

A letter explaining the situation you find yourself in
A letter from Dr Clare Craig, 3rd November 2024
On 1st November, a Professor of Social Science placed this heart-felt post on Twitter:
“I’m feeling broken today. My mum has long covid; likely from a recent asymptomatic infection: microclots, severe pain, breathlessness and lethargy. She’s always been careful and listened to me, she’s fully boosted, she masks indoors etc. I’ve not been able to protect her from this.”
Reply: “How did you find out she had microclots?”
Professor: “Went to A&E with chest pains… pulmonary embolism. Medics there later told her, following whatever tests they did, that she had 100s of tiny clots in her lungs. They said they were baffled and had never seen anything like this (which makes me feel baffled!).“
For most of members of HART and our readers, it is hard to comprehend the gulf between what we are seeing and reading and how others are interpreting the world around them. Clare Craig, sat down to write a long letter, to explain just some of the enormity of the evidence around covid-19 and the vaccines. It is long, much longer than our usual articles, but we wished to publish it in full here and hope others may find it helpful.
Dear Professor,
Yesterday, someone shared your Twitter post with me. I have also read some of the responses to it. I imagine yesterday was a very difficult day for you, especially given the concerns for your mother.
I find it hard to imagine what it must be like to spend four years deep in one belief system and then suddenly, and horribly, have your eyes open to the fact that you may have been deceived.
I will take you through the scientific evidence for why what happened to your mother was related to her covid vaccines and not to “asymptomatic covid”. You said you only want peer reviewed evidence so you can check funding sources etc. Let me reassure you that funding concerns are all in one direction through pharma sponsorship (see editors of NEJM and Lancet) and no money comes to those who are raising concerns. You might have been misled by the claim that “Anti-vaxx groups spend nearly $1 billion on social media.” you only have to read as far as the sub-heading to see this was based on a claim they had “found that anti-vaxx groups reach 58 million users on social media, earning the platforms roughly $1B in revenue.” There is no money in being anti-Big-Pharma. Whose influence do you fear? The credentialled people who have raised concerns about these products have been subject to censorship, smearing and witch hunts. There has been nothing to gain for them.
Those of us who have been trying to communicate these risks, unpaid and under constant attack, have seen the word “baffled” used repeatedly by professionals who should know better. It has come to epitomise the attitude of avoiding understanding because of the painful cognitive dissonance that comes with that. If you are prepared to set aside that pain and do some work, I am going to set it all out for you here – fully evidenced. Take it a bit at a time and absorb what you can in steps – it will still be here for you later.
All I ask that you approach this with an open mind and if your mind changes that you do not pretend otherwise. Do not become cowardly and hide, pretending you remain ignorant, but use your credentials and your voice to awaken other people to the truth.
The vaccines have been worshipped as false idols. Those who have criticised them have been treated as blasphemers and those injured by them as apostates. They are not holy, they are just a drug. Leave aside your emotions about covid and vaccines and try and engage your rational brain to weigh up the evidence below.
Yours sincerely,
Dr Clare Craig BM BCh FRCPath
1. Asymptomatic covid (as opposed to presymptomatic) cannot cause pathology
Diseases are based on symptoms. Some diseases have an asymptomatic period before symptoms. No diseaseas are asymptomatic. It would be a contradiction. Asymptomatic infection, as opposed to presymptomatic infection, means a positive test in someone who never develops symptoms. The test is highly sensitive and able to detect only 3-4 virus particles which could be found in a single aerosol 5 thousandths of a millimetre in diameter. People breathe in single contaminated aerosols all the time. Finding such contamination on a swab in someone who never develops symptoms means either: the sample was contaminated in the hospital air or laboratory, there was virus in the airway but it never entered a cell or there was virus in the airway but the immune system killed it when it entered a cell. In none of these circumstances would there be a possibility of serious pathology resulting.
2. The vaccines contain the whole spike sequence
Many professionals have assumed that the vaccines contain only peptide sequences as that would be the right approach to make them safe. That is not what happened. The AstraZeneca vaccine contained the whole unadulterated 1273 amino acid sequence for spike. Pfizer and Moderna switched out two proline groups in an attempt to reduce the shape change that comes with the cleavage (at the furin cleavage site) that allows cell entry. That may have reduced cell entry via ACE-2 receptors but spike can also enter cells via other receptors e.g. CD147, LDLRAD3 TMEM30A, (which might be reduced by the two proline substitution), DC-SIGN, L-SIGN(which would be unaffected). Futhermore, part of the SARS-1 spike is exactly the same shape as the missing gp41 protein which allows viruses to enter T cells. By 2022, a team based at the Wuhan institute of Virology, claimed that SARS-CoV-2can enter T helper cells without using the ACE-2 receptor and kill them, suggesting this additional route of entry is clinically meaningful. This work was replicated by a Brazilianteam in 2023. There is also potential for cell entry simply because the receptor binding domain is highly charged (unnaturally so). Even without any of those ways of entering and interacting with cells the spike was made inside cells in the first place thanks to the vaccine delivery systems.
