
What is the evidence?
All HART articles also on Substack. Please consider a PAID SUBSCRIPTION so we can continue our work. Comments are open so you can join in the conversation.
Covid vaccine harm is myriad and certain individuals have experienced a hugely debilitating syndrome of injury affecting more than one organ system. However, in terms of the sheer numbers affected the cardiovascular system is at the heart of the matter.
The most common cause of cardiac mortality is a heart attack or myocardial infarction – where part of the heart mucscle dies from lack of blood. This happends because of narrowing or blocking of a coronary artery by a thickening of the wall called atherosclerosis. The cause of atherosclerosis remains controversial but there is good evidence that damage to endothelial cells and inflammation play a critical role. After years of thickening, damage to the endothelial cells on the surface can result in clotting that causes the artery to suddenly become blocked.
There is strong evidence that the covid vaccines induce endothelial cell damage, intravascular inflammation and an increased risk of clotting. These are not mere theoretical risks but are supported by emerging evidence that points to mechanisms of harm which have led to the excess mortality.
What is the role of endothelial cells?
The role of endothelial cells as guardians against coagulation is well-established. Damage to these cells, as has been observed following vaccination, can contribute to the development of atherosclerosis. Furthermore, endothelial damage can precipitate the formation of thrombi (structured clots).
What does the vaccine do to endothelial cells?
Notably, mRNA vaccines have been linked to an increase in inflammatory markers affecting endothelial cells in the short term, raising the spectre of cardiovascular disease. Spike protein induces endothelial inflammation and scientists have demonstrated how “endothelial damage is a central part of SARS-CoV2 pathology and may be induced by the spike protein alone.” The vaccine has also been found to increase permeability in the endothelium of the heart’s vessels. Not only are endothelial cells affected by any spike protein in the circulating blood but they themselves can become spike factories. A skin biopsy taken 3 months after the vaccine showed mRNA induced spike protein inside endothelial cells.
Compelling evidence of the vaccine’s impact on the vasculature comes from the increased risk of retinal vessel occlusion, a condition that can lead to blindness and serves as a marker for small vessel damage. This risk, significantly elevated in the months following vaccination, underscores the systemic nature of the vaccine’s effects on the vascular system. Moreover, neurological injuries were shown to be ultimately due to immune complex formation in the small vessels supplying the nerves.
How can an injection into muscle damage endothelial cells?
The method of vaccine administration itself may inadvertently contribute to vascular damage as clearly set out by Marc Girardot. Intramuscular injections can become systemic, exposing the entire cardiovascular system to potential harm. Epipens (adrenaline injections) take advantage of this fact in order to save people’s lives from anaphylaxis.
Accidental intravenous administration of intramuscular injections happens around 1.5% to 2% of the time even when nurses carefully aspirate first to check for blood. Bodybuilders who inject steroids intramuscularly report systemic distribution resulting in “tren cough” and an oily or spicy taste occurring in around 2% of injections. Similarly a proportion of people with adverse reactions after covid vaccines reported a metallic taste immediately afterwards. How could this have occurred without intravascular dissemination?
Intramuscular injection results in a pool of extracellular fluid which would be cleared by venules and lymphatic vessles. This would expose a disproportionate quantity of the drug to the endothelial cells of the vascular system. However, accidental intravascular injection would have a more extreme effect.
Lipid nanoparticles which enter a cell will deliver their mRNA which leads to foreign spike production and destruction of those cells by the immune system. That is the design of the mRNA platform and the end result, after cell destruction is development of an immune memory. Any endothelial cells that are destroyed in this way could trigger clotting in that area or else could begin or accelerate atherosclerosis.
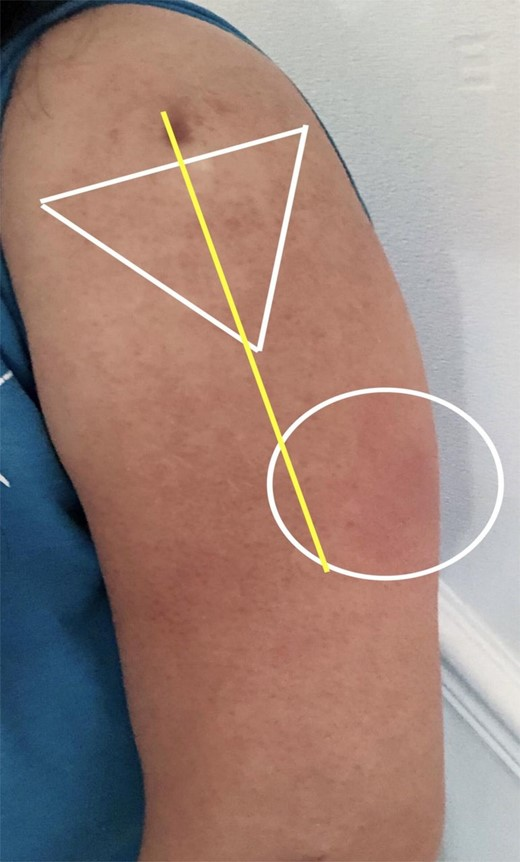
Injections were often given by volunteers and many were not given within the small safe triangle that reduces the risk of intravascular injections. The risk of intravascular injection is therefore likely even higher than reported in historical studies where the injectors were trained.
