

Why has so much been hidden?
The CEO of Global Research & Development at Pfizer’s lab in Amboise, France has been interviewed by journalist John Leake. He admits huge problems with safety testing,
“I can’t see that there was a real serious strategy for safety.” He particularly highlighted the issues with reproductive toxicology.
Here we review what randomised controlled evidence exists in relation to reproductive toxicity of the Pfizer/BioNTech and Moderna vaccines.
An experiment was carried out injecting Pfizer/BioNTech covid vaccines into rats. Running a well-powered study in rats can easily be done in under 2 months, largely because they have an average gestational period of just 22 days, with 7 pups in a typical litter. The work was outsourced to Charles River Labs, a publicly-listed multi-national animal breeding and Contract Research Organisation, with over 20,000 employees. Did Pfizer use the results of this study to reassure pregnant women? No. For some mysterious reason Pfizer didn’t deign to share the outcome publicly, or even reveal that they had ever done such work. The results were only published after a successful Freedom of Information request to the Australian Regulator in January 2021. The relevant section (6) begins on page 55 (i.e. tucked away at the very end of the report, just before the references).
Three candidate vaccines were used: BNT162b1, BNT162b2 (which was used in the end) and BNT162b3. BNT162b2 codes for the whole spike protein. BNT162b1 and BNT162b3 code for only a specific part of the spike protein (the receptor binding domain). BNT162b1 results in a spike protein that is released by cells whereas with BNT162b3 is coded to remain bound to the cell membrane. They all had the same lipid nanoparticle (LNP) coating.
44 pregnant females were used per candidate, with 22 killed at day 21 (i.e. just before birth, while the other 22 were allowed to litter down, and 4 pups of each sex per litter were analysed at 21 days (any extra pups were apparently culled at day 4 – hopefully selected entirely randomly somehow…).
Pregnancy loss
The study itself was wholly inadequate in terms of numbers of rats but nevertheless showed numerous concerning red flags. First, the rate of pregnancy loss was double in the group that received BNT162b2 (which was the product then chosen to be injected globally into humans) at 9.8% compared to 4.1% in the control (the contents of which was not disclosed). The rate for b1 was 4.8%, effectively acting as a second control group, whereas the rate for b3 was 8.0%, effectively acting as another test group.
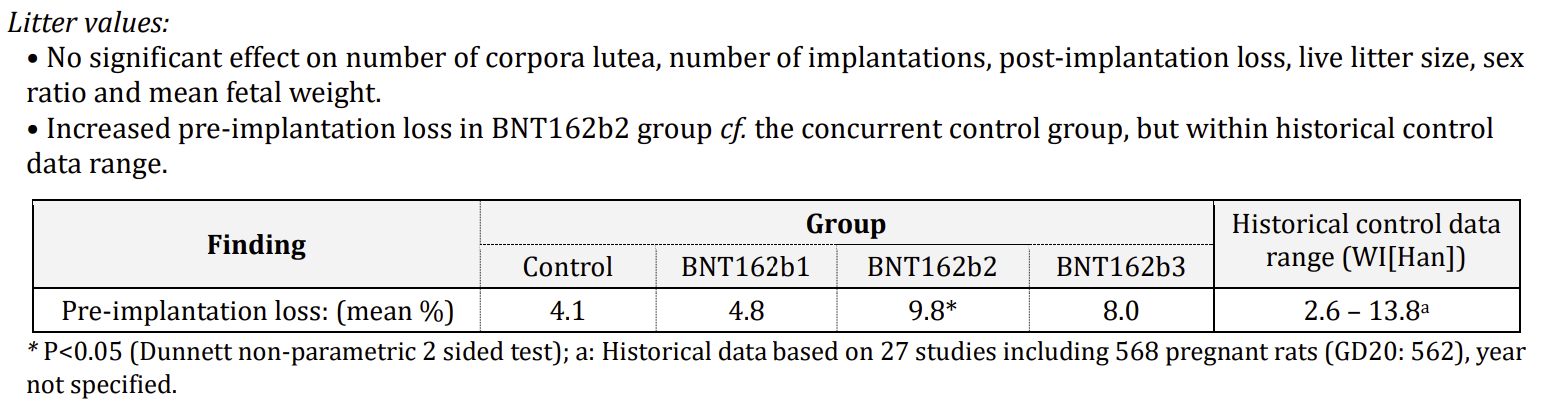
Figure 1: Table from page 55 of the TGA report
Rodents are not humans. In a rodent model with multi-pup litters if some embryos fail very early, it can increase the chance of others surviving to term in a crowded uterus, so the detection of an increased pre-implantation loss may indicate a more serious problem in the human situation, notwithstanding that the eventual litter size for the rodents was not significantly decreased.