The pathology that you have been so concerned about regarding the spike on the virus can result from these vaccines (and more besides).
3. These “vaccines” used novel technology
“Vaccine” is a very powerful word. We are told they are “modern medical miracles” and they are almost synonymous with “safe and effective”.They are drugs like any other and should be treated on merit not as sacred cows.
a) Lipid nanoparticles
The mRNA drugs used lipid nanoparticles which were first designed as a drug delivery system in the 1990s. The first gene therapy to use RNA delivered in lipid nanoparticles was approved by the FDA in 2018. Lipid nanoparticles were specifically designed, for conventional gene therapy, to reach every part of the body and to enter the nucleus of a cell. These people need a working gene to be delivered to cells throughout their body and lipid nanoparticles were therefore optimised to be able to reach every organ. However, the pharmaceutical companies found that repeated dosing led to problems with toxicity. Because of this Novartis, Merck and Roche abandoned the platform. Katalin Karikó, vice president at BioNTech said, “I would say that mRNA is better suited for diseases where treatment for short duration is sufficiently curative, so the toxicities caused by delivery materials are less likely to occur.” Moderna and BioNTech decided to focus their technology on vaccines instead – because, they claimed, with vaccines repeated dosing is not necessary and the toxicity issues can be avoided. The irony of this is not difficult to see.
The first approved vaccines using this system were the covid vaccines. The CEO of Pfizer commented that “mRNA was a technology that had never delivered a single product until that day.” Before the covid vaccine trial there were 285 people who had been administered mRNA vaccines, all in the last few years and all in a clinical trial setting. Severe adverse events, which are reactions that cause hospitalisation, disability or are life threatening occurred in between oneand twelve percent in these small trials. The primary safety concerns regard liver toxicity and inflammatory and immune reactions but these types of lipid nanoparticles can also cause direct cell death in a laboratory setting. Charged LNPs can make the energy generating centres of the cell, the mitochondria, leaky. The consequence could be cell death but where the cell survived it would struggle to produce the energy needed for normal cell function. In fact, one of Pfizer’s lipid ingredients ALC-0159, did not comply with European quality standards and MHRA did not disclose the way they had assessed its safety. The covid vaccine trials did not include a group given only LNPs so the extent of toxicity remains poorly measured.
The damage inside the cell from LNPs is of little importance if it is destined to die. However, not all LNPs contain mRNA and so not all affected cells will die. A study by McGill University and Moderan was set up in 2023 to “verify how many LNPs carry a payload such as mRNAs for vaccines.” Around 9,000 different proteins are produced in increased amounts in response to LNPs. The effect is complex but highly inflammatory with numerous neutrophils coming to the injection site – effectively internal pus. In contrast only 2,000 genes are upregulated in symptomatic covid. The quantity of LNPs in a single human dose of Moderna given intranasally is enough to kill 154 mice within 24 hours. For comparison, the dose of inhaled plutonium needed to cause the same level of death, over a 30 day period rather than 24 hours, would have to be four times as high. In Moderna’s biodistribution study submitted to the FDA they admit that the toxicity problems “are driven primarily by the composition of the LNPs and, to a lesser extent, by the biologic activity of the antigen(s) encoded by the mRNA.”
b) Modified RNA
The mRNA products were gene therapies. The official definition is broad and includes treatments that use genetic messaging i.e. RNA. The UK’s Health Research Authority’s definition of gene therapy, is “a product… aimed at the transfer of a prophylactic, diagnostic or therapeutic gene (i.e. a piece of nucleic acid).” BioNTech, the company that partnered with Pfizer to make the Pfizer product, published a paragraph about mRNA technology classification in their 2019 filing to the US Securities and exchange commission. In it they said, “mRNA therapies have been classified as gene therapy medicinal products.” Moderna, in a similar filing, said, “mRNA has been characterised as a Gene Therapy Medicinal Product… the association of our investigational medicines with gene therapies could result in increased regulatory burdens, impair the reputation of our investigational medicines, or negatively impact our platform or our business.” Their concern regarding their business model was not misplaced, given that the US FDArequires five to fifteen years of long term follow up for gene therapy products before approval.
The FDA’s definition includes both transferred genetic material including RNA or products that act by “specifically altering host (human) genetic sequences.” The mRNA products fit the first of those two alternative definitions. By the FDA definition the Oxford-AstraZeneca and Johnson and Johnson products are also gene therapy as they use a genetically modified virus vector to insert DNA into the cell nucleus to make the cell machinery produce spike protein. The Australian gene technology regulator granted AstraZeneca a licence for “Commercial supply of a genetically modified COVID-19 vaccine” in February 2021.
