
But panic not – private covid jabs available soon for over-12s in a pharmacy near you
On 1st February, the website Chemist And Druggist announced the launch of private covid jabs, under the headline UK’s first private pharmacy COVID-19 vaccine service launched today
This is a slight over-statement, in that supplies are not likely to come till April, but is nevertheless a warning of the direction of travel. Over the next few days, several pharmacy groups made similar announcements. The scheme will be available for age 12 and upwards and will initially provide Novovax, a spike protein-based vaccine but with Pfizer and Moderna’s mRNA products likely to follow. The implication is that this will be open to those not covered by the NHS programme – why else would anyone pay £45 for a vaccine they could get for free, particularly given that provision of vaccines seems to be the one thing which has continued with easy access and no waiting list?
The article says that NHS covid jabs are available to >65s or those aged over 6 months with listed underlying health conditions and those aged over 12 with an immunocompromised household contact. We wrote previously to the JCVI regarding the autumn booster programme’s unethical inclusion of vaccines for healthy adolescents to protect others and not themselves. We have yet to see minutes of the discussions which led to that decision, though an FOI request did reveal that they had taken no legal advice and that they had no calculated NNV (number needed to vaccinate) for how many healthy children needed a booster to prevent serious illness in one immunocompromised household member.
The article listed the NHS eligibility criteria for the Autumn 2023 boosters, but noteworthy is the latest JCVI guidance for the Spring boosters published on 7th February. This is now even more limited, with three criteria only:
- adults aged 75 years and over
- residents in a care home for older adults
- individuals aged 6 months and over who are immunosuppressed
Gone is the category of <75s with co-morbidities, so immune compromise is the only remaining risk factor of note apart from age.
The JCVI document makes for some interesting reading. Firstly, the graph on covid hospital admissions by age is something the mainstream media should have been sharing as an antidote to fear for the majority of the population. As JCVI states, “Data on hospital admission rates in the UK is consistent with the clinical risk being highest in those aged 75 years and older.” Note: the orange dotted line corresponds to the age group in the subplot title, while grey solid lines correspond to all other age groups, with said dotted lines almost invisible for ages 0-44, and not much happening for 45-64s either. Remember, these are hospital admissions, not intensive care let alone deaths.
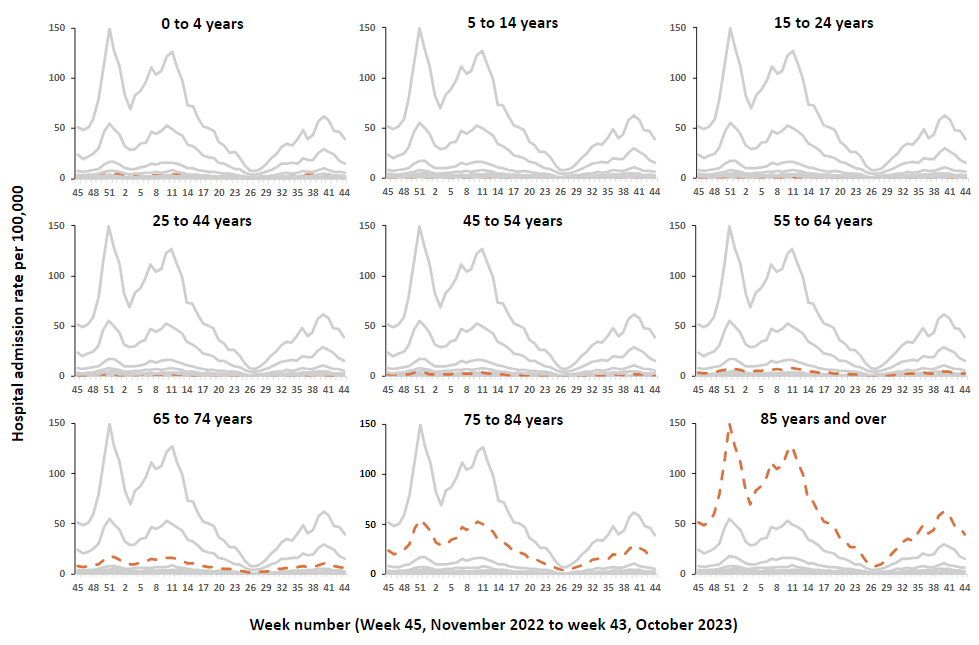
Figure 1: Weekly hospital admission rate by age group for new COVID-19 positive cases reported through SARI Watch, November 2022 – October 2023.