This finding, however, was dismissed on the basis of a control group from another experiment which had a higher rate of anomalies. It seems the scientists at Pfizer and the regulators do not know what a control is for! The whole point is to have a group exposed to the same environmental conditions, at the same time and season, in the same cohort of animals so they can be meaningfully compared. At a minimum, these findings should have led to a repeat larger study but they did not.
Fetal anomalies
The report goes on to quantify fetal anomalies. Again, b2 acts as a second control while this time the results from b3 have been completely redacted.
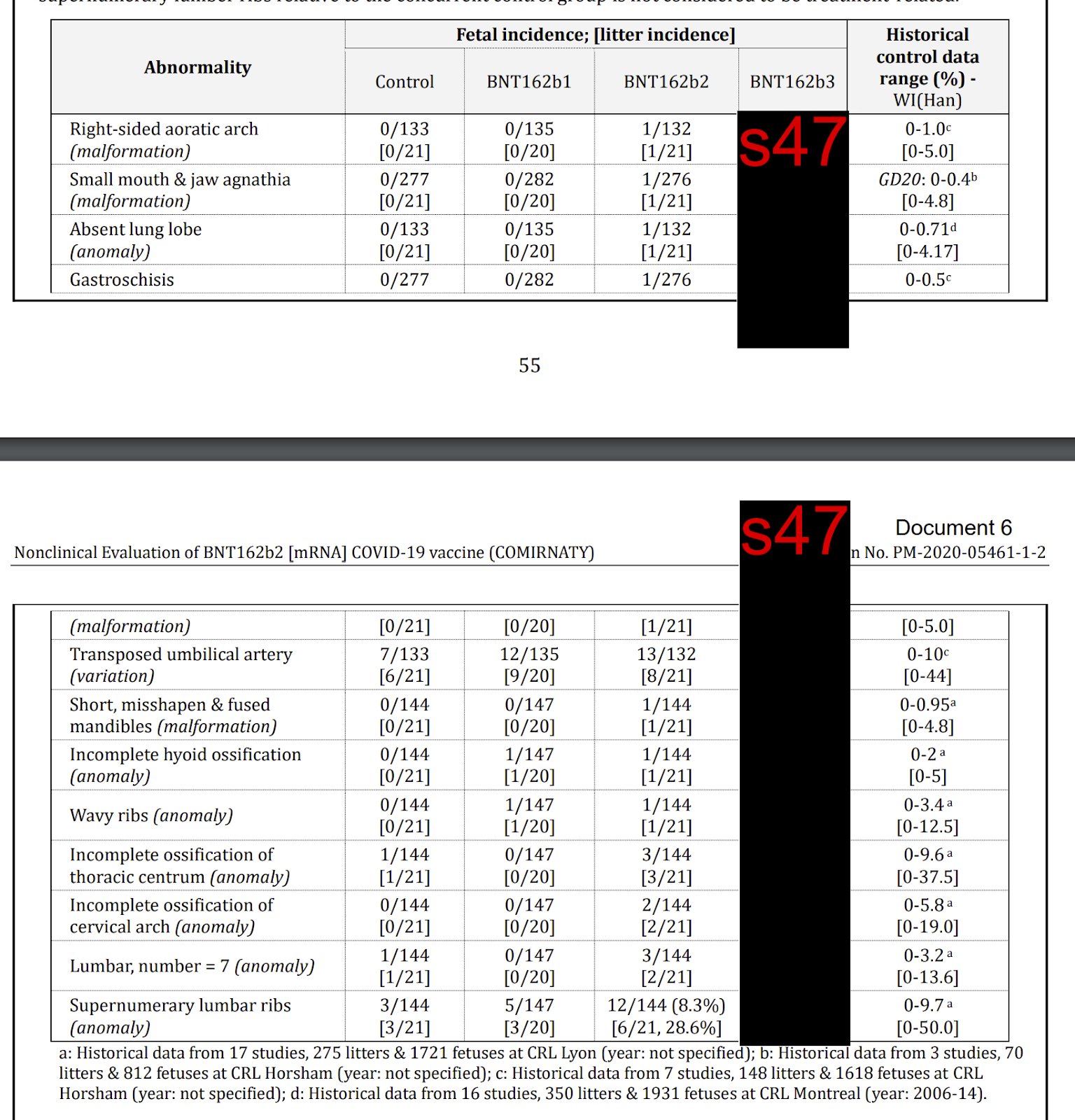
Figure 2: Table from submission to the Australian regulator
Look at the first two columns. The product b1 is again acting like a control in terms of developmental harm. However, when we look at column one and three, we see a huge issue with the product. It is barely believable that this was given to pregnant women across the world, when this data was known to regulators. In every single case, the anomaly rate is higher for the vaccinated mothers. To make matters worse, for the control animals two thirds of the abnormalities searched for came out with zero found, while at least one abnormality in *every* category was found in a pup born to the “vaccinated” mothers. How many people in possession of just this fragment of Pfizer’s own data, would have agreed to take this shot, or encouraged their daughters — or anyone else’s — to take it? These concerning outcomes appear to have been waved away as within “historical norms”.
Claiming those results are within historical norms in terms of a rate of a condition is even more inappropriate when the control group has zero observed, and the experimental group has 1 or more. It is not possible to calculate the incidence increase when the denominator is zero. Furthermore, that would be the case for just one metric, but here it happened multiple times. When every single one of 12 assessed deformations all show the same bias of presenting in the experimental cohort, yet were almost entirely absent in the control group — and when seen, the control incidence