4. Spike in blood from virus compared to vaccine
One way or another the end result of any viral infection is cell sacrifice. The pessimists like to forget that in the vast majority of cases, the immune system handles exposure to the virus. Where symptoms do develop the immune system efficiently confines the virus to the airways. For SARS-CoV-2 the vast majority of cells sacrificed are mucosal cells lining the respiratory tract. These have a high turnover and will be rapidly replaced as with all cells with a role as a protective barrier. Positive PCR from blood is often a result of circulating viral RNA rather than circulating intact virus capable of infecting other cells. Fauci and colleagues call this“RNAemia” (circulation of viral RNA in the bloodstream, as is seen with most mucosal respiratory virus infections, as distinct from viremia, in which infectious viruses can be cultured from the blood).” Except in the very sick, viruses remain restricted to the respiratory lining during an infection.
In contrast the vaccine spike is systemic from the outset. Although people were told it would remain in the arm that could never have been true. One group of researchers concluded “mRNA translation in muscle cells does not seem to play a major role in the induction of protective immune responses against SARS-CoV-2.” The liquid will mostly end up in the space between cells. It will be at high pressure as it’s not supposed to be there. As with all extracellular fluid it will mostly end up in venous capillaries. A small proportion will end up as lymph, draining through lymphatic vessels, via the lymph nodes. Lipids, including lipid nanoparticles, are preferentially taken up by the lymphatic system. The lymph is dumped back into the venous blood right by the heart. Whether it ends up in venous blood or lymph, the next stop will be the right side of the heart followed by the lungs, the left heart and then out to the body. This is how Epipens work. Epipens are given into muscle to quickly get adrenaline throughout the body to treat anaphylaxis. This shows just how ridiculous the claim that an injection into muscle will stay in the muscle. The manufacturers and regulators knew or ought to have known that the claims being made in this regard were impossible. At the very least, they ought to have identified it as a reason for further study. Instead, when Moderna showed that injecting rats intravenously with the lipid nanoparticles resulted in bone marrow toxicity, the excuse there would be minimal risk in humans because the injection was into the muscle seemed to be fully accepted. Pfizer-BioNTech clinical trial documents revealed that LNPs travelled to many organs in ratbiodistribution studies. Measurement stopped after 48 hours despite signs of an increasing rate of accumulation in the ovaries, liver, adrenal gland and spleen.
5. How much spike is produced?
No one knows how much spike protein is produced or how it varies based on sec and age etc. Even now, despite the WHO calling for animal studies to answer those questions in December 2020.
Even if each lipid nanoparticle contained only 10 strands of mRNA and even if each of those were only made into 100 spike proteins by the cells they entered, then there would still be 30 trillion spike proteins made as a result of the injection. This is of the same order as the upper end estimate for the number of spikes produced at peak infection with about 40 on each virus particle. In an infection the spike is largely confined to the lining of the airways from where it is expelled from the body. No-one can tell you how many cells end up producing spike after vaccination and how many are therefore sacrificed because no-one has tried to measure it. No-one can tell you which organs they are in either. In December 2021, the MHRA admitted it did not know how many lipid nanoparticles were in a dose, a crucial first question in order to calculate the number of cells sacrificed.
The Moderna product delivered 40 trillion molecules of mRNA – more than one for every single cell in the body. For Pfizer it was 14 trillion, so more like one for every two cells. Each was delivered in 50-100 billion lipid nanoparticle bubbles making roughly 1000 mRNA molecules per LNP for Moderna and 300 for Pfizer.
Although the MHRA claimed in September 2021 that the number of lipid nanoparticles in a dose is part of their “acceptance criteria,” by December they said they did not actually know “because this information is not deemed crucial to the safety of the Moderna vaccine.”
The amount of spike present in the blood in the first two days was of the same order as in an infection. Two weeks after injection there were still 150 billion spike proteins circulating in the blood of 3 out of 13 participants. That’s 1.5 million for each drop of blood.
People have claimed pseudouridine which makes up only 0.2-0.6 percent of human RNA was used. It was not. The nucleotide used was N1-methyl-pseudouridine which is not natural. Studies on this type of RNA only began in 2015. Having deliberately set out to make the RNA last as long as possible, understanding how long was critical. No-one knows how long it lasts in the body. How is it removed? It is the most fundamental of drug safety questions. What happens to it afterwards? Would it be recycled by cells, extending the time other normal RNA lasted? Are the answers different for younger people where protein production might be more efficient? The regulators have still not secured an answer to these questions in 2024.
After one month mRNA was detectable in the blood. In one patient mRNA was found in the muscle of the opposite arm after one month. One study showed mRNA and protein in lymph nodes at the last point they measured 2 months after vaccination. A 64 year old man had spike protein from vaccination demonstrated in his shingles skin biopsy (inside endothelial cells), 3 months after their last dose. Spike was found circulating in exosomes after 4 months in eight out of eight adults.
