

In the only trial in healthy women, for every neural tube defect prevented, NINE babies were lost
Dr Clare Craig
For nearly three decades we have been told a reassuring story. Synthetic folic acid was added to food to prevent neural tube defects – spina bifida and anencephaly (where the brain does not form properly). The trials showed benefit. The surveillance data confirmed success.
Case closed.
But it should not have been.
The apparent benefit may be entirely due to affected babies dying before they could be counted.
1. The Population Data Don’t Show What You Think
The CDC presents graphs showing neural tube defects (NTDs) in live births fell after voluntary US fortification began, with a minor continuing fall when it was mandated in 1998. But those graphs count live births only. They exclude fetal deaths and terminations – right at the time diagnostics was becoming more sensitive.
Figure 1: CDC chart of live births with NTDs[1]
In Europe, the EUROCAT registry tracks all three – live births, fetal deaths, and terminations.[2] The picture looks very different. Live births with NTDs went down. Terminations went up. And the total number of affected pregnancies? Broadly flat over decades. Fewer affected babies were being born – because more were being detected and terminated. The condition itself wasn’t becoming rarer. We were just catching it earlier and then aborting those babies.
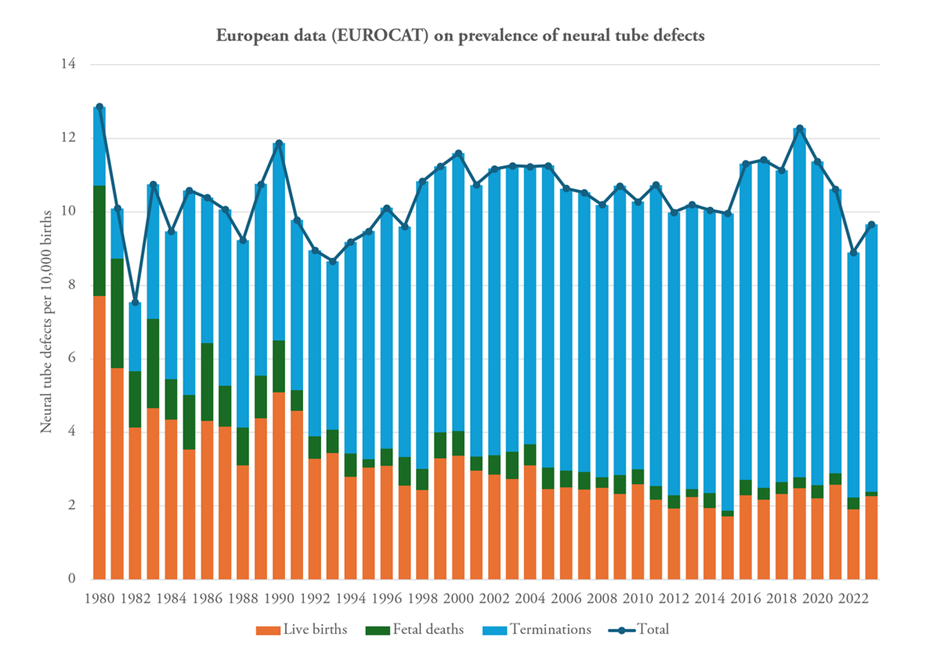
Figure 2: EUROCAT data including terminations[3]
2. The Only Trial in Healthy Women
There were four randomised controlled trials in women at high risk who were given medicinal doses of synthetic folic acid. But there was only one large randomised trial in otherwise healthy women which was the Hungarian Periconceptional Supplementation Trial conducted by Czeizel and Dudás.[4] Women planning pregnancy received either a multivitamin containing 800 micrograms of folic acid, or a trace element supplement (including known neurotoxin manganese – such that the rate of NTDs in the placebo group may have been too high).[5] Around 2,800 treatment and 2,660 placebo pregnancies were evaluated.
The headline result was zero neural tube defects in the multivitamin group versus six in the comparator.
