
Overview of evidence post to rollout
In Part 2, we will explore the difficulties in measuring the true extent of adverse reactions from the vaccines, the potential risks associated with different batches of vaccines, and the impact of vaccine rollout on hospital resources and the workforce. (Part 1 covered what was known before the rollout and Part 3 deaths).
The WHO started a campaign in August 2020, pushing the mantra that “no-one is safe until everyone is safe.” This idea penetrated the consciousness of key decision-makers and the injections started to be aimed at healthy and ever younger arms. The decision to do this came long after it was clear these products were not safe.
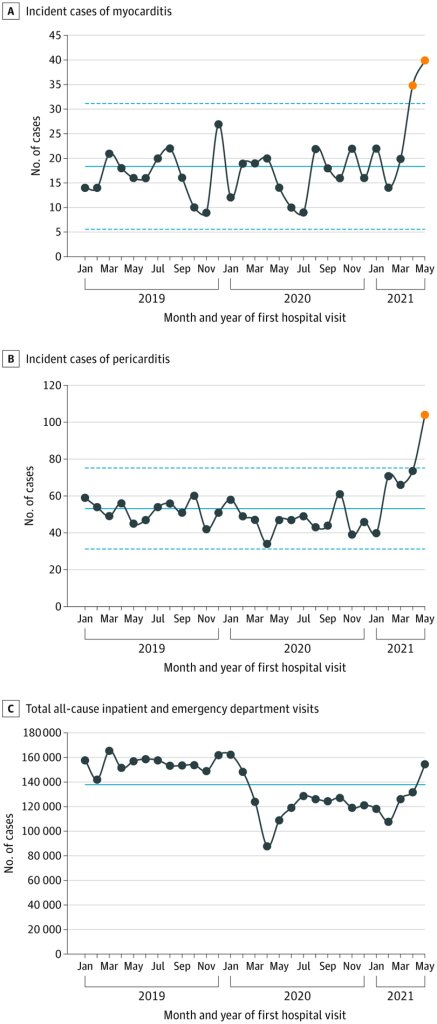
The adverse reaction alarm system started to blare red from January 2021. It was claimed this was due to over reporting because more people were informed about the system. Over the same time period reports for other drugs did not rise. The US VAERS reporting system has been forced to release its data which shows signals of harm for 770 conditions. Two thirds of these showed a stronger safety signal than for myocarditis & pericarditis, which were acknowledged as a genuine adverse event in mid 2021. Because the mechanism of harm is likely to be a combination of impacts on the immune and clotting systems, manifesting in autoimmune attack and small vessel damage, it is not surprising that almost every organ system can be affected. And small vessel damage was not rare with a tripling in the risk of occlusion of the small vessels of the eye, where such damage is easily measured, in the first three months.
How many people were affected?
It has been difficult to measure the adverse reactions from the vaccines for three separate reasons:
- some were uncommon
- some were slow to emerge and
- risks appear to be batch-dependent
Rare side effects like the brain clots and myocarditis are easier to be sure about because the impact on total numbers of those rare conditions is large.
There is an added complication that certain batches of vaccine have had a much higher adverse reaction and death rate than others. A Danish study showed the rates of reports per dose fell into three categories of batch with high, medium or low adverse events. One batch of Pfizer-BioNTech resulted in the hospitalisation of 120 children in Vietnam.
MHRA said they would do a prospective survey of adverse events but never reported on it. A German survey of 500,000 people found events that led to hospitalisation, life changing disability or death occurring in 1 in 142 people, for AstraZeneca and 1 in 500 for Pfizer/BioNTech. Those will include a small number of genuine coincidences. Reports filed by German doctors put the figure for serious reactions at 1 in 3,300 by September 2022.
Vaccine rollout coincided with a rise in pressures on hospital resources. Whereas covid had never resulted in a reduction in the number of empty hospital beds, once the vaccine rolled out there were increasing numbers of inpatients.
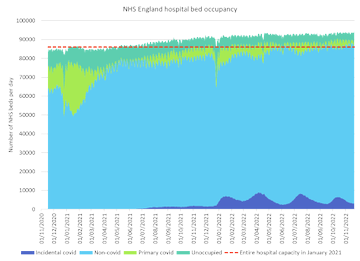
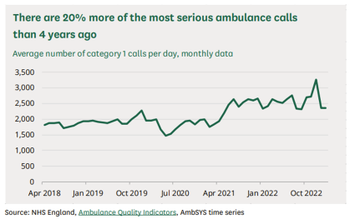
At the same time as there were reports of an accident and emergency crisis in the UK hospitals were overwhelmed in the USA. Covid had never overwhelmed total hospital bed capacity anywhere. All ambulance calls in England for life threatening conditions increased by 25 percent, an extra 500 calls every day from June 2021.