6. Does vaccine spike cause micro-clots?
Spike protein induces endothelial inflammation and scientists have demonstrated how “endothelial damage is a central part of SARS-CoV2 pathology and may be induced by the spike protein alone.” mRNA vaccines increase inflammatory markers which affect the endothelial cells in the short term. It is easiest to see small vessel damage by looking at the retina. A study in Taiwan showed an increased risk for all age groups of retinal vessel occlusion which can cause blindness. The risk after 12 weeks was three times as high as background rates. After two years the risk was double with an additional case for every 300 vaccinated over 65 years olds and 1000 18-64 year olds.
The covid spike protein has been shown to activate platelets. The receptor binding domain of the spike protein included in the vaccine “could bind platelets, cause platelet activation, and potentiate platelet aggregation” in mice. Another mouse study also showed spike receptor binding domain activated platelets through direct binding. Plasma from a 25 year old woman injected with the Moderna product showed dose dependent platelet activation. The more spike protein present the more platelet activation occurred. She did not have anti-platelet factor 4 antibodies. Four people given Moderna showed low circulating platelet levels at day 3 (arguably due to thrombus formation) which recovered by day 7. They went on to show that platelets themselves were producing spike proteins up to 40 days after vaccination.
Microthrombi formation after mRNA vaccination was serious enough to lead to pulmonary hypertension that was treatable with anticoagulation. It has been proposed that the increased inflammatory state after mRNA vaccination is responsible for an enhanced propensity to form thrombus in the absence of thrombocytopenia. Three patients presented at days 2-3 after Modernawith clots, despite no predisposition to clotting. Fibrinogen forms clots in the laboratory when spike protein is added to plasma even in the absence of platelets. The clots formed were protein rich and could not be degraded like usual clots.
Pulmonary emboli are common and in populations with a large elderly population an increase from vaccines may not be statistically significant because of the high background rate. However, in a younger population, like Israel, changes would be more noticeable. There was a marked rise in pulmonary embolism in 2021 in Israel with vaccine rollout not evident in 2020 with the virus alone.
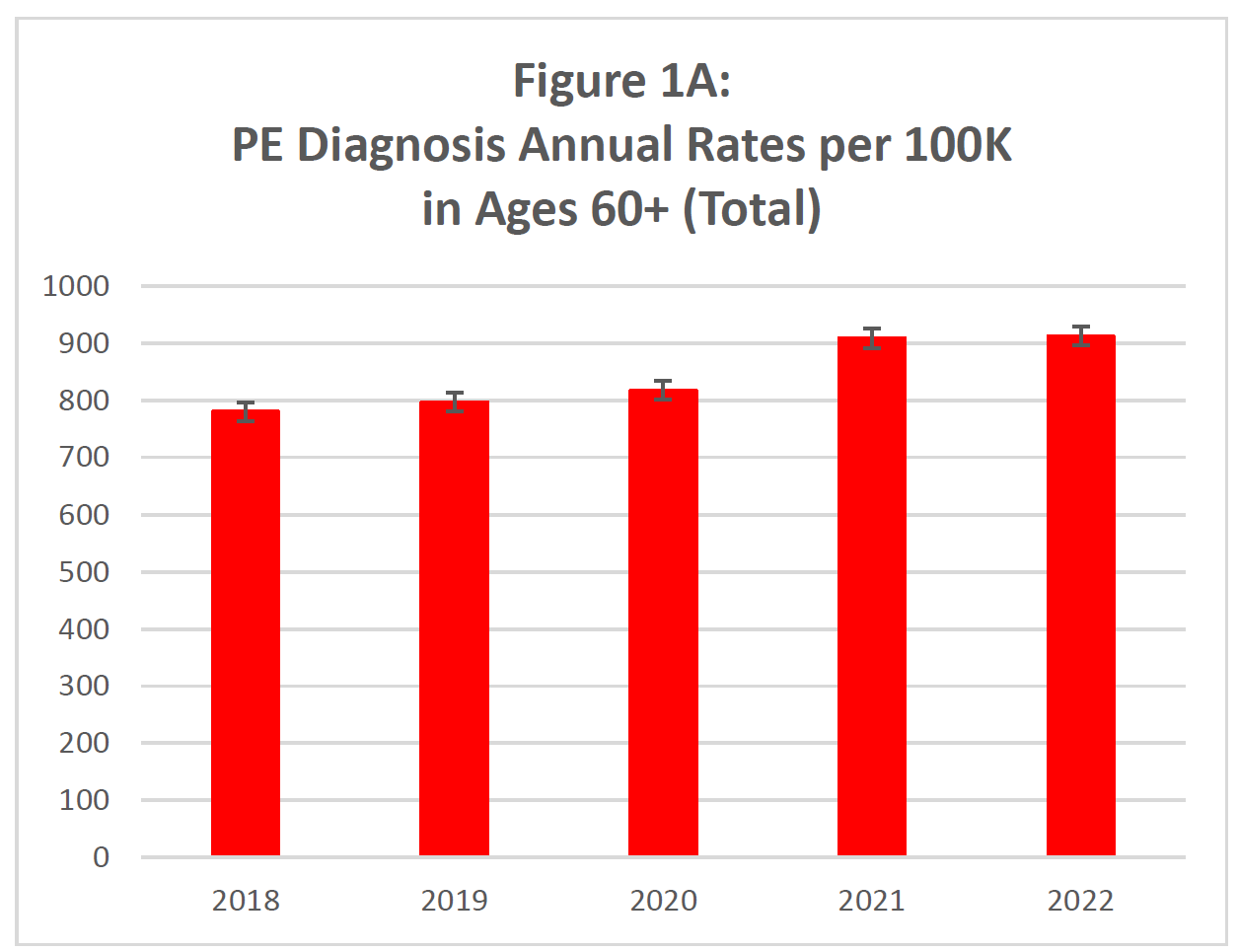
Figure 1: Pulmonary embolisms in Israel per 100,000 people
The FDA conceded that there is an increased risk of pulmonary embolisms in over 65 year olds despite using a very biased methodology.