But the same table showed something else:
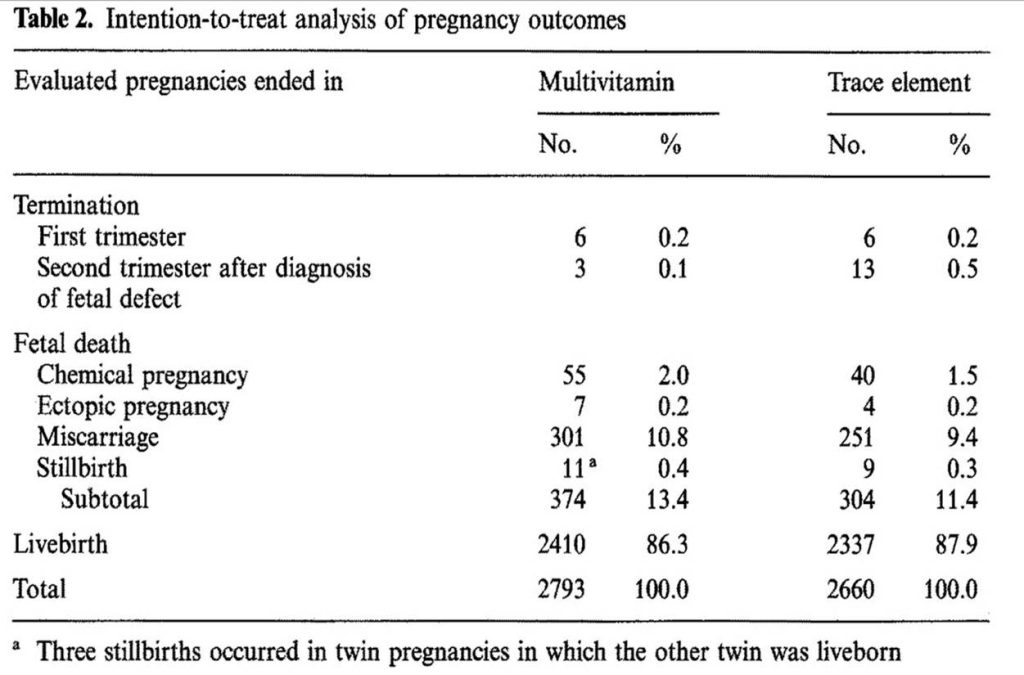
Table 2 from Czeizel, Dudás & Métneki (1994), intention-to-treat analysis.[6]
Every category of fetal death was higher in the folic acid with multivitamin group.[7]
| Synthetic Folic acid and Multivitamin | Trace elements including manganese | Excess | |
| Chemical pregnancy | 55 (2.0%) | 40 (1.5%) | +15 |
| Ectopic pregnancy | 7 (0.25%) | 4 (0.15%) | +3 |
| Miscarriage | 301 (10.8%) | 251 (9.4%) | +50 |
| Stillbirth | 11 (0.4%) | 9 (0.3%) | +2 |
| Total fetal deaths | 374 (13.4%) | 304 (11.4%) | +70 |
| Recognised losses* | 319 (11.4%) | 264 (9.9%) | +55 |
* Recognised losses = miscarriage + ectopic + stillbirth (excluding chemical pregnancies)
Seventy excess fetal deaths. Statistically significant (two-sided Pearson χ² = 4.92, p = 0.027; see statistical note below). Six NTDs prevented. Comparing absolute figures that is 11.7 dead babies for every NTD prevented. But more women fell pregnant in the multivitamin group, so comparing raw numbers isn’t quite fair – we need rates per pregnancy. When you do that, the ratio comes out at nine fetal deaths for every NTD prevented.
Even on the most conservative possible analysis – stripping out chemical pregnancies entirely and counting only clinically recognised losses – the absolute number is 9.2 dead babies for every NTD prevented. Every single subcategory running the same way.
Nine.
Nine dead babies for every NTD prevented. On the most conservative reading of the data. Published in the peer-reviewed literature. Sitting right there in the trial’s own Table 2. The largest statistically significant finding in the entire trial.
How did nobody notice?
They did notice.