was always lower than the experimental cohort — then one has a serious collection of major red-flags that clearly demands repetition with higher numbers to make a proper assessment of the actual increased rate of developmental abnormalities (i.e. at a minimum, one needs results such as seen for the extra ribs in the last row, of 3 vs 12). Overall there were 41 anomalies in the b2 group compared to 19 in the b1 group and 12 in the control. Not providing any statistical analysis of this finding is a huge omission.
Another red-flag on page 55 is simply stated without any further comment: “One female each in the BNT162b1 and BNT162b3 groups were euthanised due to all stillborn pups or total litter death” — once again, with an implied zero incidence of total litter death in the control group, one cannot interpret this, but as it stands that is a 1 in 22 total litter loss event, which happened not once but twice, in two of the vaccine candidates that appear to have caused increased embryonic defects. Shamefully, no replication or further studies were done.
Given that b1 had a better safety profile and was not redacted, it seems reasonable to assume that the redacted unused candidate b3 showed a(n even) worse profile for some or all of litter loss / embryo resorption / birth defects. If that assumption is correct, then the b3 study provided clear evidence to the regulators — prior to mass rollout — that the LNP mediated “vaccines” can cross the placental barrier and harm the fetus in utero. The results from b3 have been almost entirely censored throughout the entire document. Redactions extend throughout the document including the haematology data (p49), serum chemistry (p50), histopathology (p50), immunogenicity (p51), and neutralising antibody titres (p56). One can’t help wondering if the b3 data actually showed that the higher the antibody titre the worse the outcomes, else why redact that otherwise irrelevant data?
Moderna, which is essentially the same product but at three times the dose, made submissions which also showed a “statistically significant” number of rats were born with skeletal changes but the company dismissed these saying they were “not considered adverse.”