What is the evidence of vaccine induced atherosclerosis?
The key concern regarding risk of atherosclerosis comes from the big picture epidemiological data in the next section. However there is also some specific evidence of inflammation of the vasculature after covid injection.
Several case reports have documented vaccine inflammation of the vessels of the heart. Inflammation of heart vessels is a risk factor for both clotting in these vessels and for the development of atherosclerosis.
- 55 year old who died 4 months after mRNA with a lymphocytic myocarditis and a lymphocytic vasculitis of the small vessels supplying the coronary arteries leading to thrombosis. Vaccine derived spike protein was expressed by the endothelial cells lining the vessels.
- 76 year old myocarditis small vessels of the heart showed inflammation and endothelial cell swelling and death with occasional clots on the endothelial surface.
- 39 year old man with inflammation localised around coronary arteries.
- 24 year old with myocarditis after Moderna showed inflammation focused around the blood vessels of the heart.
- Two teenage boys with severe inflammation of the heart suggestive of catecholamine-induced injury.
In a study involving over 500 middle-aged patients who were regularly monitored, a predictive scoring model using inflammatory markers linked with heart attack risk indicated that the mRNA vaccine potentially elevated the likelihood of a coronary event within five years from a pre-vaccine rate of 11% to 25% within 2–10 weeks following mRNA vaccination. A notable early critique of this study’s conclusions pointed out the absence of a control group. Despite this, if the results hold any degree of accuracy, it suggests a significant increase in the progression of coronary artery disease and, more critically, the risk of heart attacks, occurring in the months after receiving the vaccine.
HART sent an open letter to the British Heart Foundation and Charity Commission in January 2023 to ask them to investigate but, despite chasing, have had no response from the British Heart Foundation. The Charity Commission decided not to investigate.
What is the epidemiological evidence of damage from vaccines?
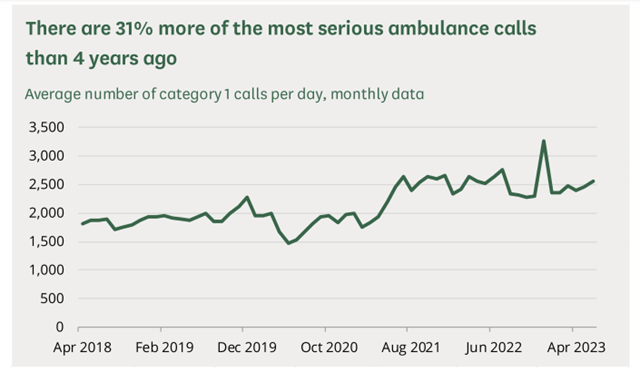
Calls to ambulances for life threatening conditions were stable at 2000 per day with a decrease during lockdown. However, during the vaccine rollout they rose and have remained at 2,500 per day since.
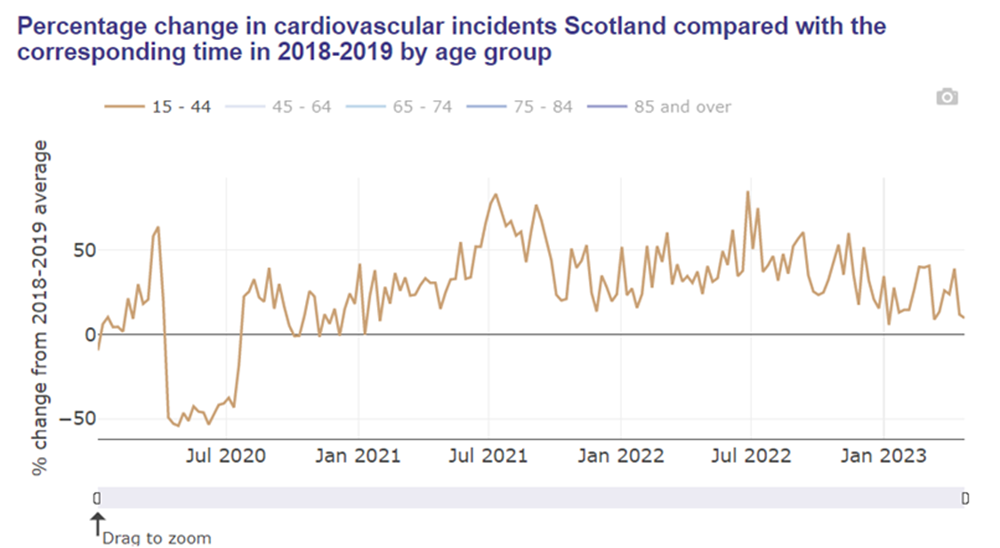
HART has written extensively on the nature of these excess deaths which are predominantly cardiovascular deaths which have had a large impact on young people. They are not due to a reduction in prescriptions as Chris Whitty claimed as there has been no reduction. It is easiest to show an increase in younger populations where background rates are lower. Cardiovascular emergencies rose in line with vaccination in Israel and Scotland.
