Americans seem to think so
All HART articles also on Substack. Please consider a PAID SUBSCRIPTION so we can continue our work. Comments are open so you can join in the conversation.
The CDC advice for this autumn is for everyone over 6 months of age to have a flu vaccine and a covid vaccine. Moreover if you are a baby, or a ‘pregnant person’ or an over-60, why not throw in RSV protection too? You’ll be pleased to know you can get all three shots on the same day, three for the price of one! What could possibly go wrong? To be fair, they tell you –
‘Getting multiple vaccines at the same visit may increase the risk of some side effects from vaccination.’
Studies of combined flu with covid jabs have shown increased side effects, as have other studies of flu combined with RSV. There have been no studies of all three!
Of note, in the UK, routine covid boosters are only recommended for those with underlying health problems or the over 65s, so if you are a healthy under 65 no need. This implies either that all Americans are unhealthy or that the UK authorities are ‘anti-vaxxers’ or possibly both.
For older adults in the UK receiving their invites, there is new wording on ‘seasonal’ protection which is quietly moving covid jabs into the same yearly pattern as flu jabs. Encouragingly titled ‘Seasonal vaccinations and winter health’ the NHS article states:
‘There are some things you can do to help yourself stay well in winter. This includes getting your flu and COVID-19 vaccinations.’
The invitations sent out by Dr Nikita Kanani from NHS England state:
‘Seasonal vaccinations have proven safety records.‘
This conflating of covid boosters with flu vaccines as ‘seasonal vaccinations’ and then ascribing them a ‘proven safety record’ is grossly dishonest to put it mildly.
Dr Kanani’s letter goes on to say
‘They give additional protection to any immunity you may have from previous infections.‘
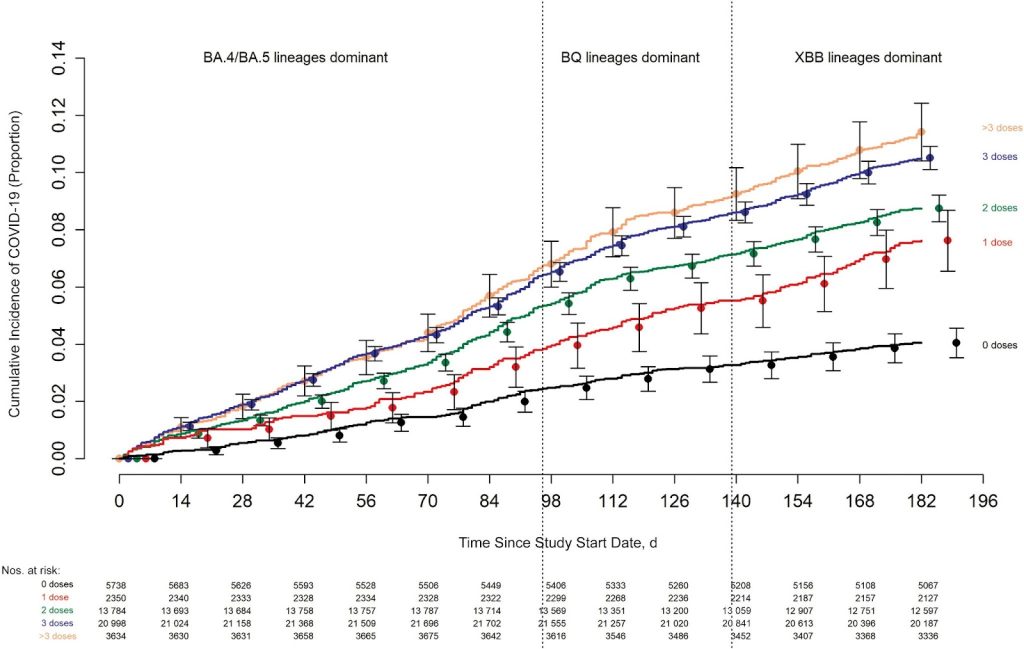
Odd that, given evidence that the more doses of covid vaccines you receive, the higher your chance of catching covid, as shown neatly in Figure 1.
The problem with the flu vaccines as a bedfellow for covid boosters, is that they also have a poor reputation for efficacy though not quite so poor for safety.