Issues with study design
As well as problems with the number of rats used, the dose timing was odd. Organ formation ends by day 15 of rat gestation. Doses were given at 21 and 14 days pre-mating, and then again at gestational day 9 and 20, just a day or two before birth. If you want to know the effect on fetal development, wouldn’t you give a dose earlier in pregnancy?
The doses were given into the muscle only. However, there is no such thing as a pure intramuscular injection. It is well established that 2-3% of intramuscular injections to humans are estimated to end up going intravascular, i.e. injected mainly into the bloodstream, such events being unavoidable even for experienced injectors owing to the highly vascular muscle tissue at the typical site of injection. Given this known risk, wouldn’t you want to inject some of the rats intravenously?
Mechanism of harm
The implied difference between the outcomes in b1 and b3 (implied as the b3 data was redacted, but it seems reasonable to assume it was adverse) is intriguing as they coded for the same antigen. The only difference was that b3 caused the antigen to be bound to the cell membrane whereas the b1 protein would be secreted from the cell. This would lead to cell destruction by T cells. Which cells were destroyed would depend on where the LNPs ended up. Occasional intra-vascular or peri-severed-vascular injection may be an exacerbating factor for subsequent vaccine harms. A higher dose of LNPs can all arrive in an organ in close proximity to each other when entering the vessels as a bolus as Marc Girardot has eloquently explored in his thought-provoking substack and recently released in-depth analysis in The Needle’s Secret. The b2 product that was used also caused membrane expression of foreign protein.
Given the understandable concerns over exposing pregnant women and their babies to experimental genetic medicines, this was an absolutely critical safety study — in fact arguably the most important safety study of all. And had the resultant data been squeaky clean, one would imagine both Pfizer and the coercive Governments would have shared it. But it wasn’t… so they didn’t.
Did this have an impact in the real world?
Abortions can be carried out under a number of legal grounds and Ground E allows for abortion for fetal anomalies where, “there is substantial risk that if the child were born it would suffer from such physical or mental abnormalities as to be seriously handicapped.”
| Date of data | Date published | Number of Ground E abortions | Number of live births | Ground E abortions per 1,000 live births |
| 2017 | 7th June 2018. | 3314 | 679106 | 4.87 |
| 2018 | 13th June 2019 | 3269 | 657076 | 4.98 |
| 2019 | 11th June 2020. | 3183 | 640370 | 4.97 |
| 2020 | 10th June 2021. | 3083 | 613936 | 5.02 |
| 2021 | 21st June 2022. | 3370 | 624828 | 5.39 |
| 2022 | 22nd June 2023 | 1428 (up to June) | 605479 (whole year) | ~4.72 |
| 2023 | Missing | No data | No data | No data |
Table 1: Ground E abnormality abortion data from UK
Each year’s absolute number is lower than the last as the overall birth rate declines, but 2021 reversed the dropping trend with nearly a 10% increase. The writer of the government report got their decimal in the wrong place, and claimed this was only a 1% rise saying: “This is a slight increase since 2020, when there were 3,083 (1%, 287 abortions).” There is no data on how many women received a vaccine in 2021 while pregnant. Based on the number who were vaccinated at delivery, including those vaccinated before pregnancy, only 15 percent of babies born in 2021 were from vaccinated mums, of which there were around 94,000. If the increased fetal abortions were due to the vaccine it works out that at least 1 in every 328 vaccinated pregnant women had a fetal anomaly.
The government said the 2022 data was delayed for a technical reason and would be published on 23rd May 2024. It has not been and there is no sign of the 2023 data either.