3. No dissent allowed
By 1997, folic acid supplementation was being hailed as the most important advance in birth defect prevention since the harm from Thalidomide was recognised. The CDC had recommended it. Fortification of the US flour supply was months away. Questioning folic acid was not a career-enhancing move.
And yet in August 1997, the trial’s own principal investigator, Andrew Czeizel, co-authored a paper in the Lancet with Ernest Hook.[8] They asked whether folic acid might work not by preventing malformations but by selectively killing malformed embryos before birth. They pointed out that their trial had found a statistically significant increase in spontaneous abortion and early fetal death alongside the decrease in birth defects. When a mother kills an infant, we call it infanticide. When a drug kills a fetus, we call it fetotoxicity. When Hook and Czeizel proposed that folic acid might work by selectively killing babies in the womb including those with neural tube defects, they called it: terathanasia. From the Greek – the death of monsters.
The reaction was swift. Judith Hall – Professor of Paediatrics at University of British Columbia, former President of the American Society of Human Genetics, and one of North America’s most senior clinical geneticists – conceded that pathological data on the pregnancy losses – to determine whether malformations were present among the dead – were “highly desirable.”[9] She then claimed it would be “unethical to repeat the trials,” so the needed data could never be collected. In fact, it was unethical not to investigate. She warned the paper’s implications “could interfere with a very important public-health opportunity.” We need the data, you can’t get the data, and please stop talking about this.
John Burn, Professor of Clinical Genetics at Newcastle (later knighted for services to medicine), and Nicholas Fisk, Professor of Obstetrics at Imperial College London, tried a different approach.[10] They broke the composite fetal death finding into subcategories – miscarriage alone was p = 0.12, they noted, so not significant. Take a significant result, split it into pieces too small to reach significance individually, and declare the problem solved. All four categories still ran the same way. The composite was still significant. But by 1997 nobody wanted to hear it.
Czeizel himself, in a 1998 review, reported the total fetal death difference as significant (P = 0.03) and acknowledged Hook’s hypothesis – while noting it was “not accepted by other experts.”[11]
No new data was ever presented. Nobody did the pathological studies. The hypothesis was named, published in the Lancet, co-authored by the trial’s own principal investigator – and then dropped. Twenty-seven years later, it remains untested.
4. Double standard
The Hungarian trial was a randomised controlled trial. Randomisation is specifically designed to ensure that the intervention and control groups are comparable so that differences in outcomes can reasonably be attributed to the intervention.
When the trial showed fewer neural tube defects in the folic acid arm, that difference was widely accepted as evidence of causation.
However, the same trial also reported a statistically significant excess of fetal losses in the intervention arm. At that point the logic changed. Instead of attributing the difference to the intervention, the excess losses were treated as coincidence or background variation.
This is a methodological contradiction. Randomisation cannot be treated as valid evidence of causation for beneficial outcomes while simultaneously being ignored for adverse outcomes observed in the same trial.
Either the trial design allows causal inference, or it does not. If randomisation justifies the claim that folic acid prevented neural tube defects, then the same randomisation must also be taken seriously when it reveals an imbalance in fetal losses.m
5. Continuing harm
The trial also found a statistically significant 41% increase in multiple births, which carry a higher rate of almost every pregnancy complication. There was no follow up of the mothers.[12],[13] This increase that persisted after excluding women who had taken fertility drugs. Czeizel himself dismissed his own finding: “this result, despite its statistical significance, may be due to chance,” he wrote, because multiple births were not a pre-specified outcome.[14] The multiple births – and the seventy dead babies – were both waved away. Follow-up of the cohort of children in the randomised trial found significantly increased atopic dermatitis[15] in infancy and otitis media at age six.[16] Deaths were numerically higher in the treatment group at every single follow-up time point – although the numbers were too small for statistical significance.
None of these harms have been acknowledged by public health officials.
6. The Other Trials
The four earlier trials tested high-dose folic acid (4 mg/day – ten times the supplement dose) in women who had already had an NTD-affected pregnancy. They did find reduced recurrence. But over 95% of NTDs occur in women with no prior history. These were the wrong women, at the wrong dose, answering the wrong question.
