www.bbc.co.uk/news/health–59488848#:~:text=Administration%20approved%20the–,Pfizer,jab%20for%20five
- https://www.pmcpa.org.uk/cases/completed-cases/auth35911221-a-complaint-on-behalf-ofusforthem-v-pfizer/#:~:text=for%20children%E2%80%99s%20needs%20to%20be%20prioritised%20during%20the%20Covid%20pandemic%20response
- https://web.archive.org/web/20210904133522/https://www.england.nhs.uk/coronavirus/wpcontent/uploads/sites/52/2021/08/C1384–Vaccinating–children–and–young–people–frequently–askedquestions.pdf
- https://www.local.gov.uk/our–support/coronavirus–information–councils/covid–19–serviceinformation/covid–19–vaccinations/behavioural–insights/resources/encouraging–vaccine–take–amongyounger–people
- https://www.gov.uk/government/publications/covid–19–vaccination–autumn–booster–resources/aguide–to–the–covid–19–autumn–programme
- https://www.hartgroup.org/dear–jcvi–how–can–boosters–protect–others/
- https://wonder.cdc.gov/controlle/datarequest/D8;jsessionid=C926AA45E76932525407BE3BC79B
- https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/articles/ provisionalbirthsinenglandandwales/2021#stillbirths
- https://www.heraldscotland.com/news/23259523.expert–review–mystery–spike–scots–baby–deathsbegins/
- https://www.hartgroup.org/inquiry–into–increased–neonatal–deaths–in–scotland–gets–underway/
- https://www.healthcareimprovementscotland.scot/wp-content/uploads/2024/02/20240227-Neonatal-Mortality-Review-Report-FINAL-NO-EMBARGO.pdf
- Data on Neonatal Deaths from Major Israeli Health Insurer Shows Huge Spikes. Joel Guetzkow. https://researchrebel.substack.com/p/data-on-neonatal-deaths-frommajor?utm_source=profile&utm_medium=reader2
- Menstrual disturbances in 12- to 15-year-old girls after one dose of COVID-19 Comirnaty vaccine: Population-based cohort study in Norway. https://doi.org/10.1016/j.vaccine.2022.11.068
- COVID-19 Vaccines: The Impact on Pregnancy Outcomes and Menstrual Function. Thorp JA, Rogers C, Deskevich MP et al. https://www.jpands.org/vol28no1/thorp.pdf
- PREGNANCY AND LACTATION CUMULATIVE REVIEW, Pfizer BioNTech, 20 April 2020. https://icandecide.org/wp-content/uploads/2023/04/125742_S2_M1_pllr-cumulative-review.pdf
- Covid-19 vaccination BNT162b2 temporarily impairs semen concentration and total motile count among semen donors. Gat I, Kedem A, Dviri M, Umanski A, Levi M, Hourvitz A, Baum M. https://doi.org/10.1111%2Fandr.13209
- Decline in birth rates in Europe (in German) R Hagemann, U Lorré, et al Aug 25 2022. https://www.aletheia–scimed.ch/wp–content/uploads/2022/08/Geburtenrueckgang–EuropeDE_25082022_2.pdf
- https://assets.publishing.service.gov.uk/media/614c53a28fa8f56113bf6472/Vaccine_surveillance_rep ort_–_week_38.pdf.