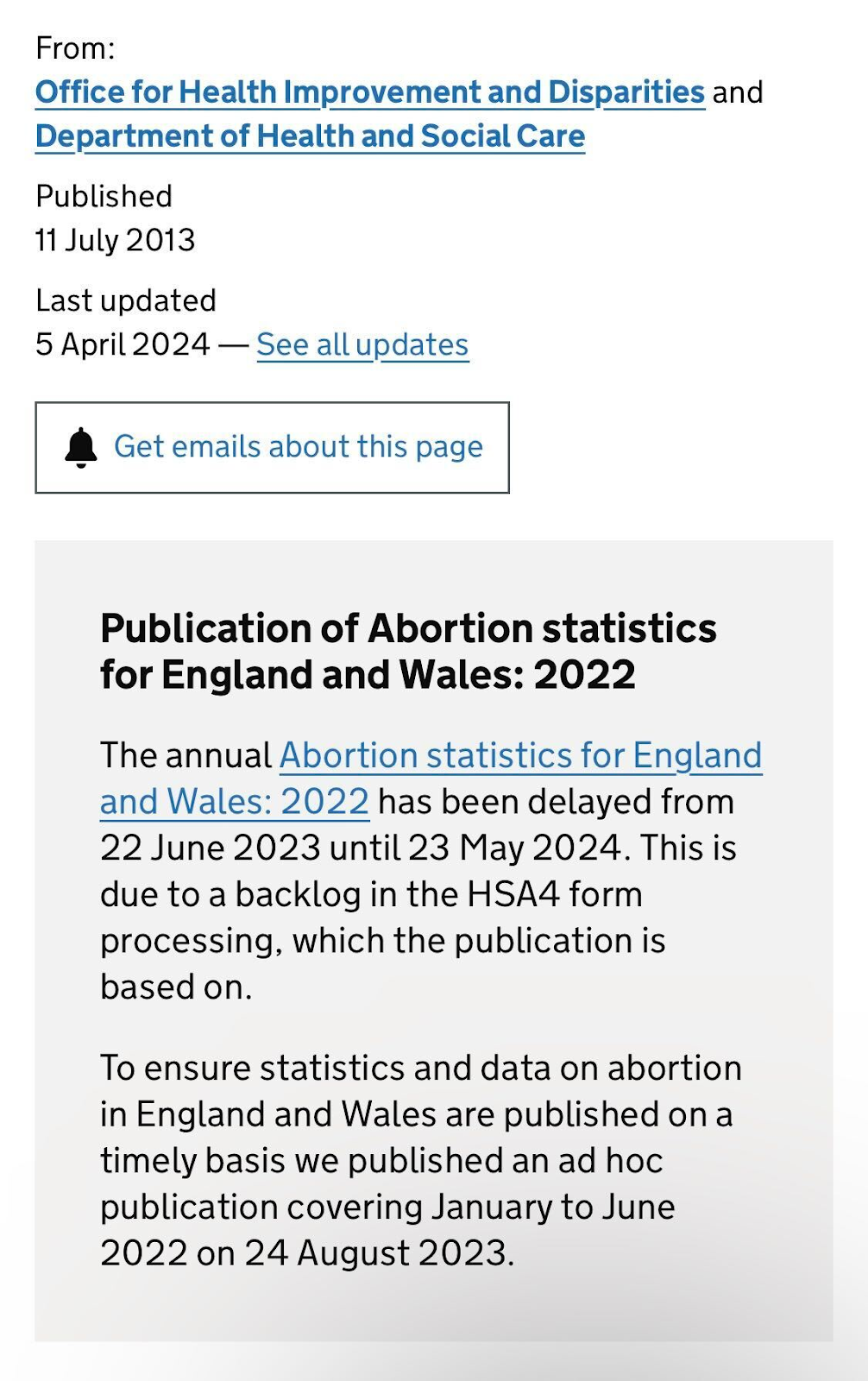
Figure 3: Delay in 2022 data
If only the MHRA would finally release the data from the 2000 pregnant women who were vaccinated in the first half of 2021, that the MHRA said had enrolled for prospectively monitoring, we might begin to be able to answer some crucial questions. Obviously, the outcomes from these births are long ago known by now, yet the MHRA are still refusing FOIA requests for the data, on the feeble basis that it will allegedly (at an as yet undisclosed date) be submitted for publication…
That data is probably stuck in the same black hole as the CDC’s equivalent pregnant vaccinee cohort, published in April 2021. They had to issue a correction over their claimed safety proof, as “No denominator was available to calculate a risk estimate for spontaneous abortions, because at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester.” Strangely, that follow-up data is apparently still not available, 3 years later.