7. Other mechanisms of vaccine harm
I have focused above on the spike protein but that is a very narrow view of the causes of harm. The other causes are likely to cause a wide breadth of presentations. It is this breadth of presentations that has caused many doctors and the regulators to dismiss the issues as coincidences. Regulatory systems are set up to detect single new rate conditions of increased incidence.
For example, FOIs from FDA show there were 770 conditions where reporting was higher that would be expected compared to unrelated conditions. Of these, 500 had a higher signal than myocarditis.
- Cell damage
The expression of foreign protein leads to T cell mediated cell death. This occurred in organs across the body. All our organs have a cellular reserve which can be hiding all sorts of different pathologies within that organ. Depletion of the cellular reserve will reveal a wide variety of conditions. - Vascular damage
Damage to small vessels will affect every organ. A study spanning six neurologicaldepartments in the USA demonstrated abnormalities were shown in the small vessels supplying the nerves seen in skin biopsies. - Unknown proteins
Multiple proteins of unknown function would be produced because of- Fragmented RNA in the vaccines
- “Frameshifting” where the sequence slips when being read resulting in the production of unintended proteins. Although some have tested for particular unintended proteins the range is huge and what was really produced remains a massive unknown. Antibodies to one possible alternative protein were found in a third of subjects.
- Thirdly, the nucleotides in the sequence were adjusted to maximise production in human cells while keeping the same resulting amino acid sequence. Such manipulations result in unpredictable folding resulting in a new shape and new, unpredictable function.
- Endotoxin
Mass manufacturing used massive vats of E. coli bacteria, commonly found in faeces. E. coli has a harmful substance in its outer layer called endotoxin, which can cause various health problems. Vaccine vials were contaminated with endotoxin. - Foreign Nucleotide
The WHO said, “drugs that contain unnatural nucleoside analogues have caused mitochondrial toxicities, resulting in myopathy, polyneuropathy, lactic acidosis, liver steatosis, pancreatitis, lipodystrophy, and even fatality.”They recommended animal testing to assess this issue. - Autoimmune harm
When the body attacks its own cells resulting in disease, the medical term used in auto-immune disease. The conventional mechanism is that the immune system is misdirected and attacks the cells but the clinical picture would look just the same if the attack was a result of removing cells expressing foreign protein. The more conventional concern of misdirection of the immune system was also valid, especially given the high levels of antibodies that were produced and especially as the spike protein had 80 percent homology with human proteins.
9. These harms were not a surprise
In summer 2020, The Brighton Collaboration established working groups to examine vaccine side effects including, clotting, cardiovascular injury and multisystem inflammatory syndrome in children.
On 22nd October 2020, Steven Anderson who was in charge of drug safety monitoring at the FDA presented a list of 22 “possible adverse events.” The list was determined using three sources: potential concerns raised by pharmaceutical companies; the medical literature and regulatory experience with vaccines and this particular platform. The slide was shown two and a half hours into the meeting and was only visible for one second. The list included demyelinating diseases, seizures, stroke, narcolepsy, allergies, acute myocardial infarction, myocarditis/pericarditis, autoimmune disease, deaths, pregnancy and birth outcomes, clotting issues and thrombocytopenia, arthritis and joint pain, Kawasaki disease, multisystem inflammatory syndrome in children and vaccine enhanced disease. This was far from a scatter gun list and the FDA was showing considerable foresight. The following day the MHRA advertised for AI software “to process the expected high volume of Covid-19 vaccine Adverse Drug Reaction”
An AstraZeneca representative said, “This is a unique situation where we as a company simply cannot take the risk if in … four years the vaccine is showing side effects.” The Pfizer-BioNTech contract said “the long-term effects and efficacy of the Vaccine are not currently known and… there may be adverse effects of the Vaccine that are not currently known.”