And they were far too small to detect the two-percentage-point rise in fetal deaths the Hungarian trial found. Absence of a signal in an underpowered study cannot be used as reassurance of safety. It is simply an absence of data.
7. What Happened After Fortification?
From 1979 to 1997, US infant mortalitydeclined in a predictable way. After mandatory fortification in 1998, the decline flattened.
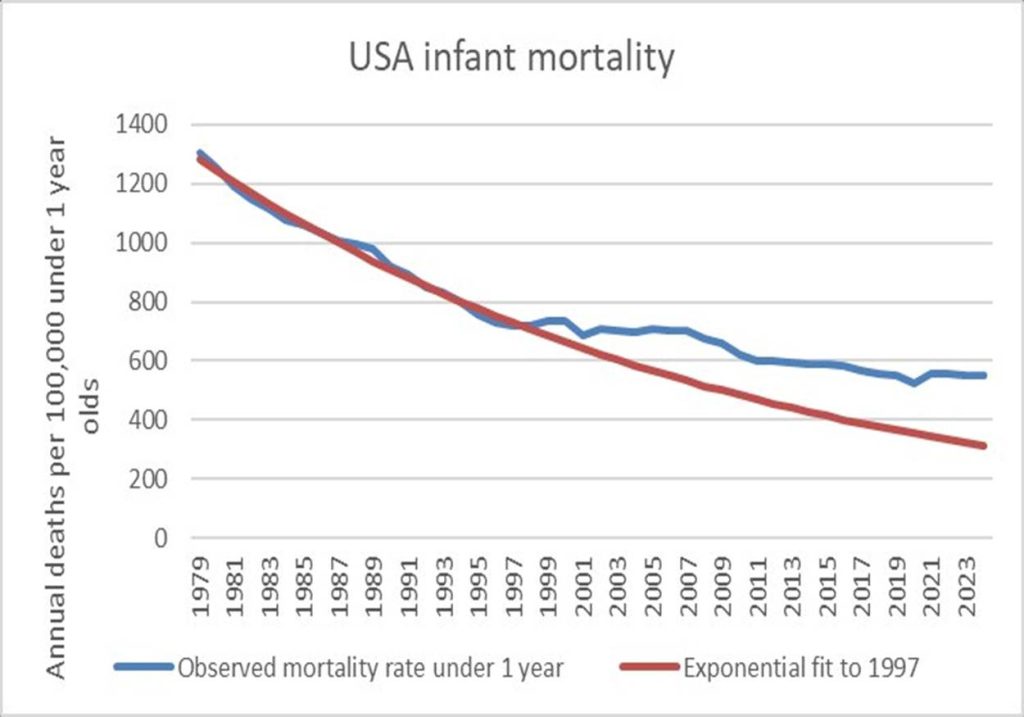
Figure 3: US infant mortality with exponential trend fitted to 1979–1997
Miscarriage rates have climbed from 11% in 1990 to approximately 17% by 2010, a period that coincided with the introduction of mandatory flour fortification and increasing uptake of folic acid pregnancy supplements.[17] The trend persisted after adjustment for maternal age and other demographic factors. The most commonly proposed explanation – that improved home pregnancy testing led to earlier detection of losses that would previously have gone unrecognised – was directly tested in 2017 and no change in gestational age at pregnancy awareness was found from 1990–2012.[18] The link to folic acid has not been investigated.
The Hungarian trial’s excess deaths were overwhelmingly first-trimester miscarriages and chemical pregnancies. The US surveillance system only records fetal deaths at twenty weeks or later.[19] The specific harm signal from the trial – the very deaths that make the number nine – is virtually invisible to the monitoring system.
The monitoring systems simply were not in place to detect the safety signal that the trial shows.
Of course other factors may be at play but the striking feature is that these patterns have not been systematically examined in relation to folic acid exposure, despite the known safety signal in the trial.
Conclusion
Public health messaging has been simply that synthetic folic acid prevents neural tube defects.