There are still a huge number of people who have been led to believe that vaccines are *definitionally* safe, but here we see 3 candidate vaccines exhibiting different levels of harm to the developing embryo under impartial pre-clinical trial monitoring. We have been told for so long that an intramuscular shot cannot cause harm anywhere else, but this data clearly shows that these vaccines can migrate far away from the injection site, and to such a degree that they can even cross the placental barrier, and harm the developing embryo. The regulators have known this since January 2021 and yet pregnant women have been put under immense pressure to take these products.
Appendix
The raw data from the Charles River experiments is now in the public domain thanks to lawyer Aaron Siri representing the Texan court case.
The percentage of live births (out of all births) shows marked differences thanks to the total litter loss in two dams (female rats).
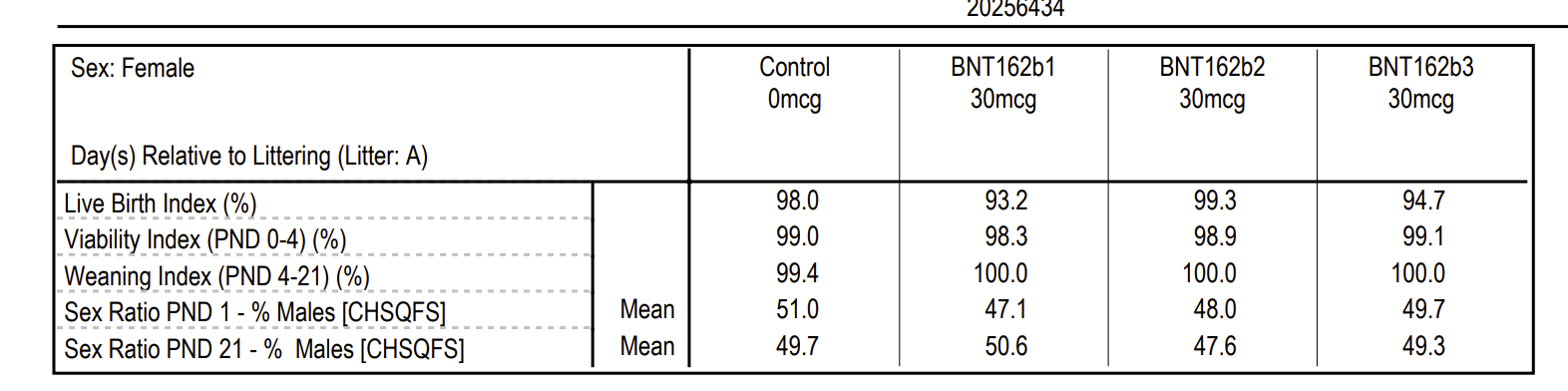
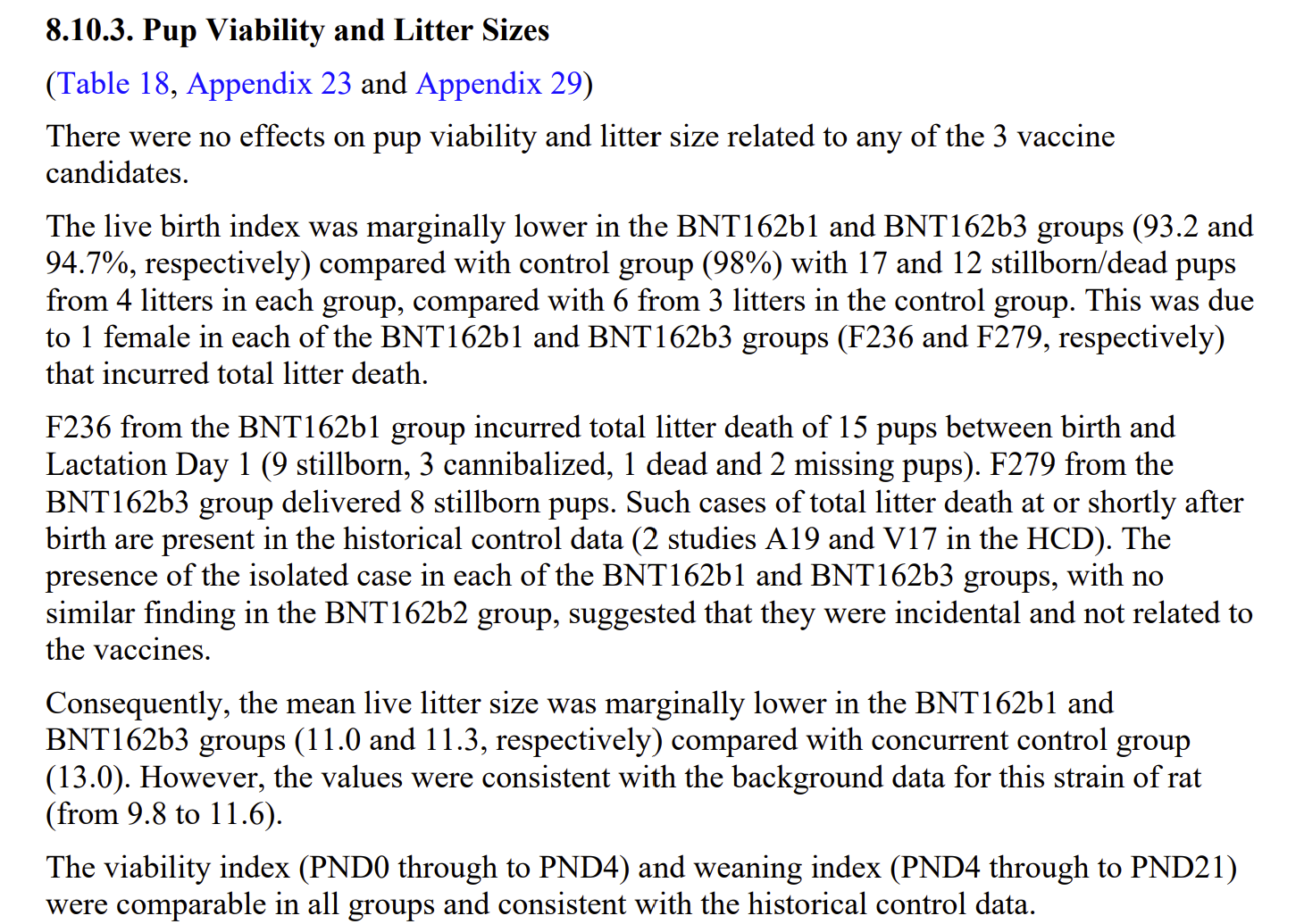
The total litter deaths were dismissed as incidental on the basis that there was “no similar finding in the BNT162b2 group”. This displays a highly concerning lack of awareness of statistics. If total litter loss occurred at a rate as high as 5% then in random groups of 20 there would be no abnormality a third of the time. This is totally in keeping with these results and it is a scandal that a larger study was undertaken immediately.