On the efficacy side, ‘seasonal’ flu vaccines have now been in place for decades, yet the evidence that they have reduced mortality has been called into question. Figure 2 shows all-cause winter season excess deaths in the US from 1968 through to 2001. The authors attribute the drop in mortality in the ‘70s to immunity acquired naturally during the 1968-9 pandemic. Mortality rates then climbed over the subsequent two decades at a time when influenza vaccine uptake rose from 15% to 65%.
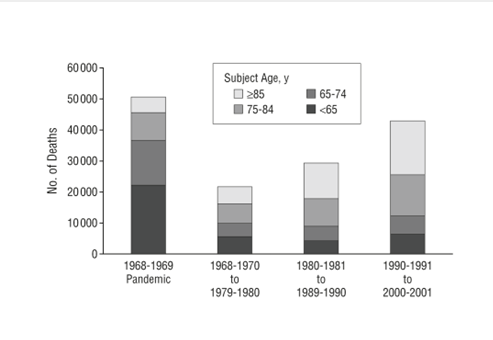
Complex age adjustments correcting for an ageing population flattened the increase in deaths from pneumonia and influenza but revealed no reduction in any age group despite the rising vaccine uptake. Possible mechanisms for the poor efficacy of flu vaccines are fully discussed here. A small RCT from Hong Kong showed a fourfold increase in non-influenza viral infections in vaccine recipients (relative risk: 4.40; 95% confidence interval: 1.31-14.8). In another study from Western Australia reports 58% efficacy in its abstract but if you can get past the paywall to look at Table 2, you find that seasonal flu shots doubled their risk of illness from non influenza virus infections (unadjusted OR 2.13, CI 1.20—3.79). Another more recent paper discusses the interaction of upper airway organisms. All of these failures have been summarised in an excellent rapid response in the BMJ.
On the safety side, lumping flu and covid vaccines together as ‘seasonal vaccines have proven safety records’ completely overlooks the ever-increasing evidence that mRNA vaccines have an appalling safety track record, too big a topic for this particular article.
What about children?
When it comes to flu immunisations for children, we enter even murkier, ethical territory.
As Sally Beck points out in a recent article in TCW, schoolchildren are primarily being given the ‘FluMist’ vaccine to protect babies and the elderly. The live attenuated intranasal vaccine (LAIV) appears to be more ‘effective’ than the intramuscular dose used in vulnerable adults, in part because it targets the entry point for flu viruses rather than stimulating antibodies against viruses reaching the blood stream.
But because the nasal vaccine is a ‘live attenuated’ vaccine, it is not suitable for those with a poorer immune system. Listed in the bnfc as common or very common side effects for all live vaccines are: abdominal pain; arthralgia; diarrhoea; fever; headache; myalgia; nausea; skin reactions; vomiting with a bonus of ‘nasal symptoms’ for the live flu vaccine. Other potential side effects include an increase in nasal carriage of other organisms, such as streptococci and haemophilus influenzae. Other side-effects listed include wheezing and children with severe asthma are advised to speak to their doctor! Many parents have reported an increase in school absence in the days after the vaccine and concerns have been raised that children whose parents declined the vaccine would nonetheless be exposed via their class mates, but data on this is not forthcoming.
LAIV is specifically contra-indicated in the immunocompromised. The UKHSA guidance for healthcare practitioners specifically states: ‘If the child is a household contact of a very severely immunosuppressed individual (for example bone marrow transplant patients requiring isolation) an inactivated flu vaccine should be given instead of LAIV.’ This begs the question of whether it is suitable to give the programme in schools, where individual informed consent may be sketchy. We have previously discussed whether school premises are really suitable for vaccinations.
Fortunately, healthy children are not being recommended to take a covid booster, indeed no healthy under 65s are even eligible for a primary course now (if anyone originally unvaccinated should change their minds – an improbable scenario) But for children with health vulnerabilities, concerns about effects of repeated boosters on immune function (see examples here and here) are highly relevant. And for any teenager being tempted to take a booster to protect an immunocompromised household contact, just look back at Figure 1 above and ask yourself how taking this vaccine protects anyone.
Perhaps the best judgement on flu and covid vaccines comes from NHS staff, of whom by late November only 28% had taken a flu jab and a mere 21% had taken a covid booster.
