

Exaggeration of impact of COVID-19 on healthy children
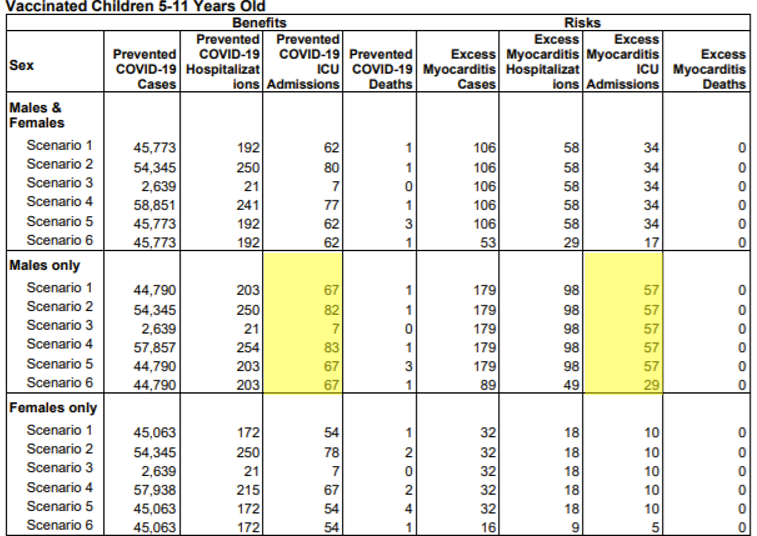
The FDA have published their reasoning behind justifying the vaccination of children aged 5 to 11 years old. The table, reproduced below, shows their estimates of risk of ICU admissions and deaths, in hypothetical future Covid waves, against the guaranteed risk from myocarditis if vaccination is carried out.
In England, there were 291 children on intensive care with a Covid diagnosis up to May 2021. Just over half were under 12 years olds and, if we assume an even age distribution, that would represent under 100 patients on ICU aged 5-11 years old over the course of a year. Extrapolating to a population of one million children aged 5 to 11 this works out at 20 per million children.
The fact that only 30% of the children ‘admitted’ to ICU with Covid had a positive test before arriving in intensive care, casts doubt on the number of genuine Covid PICU admissions. The Paediatric Intensive Care Audit Network (PICANet) say “These children may not primarily be in PICU because of Covid-19 but all tested positive to the virus either prior to or during their PICU admission.”
The FDA claims that vaccination could prevent between 60 and 80 ICU admissions per million children aged 5 to 11 in just a 6 month period. That would mean 120 to 160 over the course of a year or 6 to 8 times more admissions than were seen in the UK.
To reach such a conclusion the following assumptions must have been made:
- Natural immunity in those children who have been infected does not exist
- There is no such thing as hospital transmission to children who are already sick for another reason
- Children with co-morbidities are at no greater risk than children who are healthy
- Vaccination can prevent the vast majority of intensive care admissions
- There is no vaccine waning in children
These assumptions are so extreme that presenting the data in this way to create a case for vaccinating healthy children amounts to negligence if not outright fraud.
The JCVI were more careful in their calculations. They carried out a calculation that estimated only the risk for otherwise healthy 12 to 17 year olds. (A healthy child admitted to intensive care for another cause, e.g. meningitis, who then contracted Covid in hospital would be counted as a preventable Covid admission). They concluded that giving all 2.7 million 12 to 15 year olds in England one dose might prevent 7 ICU admissions of healthy children. Given the risks of vaccination they therefore felt they could not recommend vaccinating this age group. It was the four Chief Medical Officers who made the recommendation for children this age.
The FDA compares the risk from Covid to the risk of myocarditis. Even on their own figures, the risk of intensive care admission for males due to post vaccination myocarditis (see table) is of the same order as the allegedly prevented intensive care admissions. It is hard to see how it fulfils the FDA criteria for emergency authorisation:
“The known and potential benefits of the product, when used to diagnose, prevent, or treat the identified serious or life-threatening disease or condition, outweigh the known and potential risks of the product”
The figure they use for the risk of myocarditis is 1 in 10,000 with a third requiring intensive care. It is not unusual for the risk of an adverse reaction to a drug to become higher as time passes partly because attention is drawn to the issue and it is measured more accurately. Ontario public health estimates the risk per million to be higher than this when adding the risk after first dose to the risk after second dose, with a considerably higher rate in younger age groups. For example, the rate after the second dose of Pfizer is estimated to be 92 per million in males aged 12-17 compared to 43 per million in males aged 18-24 years. It is highly likely that a 1 in 10,000 risk for children aged 5 to 11 is an underestimate. No consideration has been taken as to the longer term impact of myocarditis nor what effect priming the immune system with vaccination has on myocarditis rates in those children who then encounter the virus. In the words of the FDA:
“Information is not yet available about potential long-term sequelae and outcomes in affected individuals, or whether the vaccine might be associated initially with subclinical myocarditis (and if so, what are the long-term sequelae).”
The FDA paper ends with a note that a 5 year trial will begin
“to characterize the clinical course, risk factors, resolution, long-term sequelae, and quality of life in children and young adults <21 years with acute post-vaccine myocarditis/pericarditis.”
Myocarditis is not the only adverse reaction to which children who are vaccinated will be exposed. During the swine flu epidemic which is alleged to have killed 70 children in England, the Pandemrix vaccine was withdrawn from the market when it was shown to be causing narcolepsy in 1 in 50,000 recipients. Given that only 20 children have died ‘with’ Covid in the 5 to 14 year old cohort, most of whom had serious co-morbidities, there is simply no reasonable argument for vaccinating this age group given the known adverse events risks.
The decision to vaccinate children is reckless and the way the data has been presented as representing the risk to healthy children, is, whether deliberately or not, fraudulent.