It does not mention seventy excess fetal deaths.
It does not mention the Lancet paper where the trial’s own investigator asked whether folic acid works by killing malformed babies.
It does not mention that European data show no fall in total NTD prevalence.
It does not mention that the US monitoring system is blind to the category of death the trial identified.
Nine dead babies for every claimed NTD prevented.
There has also been no mention of the other significant harm caused, measured, reported and never followed up.
A drug with this profile would never be licensed. Calling it vitamin B9 (the synthetic version is not benign) does not change the arithmetic.
The UK is blindly following the USA
From December 2026, synthetic folic acid will be mandatory in all non-wholemeal wheat flour in the United Kingdom, including imports.[20],[21] It will be in bread, pasta, pizza, biscuits, cakes, pies, sauces – bought or home made. Most UK millers have already made the change – including it even in wholemeal and gluten free products.
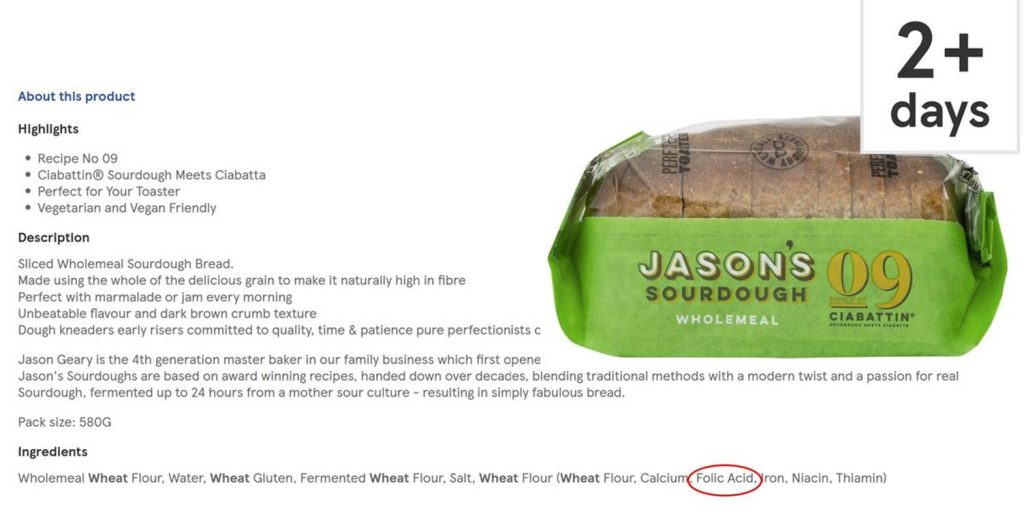
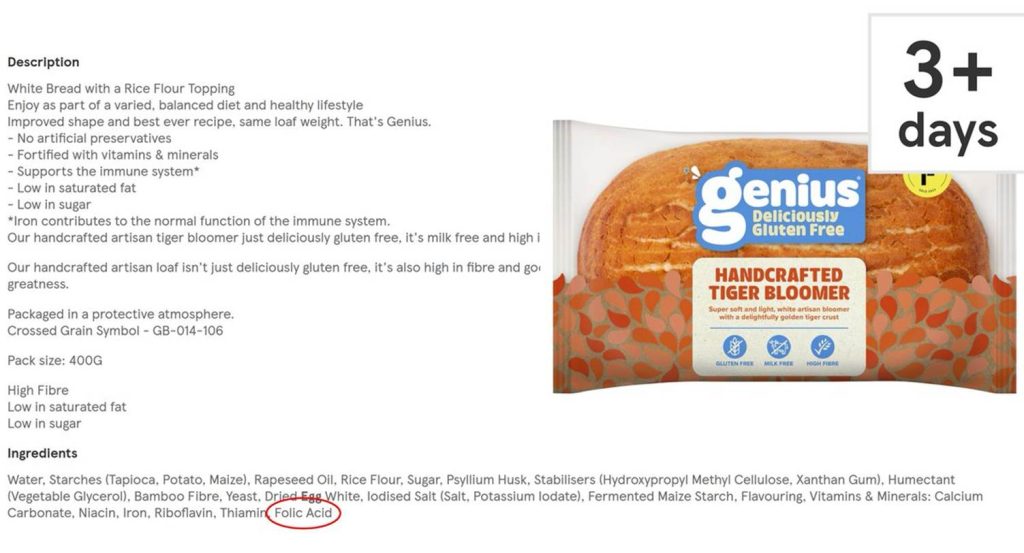
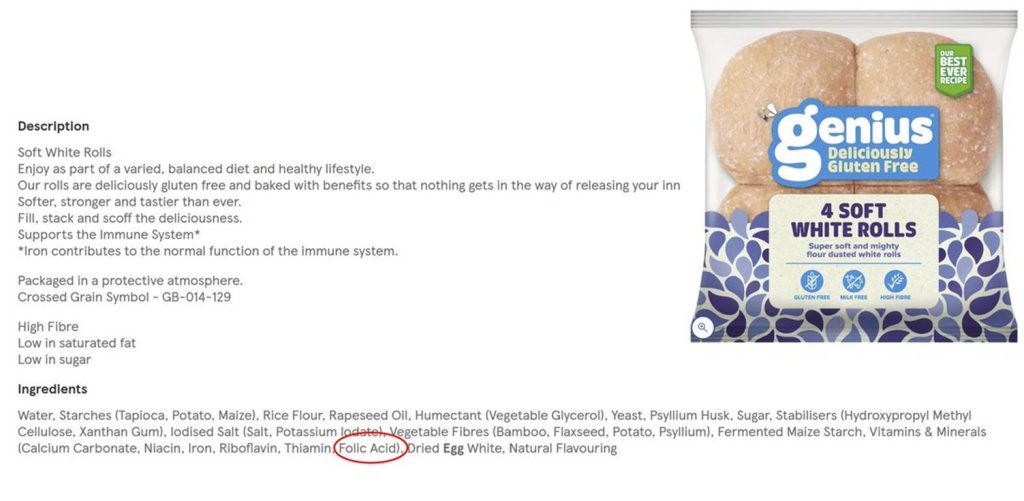
Figure 4: Evidence of folic acid being added to UK wholemeal and gluten free bread in 2025
38% of consultation respondents supported no mandatory fortification at all, and only 9% supported the option actually chosen.[22] It went ahead anyway. The policy is based on the same evidence examined in this article. The same evidence that shows nine dead babies for every NTD prevented.
Statistical note:
Total fetal deaths including chemical pregnancies (374/2,793 vs 304/2,660): two-sided Pearson χ² = 4.92, p = 0.027.
Recognised losses excluding chemical pregnancies (319/2,793 vs 264/2,660): two-sided Pearson χ² = 3.20, p = 0.074.