Covid is not the cause of the excess. Studies claiming covid leads to heart disease almost always include spring 2020 positive covid cases. These cases are biased as testing was not readily available. People with a high likelihood of heart disease e.g. the hospitalised, were much more likely to be tested than people who were otherwise healthy. Comparing this group to the population as a whole is not reasonable. Comparing the risk of a myocardial infarction to people who had just had another cause of pneumonia showed the “risk of AMI after hospital discharge was lower compared to that observed after other inflammatory conditions of the respiratory tract, such as pneumonia.”
Furthermore, many studies fail to account for a low incidence of disease in the period immediately after vaccination the “healthy vaccinee effect” and include this when comparing overall risk. Finally, socioeconomic factors are significantly worse in the unvaccinated population putting them at a higher baseline risk and yet studies fail to account for these when assessing vaccine safety.
In order to understand whether vaccines could have caused this rise it is helpful to look at places that had had minimal covid before their national vaccine roll-out. Countries like Australia and Singapore can act as a control group in this regard as the timing of their covid waves was very different but the timing of their vaccine rollout was similar. Both show a rise in cardiac presentations and mortality in line with the vaccine rollout.
How important is an increased risk of clotting?
Increased clotting risk, another grave concern, has been evidenced by studies showing vaccine-induced platelet activation and aggregation. This heightened pro-thrombotic state following vaccination raises the alarm about the potential for life-threatening conditions.
The covid spike protein has been shown to activate platelets. The receptor binding domain of the spike protein included in the vaccine “could bind platelets, cause platelet activation, and potentiate platelet aggregation” in mice. Another study on mice also showed spike receptor binding domain activated platelets through direct binding.
The mRNA covid vaccines deliver a sequence for cells to produce the whole viral spike protein. The only differences are two proline amino acids at the base of the protein were substituted and the mRNA was synthetic enabling it to last much longer than normal RNA. The substitutions were to prevent binding of the spike protein to the ACE-2 receptor on the cell surface. However, not all spike pathology is dependent on this binding and cell entry occurred anyway as a function of the lipid nanoparticle delivery system.
There are examples of the impact of this effect in the real world. Plasma from a 25 year old woman injected with the Moderna product showed dose dependent platelet activation. The more spike protein present the more platelet activation occurred. She did not have anti-platelet factor 4 antibodies which cause the AstraZeneca related VITT and brain clots.
Four people given Moderna showed low circulating platelet levels at day 3 (arguably due to thrombus formation) which recovered by day 7. They went on to show that platelets themselves were producing spike proteins up to 40 days after vaccination.
Spike protein was found to circulate in the plasma of Moderna recipients from one day after vaccination. “Spike protein was detectable in 3 of 13 participants an average of 15 days after the first injection.”
It has been proposed that the increased inflammatory state after mRNA vaccination is responsible for an enhanced propensity to form thrombus in the absence of thrombocytopenia. Fibrinogen forms clots in the laboratory when spike protein is added to plasma even in the absence of platelets. The clots formed were protein rich and could not be degraded like usual clots. There was a marked rise in pulmonary embolism in 2021 in Israel with vaccine rollout not evident in 2020 with the virus alone. This increased risk continued into 2022.
How long did the increased risk last?
Pfizer claimed the mRNA would be “nearly completely degraded in 9 days” and claimed the spike protein would be broken down as if it was a regular human protein. However, human studies published more than a year after the vaccine rollout began showed mRNA or spike protein was detectable for considerably longer periods. In many of these studies it was still present at the last time point it was measured.
- mRNA 15 days in the blood
- mRNA up to 28 days in bloodstream
- both mRNA and spike proteins were detectable in lymph nodes for up to 8 weeks
- 150 billion spike proteins circulating in the blood of 3 out of 13 participants at two weeks.
- spike protein circulating in the blood for 4 months.
- spike protein from vaccination demonstrated in a shingles skin biopsy at 3 months
In 2023 it was demonstrated that half of the vaccinated population were still producing vaccine induced spike protein from 69 days to up to 6 months after injection when the study ended. It is highly unlikely for even modified RNA to remain active for such a length of time and the authors proposed either that it was integrated into the cell’s DNA or that of bacteria in the gut which became a continuing source of spike protein production.
The dishonest marketing of these products as “safe and effective” has led to the dishonest failure to face up to their terrible safety profile. With the prime minister this week calling the vaccines “safe” in parliament it feels like we are no further forward. However, the evidence is comprehensive and more and more keeps accumulating. Ultimately there will be nowhere to hide.