The second important inclusion is a section on cost effectiveness. “Utilising a deployment cost of £25 per vaccine (as estimated by NHS England), the non-standard cost-effectiveness assessment for booster vaccination in spring 2024 indicated that, within the assumptions describing the most plausible projected scenario, vaccination was likely to be cost-effective when offered to the following groups:
- all adults aged 90 years and over not in a clinical risk group
- all adults aged 80 years and over in a clinical risk group
- all adults aged 65 years and over with immunosuppression
Just read that list again. Yes, you did read it correctly, over 90s are the only age group for whom regardless of comorbidity, they deem the vaccine to be cost-effective. Otherwise only cost-effective for over 80s with any of the listed clinical risk groups. Interestingly the Norwegian Medicines Agency advised caution for vaccination over 80s especially with comorbidities because of early post-vaccination deaths, but don’t worry about great-grandpa, it’s called ‘kill or cure’. As for 65-79s it is only cost effective if you are immunosuppressed. For under 65s, however sickly, covid vaccines are not deemed worth the candle. We are not talking about a costly drug here, this is calculated on a total cost, including administration of £25.
However, undeterred JCVI proceed to offer the vaccine to a wider group of all over 75s on the basis that “It is also recognised that a high proportion of older adults are living with comorbidities and that vaccine uptake is higher in universal age-based programmes.” I can see that GPs would find it easier to send invitations (why does that word make me think of nice things like birthday parties?) to anyone born before 1949, but the invite could simply list the conditions and say “if you have any of the following conditions, we recommend you book a covid booster but if you are in good health, you don’t need it.” I know many 75-year-olds who might like to know they are thought to be too dopey to understand such a complicated message.
To return to the headline, many will argue that if it is not cost effective for the NHS to spend its (aka ‘our’) money on, then let people pay themselves. But this should assume fully informed consent. If the legal challenges against AstraZeneca succeed, the argument is that the drug did not comply with the Consumer Protection Act in that the vaccine was not as safe as the public were entitled to expect. Of course, AstraZeneca has been quietly mothballed but court cases against Pfizer and Moderna will surely follow. This could put pharmacies in the invidious position of promoting something which later gets withdrawn on safety grounds.
Of note, the first drug to go up for private use is Novovax, perhaps because it is not being taken up in the NHS? It is a standard vaccine, so at least has the advantage that it won’t be telling its recipient to make an unknown quantity of spike protein in unknown parts of their body for an unknown period of time. But it is still based on the spike protein, and the trial reports 64% systemic adverse events after the second dose, with the usual statement that, “Systemic adverse events were reported more often by younger vaccine recipients than by older vaccine recipients”. As with all the covid vaccine trials, both the numbers involved and the follow-up time, lack the power to quantify any serious adverse events.
Whatever the arguments for adults, it surely cannot be ethical to sell to parents a drug aimed at protecting grandparents, which will clearly fail in that aim but will at the same time put the adolescent at significant risk of harm. We don’t ban smoking but it is illegal to sell cigarettes to children for a very good reason.

At least the JCVI don’t want to damage Kids even if schools do. Perhaps we’ve ran out of credit to pay for them. Best to be prepared for the horrendous levels of circulating viral disease in the Summer. Its great to see that I’m too young to make the cut after 3 years of refusal. Pharmacies can not give informed consent (even if they are capable) and need to beef up their insurance cover. I’ll just have to content myself with lying in the sunshine.
Glad you stuck to your guns. People tell me parents should be allowed to choose but that doesn’t seem at all fair on the children if parents are encouraged to choose something which is known full well by the JCVI to be harmful.