Pfizer-BioNTech insisted on blanket immunity, or, as in the UK, unlimited indemnity as part of its contracts with the government. Matt Hancock, the health secretary was gung-ho saying, “I would like to stress that the data so far on this vaccine suggests that there will be no adverse reactions, and so no liability.” The UK government signed up saying, “Willingness to accept appropriate indemnities has helped to secure access to vaccines…sooner than may have been the case otherwise.”
The Pfizer contracts included a ten year secrecy clause but the Albanian, Brazilian and South African contracts ended up published online. At a Brazilian Inquiry into covid in May 2021, the resident and health ministry claimed the terms of the contract had been “abusive”. The CEO of Pfizer Brazil in 2020, Carlos Murillo, said“The conditions that Pfizer sought for Brazil are exactly the same conditions that Pfizer negotiated and signed, at this moment, with more than 110 countries in the world.”
The Indian government would not provide indemnity and told Pfizer that they wanted to run an independent trial of the Pfizer/BioNTech product before agreeing a contract as no Indians had been included in the trials. All other vaccine companies agreed. Rather than cooperate to ensure patient safety, Pfizer walked away from a market containing a sixth of the world’s population.
10. Long covid or long vaccine?
Since 2019 there has been a mass disabling event. The UK had a pretty steady 2 million working aged people who were long term sick from 2012 to 2020. By the end of 2023 there were an extra 800,000. In the USA an extra 3 million have been added to the disabled figures in that time period. In UK and USA the numbers rocketed from May 2021 and stabilised at the end of 2023.

Figure 2: US disability data
How much of this was due to long covid? There are a proportion of people who have prolonged sickness after a covid infection. In previous years, post viral syndromes have similarly caused a longer debilitating illness in a minority. Modern medicine could offer little but hand holding while time did the healing. As well as the post viral syndromes, I was taught to tell pneumonia patients, even young ones, that it would be a full six months before they would feel fully recovered. There was never a label for these “long pneumonia” patients so there are no measurements with which to compare such patients with post covid-labelled pneumonia. These conditions are real and can be horribly debilitating, altering the lives of those affected in dramatic ways. I honestly feel for those affected. However, that does not mean long covid caused the rise in long term sickness. The data on overall sickness shows that post viral illness continued at the same rate as before.
The Governor of the Bank of England(15:23) commented to the parliamentary treasury committee in May 2022on a 450,000 person drop in the labour force including 320,000 with long term sickness. Estimates based on surveys and modelling in March 2022 reached a figure of 80,000for the number of people not working because of long covid. It is not clear how that compares to post viral and post pneumonia syndromes from the past. There is an obvious huge discrepancy between the 320,000 people missing from the workforce and the numbers attributable to long covid.
A team at Imperial College stepped up to solve the problem. They carried out a survey and claimed a third of covid patients had self reported symptoms at 12 weeks. It seems no-one stopped to think whether that seemed realistic. The authors admitted that the offer of a free at home antibody test will have created bias in who responded yet they pressed on and extrapolated their findings to a claim that nearly 2
million, or 1 in 36 of the population had long covid by May 2022. The government disseminated this information and the headline writers then joined in too. The proliferation of this massive number meant the actual gap between reality and long covid could be hidden and dismissed.
How common was it really? A research group at King’s College London established a symptom tracking app, the Zoe App, in early 2020. 4.7 million people used it to enter daily symptoms. Because this followed people before they had an infection there is less room for bias. They found not a third, but only 2.3 percent had self reported symptoms (of any kind) at 12 weeks. That would mean the total in May 2022 would have been in the tens of thousands not 2 million.
For long covid, every coincidental problem that people have after a positive test was attributed to covid. For post vaccine problems, every genuine problem was dismissed as a coincidence.
Imagine a study that set out to define “long vaccine”. Every patient admitted to hospital within 28 days of their vaccine would be described as a “vaccine patient”. All subsequent health conditions in this population that were over and above the general levels in the population would be
described as “long vaccine”. It would be obvious that this would massively exaggerate the problem and would include all sorts of conditions that are simply more likely in the kind of population who end up in hospital for any reason. However, when the word covid is attached people become blind to these biases.
The timing of the rise in disabilities is critical. Through 2020, there was nothing unusual about the number of people describing themselves as long term sick. The spring covid wave left no trace on these figures and neither did the first covid winter. The numbers only rocketed from May 2021 and the exact same timing was seen in the USA. The lack of impact on long term sickness prior to spring 2021 does not mean long covid did not exist. It simply means the numbers of people with long covid were equivalent to the numbers with post viral syndromes and long pneumonia seen in previous years. The timing of the rise in disabilities was ignored.