References
[1] CDC. (2015). Updated estimates of neural tube defects prevented by mandatory folic acid fortification – United States, 1995–2011. MMWR Morbidity and Mortality Weekly Report, 64(1), 1–5. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6401a2.htm
[2] EUROCAT. (n.d.). Prevalence tables. European Surveillance of Congenital Anomalies. https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence
[3] EUROCAT. (n.d.). Prevalence tables. European Surveillance of Congenital Anomalies. https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence
[4] Czeizel, A. E., & Dudás, I. (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. New England Journal of Medicine, 327(26), 1832–1835. https://pubmed.ncbi.nlm.nih.gov/1307234/
[5] ATSDR. (2012). Toxicological profile for manganese. U.S. Agency for Toxic Substances and Disease Registry. https://www.atsdr.cdc.gov/toxprofiles/tp151.pdf
[6] Czeizel, A. E., Dudás, I., & Métneki, J. (1994). Pregnancy outcomes in a randomised controlled trial of periconceptional multivitamin supplementation: Final report. Archives of Gynecology and Obstetrics, 255(3), 131–139. https://pubmed.ncbi.nlm.nih.gov/7979565/
[7] Czeizel, A. E., Dudás, I., & Métneki, J. (1994). Pregnancy outcomes in a randomised controlled trial of periconceptional multivitamin supplementation: Final report. Archives of Gynecology and Obstetrics, 255(3), 131–139. https://pubmed.ncbi.nlm.nih.gov/7979565/
[8] Hook, E. B., & Czeizel, A. E. (1997). Can terathanasia explain the protective effect of folic-acid supplementation on birth defects? The Lancet, 350(9076), 513–515. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(97)01342-1/abstract
[9] Hall, J. G. (1997). Terathanasia, folic acid, and birth defects [Correspondence]. The Lancet, 350(9088), 1322. https://www.thelancet.com/action/showPdf?pii=S0140-6736%2805%2962480-4
[10] Burn, J., & Fisk, N. M. (1997). Terathanasia, folic acid, and birth defects [Correspondence]. The Lancet, 350(9088), 1322. https://www.thelancet.com/action/showPdf?pii=S0140-6736%2805%2962480-4
[11] Czeizel, A. E. (1998). Periconceptional folic acid containing multivitamin supplementation. European Journal of Obstetrics & Gynecology and Reproductive Biology, 78(2), 151–161. https://pubmed.ncbi.nlm.nih.gov/9622312/
[12] Czeizel, A. E., Métneki, J., & Dudás, I. (1994). Higher rate of multiple births after periconceptional vitamin supplementation. New England Journal of Medicine, 330(23), 1687–1688. https://www.nejm.org/doi/full/10.1056/NEJM199406093302314
[13] Czeizel, A. E., Dudás, I., & Métneki, J. (1994). Pregnancy outcomes in a randomised controlled trial of periconceptional multivitamin supplementation: Final report. Archives of Gynecology and Obstetrics, 255(3), 131–139. https://pubmed.ncbi.nlm.nih.gov/7979565/
[14] Czeizel, A. E., Métneki, J., & Dudás, I. (1994). Higher rate of multiple births after periconceptional vitamin supplementation. New England Journal of Medicine, 330(23), 1687–1688. https://pubmed.ncbi.nlm.nih.gov/8177283/
[15] Czeizel, A. E., & Dobó, M. (1994). Postnatal somatic and mental development after periconceptional multivitamin supplementation. Archives of Disease in Childhood, 70(3), 229–233. https://pubmed.ncbi.nlm.nih.gov/8135567/
[16] Dobó, M., & Czeizel, A. E. (1998). Long-term somatic and mental development of children after periconceptional multivitamin supplementation. European Journal of Pediatrics, 157(9), 719–723. https://pubmed.ncbi.nlm.nih.gov/9776529/
[17] Rossen, L. M., Ahrens, K. A., & Branum, A. M. (2018). Trends in risk of pregnancy loss among US women, 1990–2011. Paediatric and Perinatal Epidemiology, 32(1), 19–29. https://pmc.ncbi.nlm.nih.gov/articles/PMC5771868/
[18] Branum, A. M., & Ahrens, K. A. (2017). Trends in timing of pregnancy awareness among US women. Maternal and Child Health Journal, 21(4), 715–726. https://pubmed.ncbi.nlm.nih.gov/27449779/
[19] Gregory, E. C. W., Valenzuela, C. P., & Hoyert, D. L. (2024). Fetal mortality: United States, 2022. National Vital Statistics Reports, 73(9), 1–19. https://stacks.cdc.gov/view/cdc/158788
[20] UK Government. (2024). Birth defects prevented by fortifying flour with folic acid. GOV.UK. https://www.gov.uk/government/news/birth-defects-prevented-by-fortifying-flour-with-folic-acid
[21] Food Standards Agency. (n.d.). Folic acid. https://www.food.gov.uk/safety-hygiene/folic-acid
[22] UK Government. (2021). Proposal to add folic acid to flour: consultation response. GOV.UK. https://www.gov.uk/government/consultations/adding-folic-acid-to-flour/outcome/proposal-to-add-folic-acid-to-flour-consultation-response