In late 2021, the vaccinated were attending the emergency department five times more frequently than the unvaccinated.
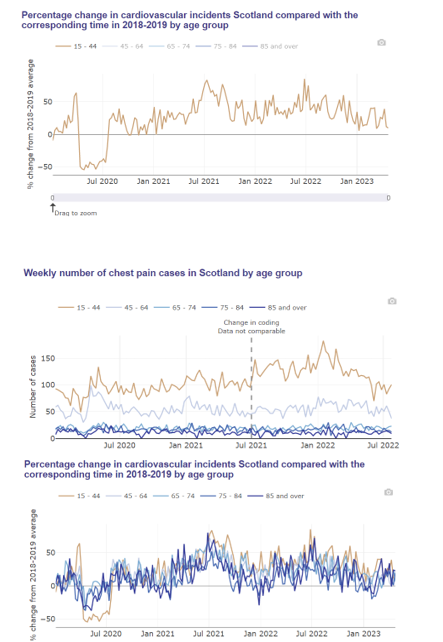
In Israel, there was a 25 percent rise in ambulance calls for cardiac arrests or coronary heart disease among 16 to 39 year olds. The rise was correlated to vaccination and not covid waves. The Scottish data shows a clear rise in cardiac problems in the young.
It was claimed this was all due to the Delta wave or long covid effects. But not everywhere had covid before Omicron; there is a control group.
Australia had had minimal covid prior to the rollout of the vaccines. Yet, their hospitals were also overwhelmed. By May 2021, there was an ambulance crisis even though there were fewer than 100 covid patients in all hospitals in Australia. Despite it being springtime in Australia headlines reported on ambulances unable to drop off patients in hospitals that were at full capacity. Queensland doctors called the problem a “ticking time bomb” in April 2021 and described a “flood of patients.” In April 2022, Yvette D’ath Queensland health minister said she could not explain the rise in the most urgent ambulance calls (“code ones”):
“I don’t think anyone can explain why we saw a 40% jump in code ones… We just had a lot of heart attacks and chest pains and trouble breathing, respiratory issues. Sometimes you can’t explain why those things happen but unfortunately they do.”
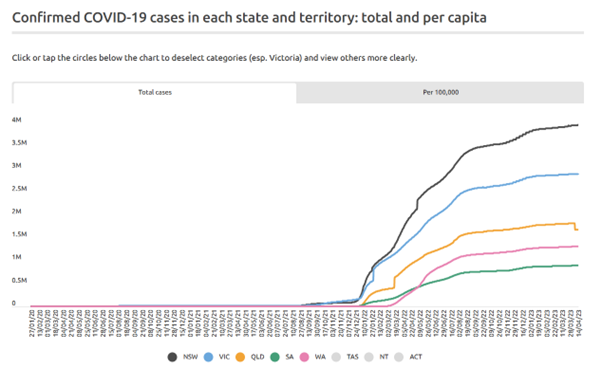
Western Australia and South Australia had almost no covid before Omicron. Up to mid-December 2021, Western Australia had around 1000 cases and South Australia only 1000. The graph shows total cumulative cases by state.
In Oct 2021, Mark McGowan, Premier of Western Australia said he could not explain the overwhelmed hospitals.
“Our hospitals are under enormous pressure. This has been something no-one has ever seen before. Why it is, is hard to know.”
Despite having fewer than 1000 covid cases prior to December 2021, South Australia saw 25,800 extra ambulance calls (mostly cardiac) from July 2020 to June 2021. There was a year on year increase from 2018 to 2019 and 2019 to 2020 but this rise was about double the increase seen in the preceding two years.There was a clear rise in attendances for particular conditions which correlated with the vaccine rollout.