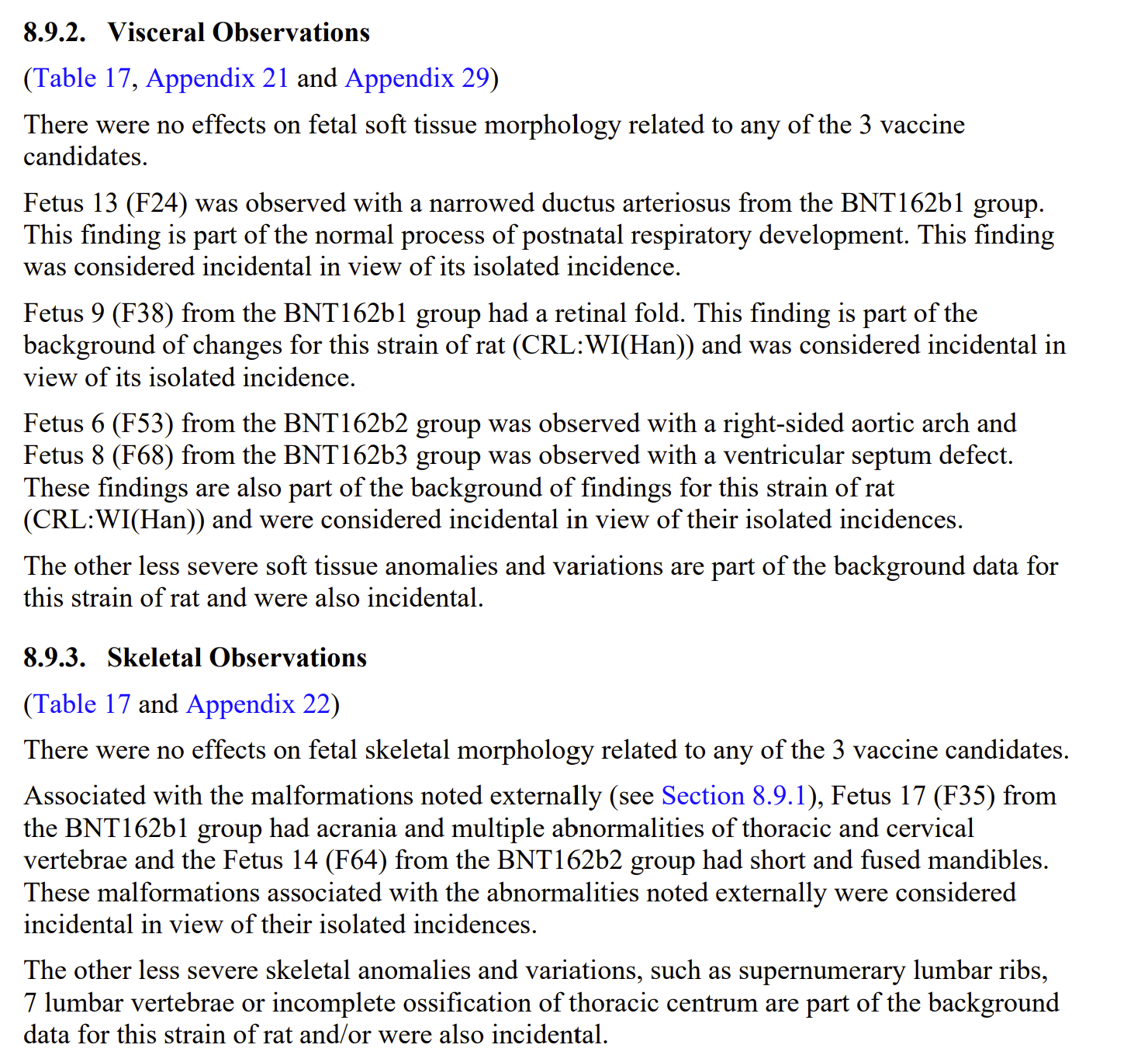
The serious malformations mentioned were only present in the vaccinated groups but were dismissed as incidental:
Readers won’t be surprised to learn that pregnant women are now being recruited to a trial of a new Moderna mRNA vaccine to protect their babies from Respiratory Syncytial Virus (RSV).
Update: 25-08-2025
| Date of data | Date published | Number of Ground E abortions | Number of live births | Ground E abortions per 1,000 live births |
| 2017 | 7th June 2018. | 3314 | 679106 | 4.87 |
| 2018 | 13th June 2019 | 3269 | 657076 | 4.98 |
| 2019 | 11th June 2020. | 3183 | 640370 | 4.97 |
| 2020 | 10th June 2021. | 3083 | 613936 | 5.02 |
| 2021 | 21st June 2022. | 3370 | 624828 | 5.39 |
| 2022 | 22nd June 2023 | 1428 (up to June) | 605479 (whole year) | ~4.72 |
| 2022 | 9th April 2025 | 3124 | 605479 | 5.16 |
Table 1 updated: Ground E abnormality abortion data from UK
Interesting that the 2022 abortion data publication was delayed by almost 2 years. Data for 2023 is still unbpublished.