The strongest risk factors for developing long covid were being female and having mental disorders especially anxiety. One study showed 48 percent of those who developed long covid had a mental health
problem, predominantly anxiety, and these rates were double the rates in the control group. These risk factors are also predictive of other physical symptoms regardless of the presence of an infection. The clincher should have been that having had covid, as measured by antibodies, was not a risk factor only the belief that one had had it. None of this evidence seemed to shift the belief that the disabling event was due to long covid.
Even when a study claimed the symptom most predictive of long covid was having no symptoms at all, the believers doubled down. The founder of USA long COVID advocacy group Survivor Corps said“What’s the symptom of acute COVID that is most predictive of #LongCovid? Being ASYMPTOMATIC. No one is protected against #LongCovid. Fear it like the devil.”
11. Did the vaccines prevent long term symptoms?
Blind faith led to the oft repeated claim that vaccines would prevent long covid. The Zoe App data showed there was no difference in the likelihood of having persistent symptoms based on vaccine status. Concerningly, 98 percent of the long covid reported in the study from spring 2021 was seen in the vaccinated group.
There were studies that claimed vaccines prevented long covid but they used more statistical chicanery. One method was to compare long covid rates in spring 2020 in the unvaccinated patients, a disproportionate number of whom were only tested because they were hospitalised, with rates in the vaccinated after omicron. Rates of long covid after omicron infections were much lower in the unvaccinated as well as the vaccinated so claiming that was a vaccine effect is, at a minimum, disingenuous.
The vaccinated population seemed to fare even worse when they then encountered the virus. By September 2021, Peter Hotez admitted, “I’m also concerned about high rates of long covid in vaccinated breakthrough cases.” Whereas the long covid rate was claimed to be a 2.3 percent in the unvaccinated ZoeApp population, for the vaccinated in Australia it was 18 percent and this was after Omicron infections where the risk is far lower. One Swiss study presented the data in a very odd way by reporting rates among vaccinated people who had been unvaccinated when they had covid. This allowed them to claim an 18 percent long covid rate in the “unvaccinated” even though this was a vaccinated population. Of those who had recovered from covid at 6 months after infection, all of them deteriorated at a later date, yet there was no discussion about what might have caused that.
An Australian paper also made the claim that vaccination protected against long covid. The claim was based on lower rates of long covid in a niche population who had had more than four doses. These were predominantly over 70 year olds who had the lowest underlying risk of long covid. Furthermore, the definition in this paper required 90 days of illness and most of those who had had 4 doses would not have had that long since infection to qualify as having long covid. The authors hid the data on the unvaccinated grouping them with those who had had one and two doses and then quoted the covid scriptures saying ”our results add to the growing body of evidence showing that COVID-19 vaccinations are associated with a reduced risk of developing Long COVID.”
The study included all covid positivetests in Western Australia. Fewer than 80 percent had had three doses yet 93 percent of those with long covid in the study had had three doses. When it was clear Australia had a vaccine induced problem, Queensland’s chief health officer said long covid was no different to any other post viral syndrome and should be ignored.
12. How much long covid was really long vaccine?
The ZoeApp team also showed an interesting change in what were called long covid symptoms before and after vaccination. Both the spring 2020 Wuhan wave and the post vaccine Delta wave resulted in a similar number who had persistent respiratory symptoms. However, after Delta there were three times as many who had neurological symptoms with no mention of respiratory symptoms. In addition the number who had multi-organ, systemic and immune related symptoms was five times as high. Did these people have a vaccine injury in addition to or rather than long covid?
Public health authorities use data for what people search for on Google as a tool for tracking covid. In theory it is imperfect because news stories can affect search numbers as well as sickness, but in practice it is a useful tool. If long covid was a significant problem you might expect Google searches for “long covid” to rise and fall with a lag after the searches for “covid symptoms” but both search terms were perfectly in synchrony. As soon as people recovered from acute covid they stopped searching for “long covid”. Searches for “vaccine side effects” aligned with the first two doses of the rollout but were far lower for the third dose. However, Google searches for “long covid” surged after the booster doses in late 2021. Were those people who were most concerned about covid and long covid and therefore most likely to take a booster also those least open to the idea of vaccine side effects? If so, the fact that long covid has been measured and studied based on self reported symptoms may mean that adverse reactions have been mislabelled as long covid.