- https://clinicaltrials.gov/study/NCT05815498
- https://www.whatdotheyknow.com/request/nextcove_booster_trial_in_childr_2
- https://www.wma.net/what–we–do/medical–ethics/declaration–of–helsinki/
- https://www.hartgroup.org/nextcove–trial–contravenes–the–declaration–of–helsinki/
- WhatsApp exhibit provided
- FOI reply from Barts & Royal London NHS Trust, provided
- https://childethics.com/payment–compensation/#1652396073278–952504c9–a815
- FOI Internal Review reply from Barts & Royal London NHS Trust, provided
- Berkshire REC committee minutes – 11 April 2023, provided
- https://assets.publishing.service.gov.uk/media/635a731ed3bf7f20d918f02b/Weekly_Flu_and_COVID –19_report_w43__3_.pdf
- https://usforthem2020.substack.com/p/the–real–reason–parents–are–hesitating?utm_source=postemail–title&publication_id=1051965&post_id=140738389&utm_campaign=email–posttitle&isFreemail=true&r=gnlba&utm_medium=email
- Good medical practice guidelines. General Medical Council. (2013) https://www.gmc–uk.org//media/documents/good–medical–practice—english–20200128_pdf–51527435.pdf
- Draft Good medical practice guidelines. General Medical Council (January 2024) https://www.gmcuk.org/–/media/documents/gmp–2024–final—english_pdf–102607294.pdf
- In the end, the AstraZeneca vaccine just wasn’t as good as its rivals. Sarah Knapton. https://www.telegraph.co.uk/news/2023/11/08/how-astrazeneca-vaccine-was-shelved/
- Vaccine rollout to children faces backlash, Camilla Turner, Daily Telegraph. https://www.telegraph.co.uk/news/2021/05/18/vaccine-roll-children-faces-backlash
- https://bigbrotherwatch.org.uk/campaigns/ministry–of–truth/#overview
- Subject Access Request to Department of Culture, Media and Sport, 2023
- https://wherearethenumbers.substack.com/p/an–update–on–my–nhs–conference–cancellation
- https://www.hartgroup.org/joint–open–letter–to–charity–commission/
- https://bigbrotherwatch.org.uk/2023/12/released–military–surveillance–files/
- https://www.hartgroup.org/full–open–letter–to–mhra–17–05–2021/
- https://www.hartgroup.org/mhra–response/
- https://www.hartgroup.org/open–letter–to–mhra–06–06–2021/
- https://www.hartgroup.org/open–letter–to–the–jcvi–19th–august–2021/
- https://www.hartgroup.org/open–letter–to–mhra–23–08–2021/
- https://www.hartgroup.org/open–letter–to–the–chief–medical–officers/
- https://www.hartgroup.org/open–letter–to–mhra–14–11–2021/
- https://www.hartgroup.org/gmc–reply–07–12–2021/
- https://www.hartgroup.org/open–letter–to–the–mhra–regarding–child–death–data/
- https://www.hartgroup.org/open–letter–to–all–members–of–the–fda–vaccines–committee/
- https://www.hartgroup.org/open–letter–2–fda–vaccines–committee/
- https://www.hartgroup.org/open-letter-to-the-secretary-of-state-for-health-social-care/
- Reply, supplied
- https://www.hartgroup.org/a–further–letter–to–the–secretary–of–state/
- https://www.hartgroup.org/open–letter–covid–19–vaccine–associated–myocarditis–a–cumulative–risk/
- https://www.hartgroup.org/com–cov–3–booster–study–for–12–15–year–olds/
- https://www.hartgroup.org/open–letter–to–prime–minister–liz–truss/
- https://www.hartgroup.org/safety–concerns–re–covid–19–vaccinations–in–pregnancy/
- https://www.hartgroup.org/latest–open–letter–to–our–latest–prime–minister/
- https://www.hartgroup.org/safety–concerns–re–covid–19–vaccinations–in–pregnancy–the–rcog–dontthink–so/
- https://www.hartgroup.org/dear–jcvi–how–can–boosters–protect–others/?swcfpc=1
- https://www.hartgroup.org/safety–concerns–remain–re–covid–19–vaccinations–in–pregnancy/
- https://www.hartgroup.org/open–letter–to–mhra–on–vaccines–for–0–5s/
- https://www.hartgroup.org/open–letter–to–the–jcvi–2/
- https://www.hartgroup.org/an–independent–review–of–vaccine–safety–is–urgently–required/
- https://www.hartgroup.org/rcog–still–pushing–covid–vaccines–to–pregnant–women/
- https://www.hartgroup.org/nextcove–trial–contravenes–the–declaration–of–helsinki/?swcfpc=1