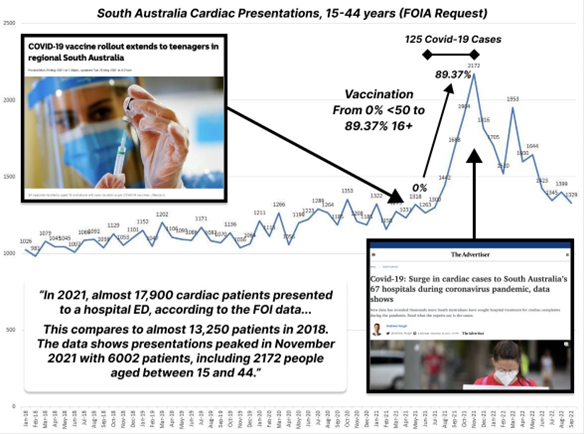
A Freedom of Information request showed that South Australia normally sees around 1,300 cardiac presentations per month for 15-44 year olds. This rose sharply in August 2021 with vaccine rollout, peaking at 2,172 in December. The whole state had seen only 1000 covid cases by 15th December.
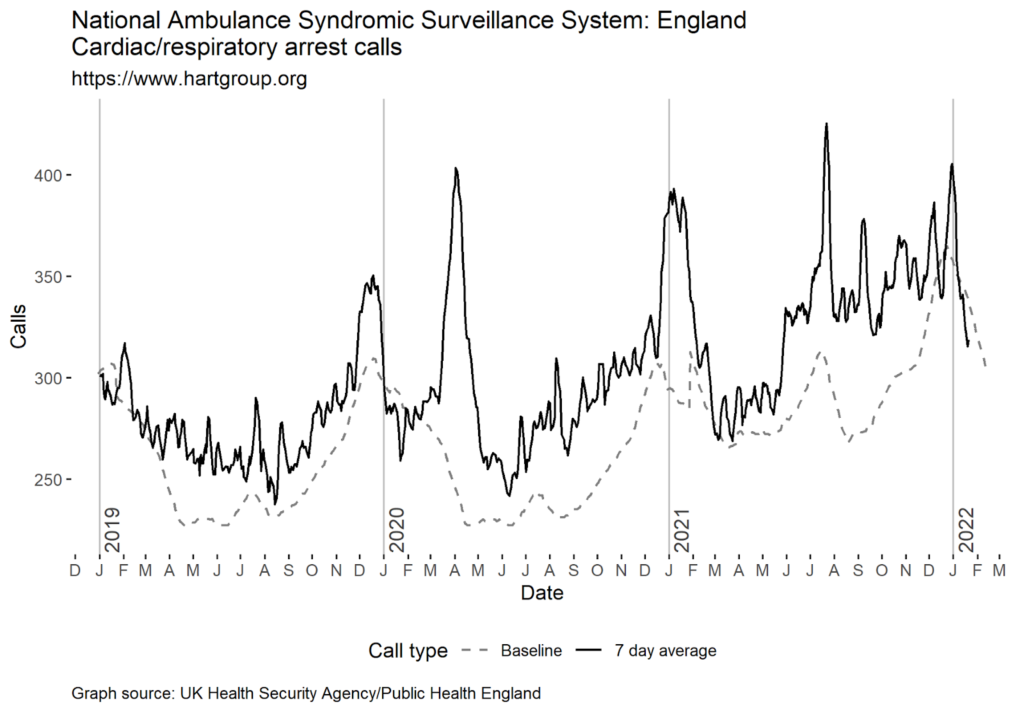
In England, each covid wave saw a rise in cardiac / respiratory arrest calls but there was an additional rise seen from the vaccine rollout, which led to numbers far higher than in previous years. Heart attacks can be caused by direct damage to the electrical circuitry of the heart, e.g. from inflammation or scarring because of myocarditis, or else can be due to slow narrowing of the vessel walls supplying the heart muscle due to inflammation. A time lag should be expected. We have previously written extensively on potential cardiac mechanisms of harm.
There was a notable rise in people who were not working because of long term sickness which was not seen in 2020 but began in spring 2021 when the vaccine was rolled out to the working aged population.