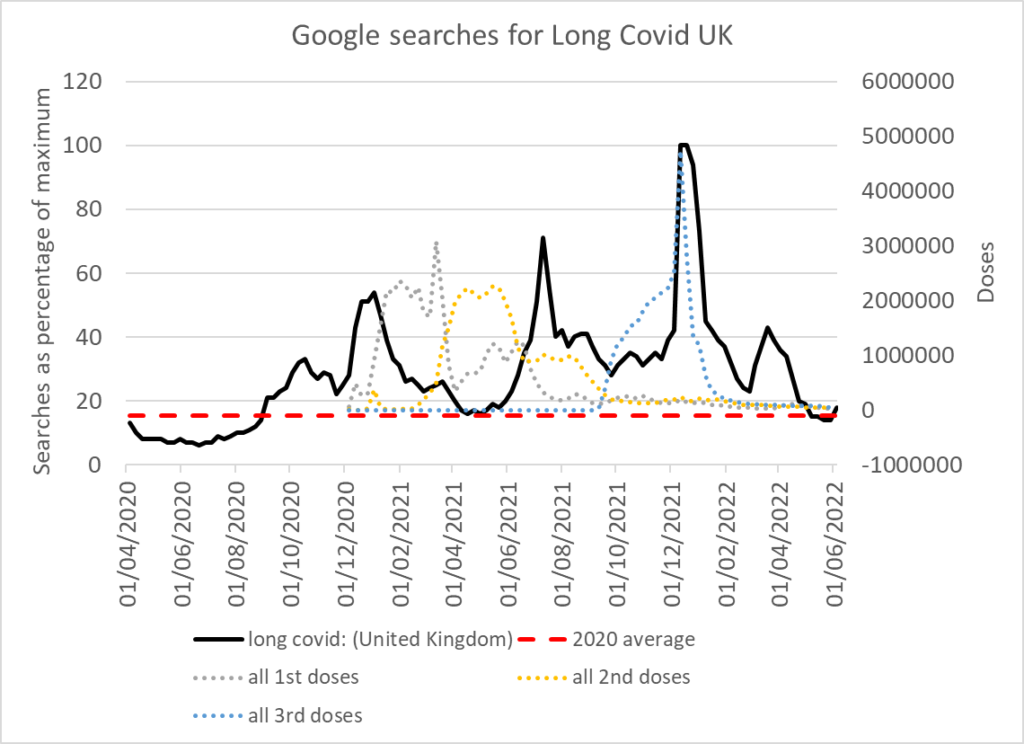
Figure 3: Google searches for “long covid” plotted against vaccine doses and the 2020 average number of searches
The Imperial survey study that claiming 2 million people had long covid showed a much higher risk of reporting long term symptoms among the older cohorts and in health and social care workers. The study was in early 2021 when these were the only vaccinated groups, yet the v-word did not get mentioned at all. Very few long covid papers examined the relationship to vaccines, but little bit by little bit the association became evident. In January 2022, Sciencemagazine said there were rare instances where the vaccine caused long covid and eighteen months later said this “rare” link was starting to “gain acceptance.” They estimated 1 in 450 vaccinated people would end up with a small fibre neuropathy affecting their heart rate and blood pressure. That is too common for a definition of “rare” to apply.
During the vaccine rollout, researchers at Yale University and others suggested, based only on anecdotal evidence, that vaccination could reverse long covid symptoms. The reverse was true. In February 2024, it was shown that when people with long covid were given a vaccine it “prolonged symptoms of long-COVID for more than one year after the initial infection.” A group who designed a test for long covid demonstrated that it was caused by the immune response to residual spike protein. They went on to show spike protein “alone delivered by vaccination can cause similar pathologic features”, and concluded it may be a “major contributor” of long covid symptoms after infection or vaccination.
13. Long covid unknowns
There was a serious lack of meaningful research. The US government committed $1 billion to long covid research but, after two years, not a single patient had been recruited to a treatment trial. The UK government claimed to have spent £314m on specialised healthcare services for people with long covid. Anyone with long vaccine had to go along with the lie that their condition was caused by the virus in order to get treatment. That meant contributing to the inflated claims of the effect of the virus.
Long covid, i.e. post viral syndrome does exist but attempts to exaggerate the problem have distorted people’s perception of the risk, keeping them scared. Numbers have been inflated by failing to properly define the syndrome and allowing self reporting of every medical condition as long covid. Severity has been inflated by equating someone with a long period of loss of smell or a lingering cough to those with debilitating fatigue. The failure to be honest about vaccine injury may also mean that substantial numbers of people who believe they have long covid were actually harmed by vaccination. A failure to acknowledge this possibility prevents vaccine injury being properly defined and measured.
The one measure we do have is the tip of an iceberg of the total number of people unable to work because they are long term sick. People who were sick managed to sustain work for varying periods before giving up. Thankfully, the rise seemed to plateau at the end of 2023 such that the number of newly long term sick matched those no longer sick. However, it is worth reiterating that there are an extra 800,000 long term sick on top of the 2 million pre-2020. Since the vaccine rollout, an extra 1 in 53 working aged people in the UK is now not working because of long term sickness.