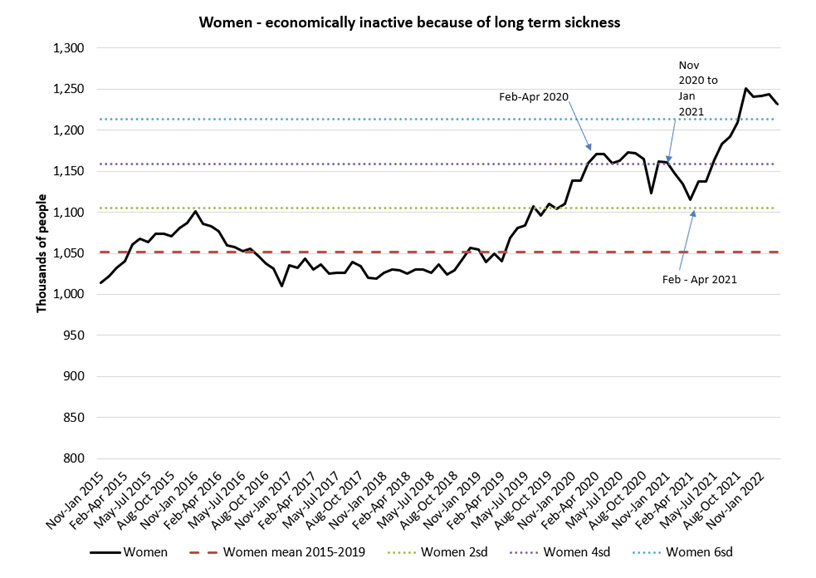
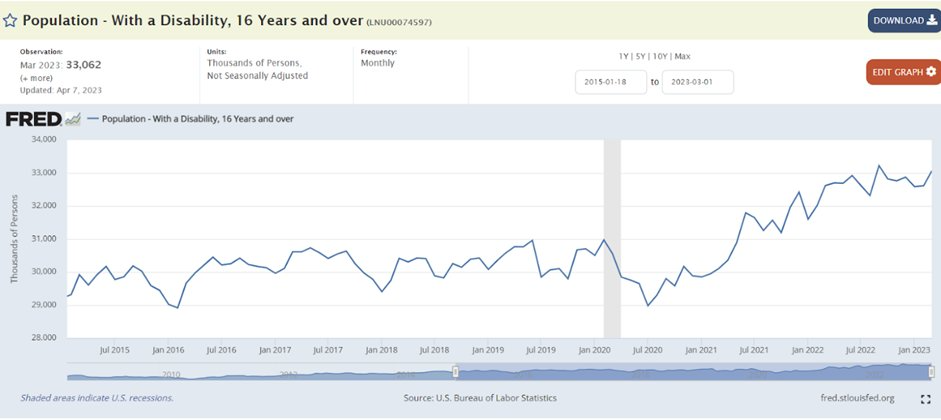
The rise was evident in males and females and also evident in the USA disability data.
In May 2022 the Governor of the Bank of England said there were 320,000 more people not working because they were sick. At the time it was estimated from self reporting that only 80,000 had ever had symptoms of long covid.
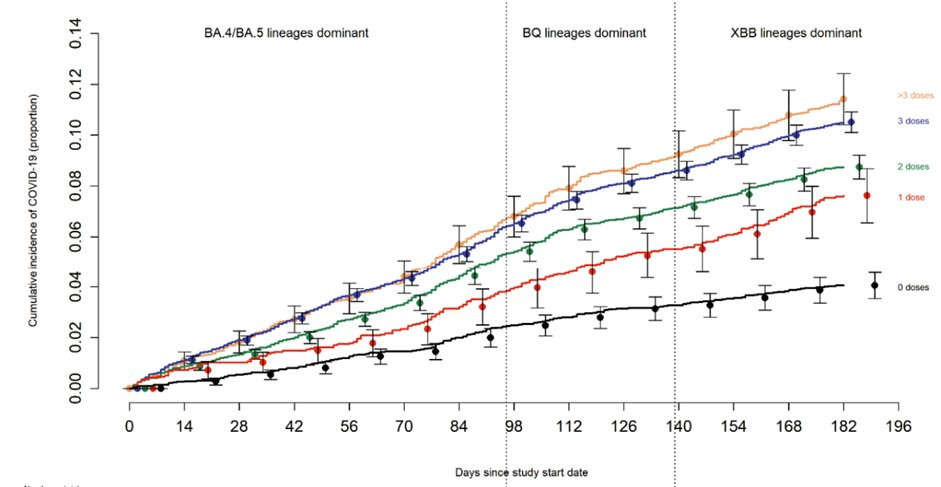
As if that wasn’t bad enough, we now have evidence that the more doses given the higher the covid rates.
In conclusion, the push to vaccinate the world against covid has been one of the most controversial public health campaigns ever. The risks associated with these novel products were downplayed or even ignored. The adverse reaction alarm system has been blaring since early 2021, with reports of serious reactions, hospitalisations, and deaths from COVID-19 vaccines. The rollout of the vaccines has coincided with a rise in hospitalisations and ambulance calls for heart attacks and other serious conditions. The rise in long-term sickness and disability is also concerning. It is clear that these novel products are not without risks, and more research is needed to fully understand the scope of those risks.
