

The new face of coercion
Unvaccinated children sent home from school as a ‘National incident’ is declared. Does that ring any bells? Well maybe if you had lived in Lithuania or California during the recent pandemic. But here in the UK, those strident voices warning of ‘consequences’ for citizens declining an offer of a covid vaccine were generally ignored.
HART covered the beginnings of this story in September, when the BBC reported “Mathematical calculations suggest an outbreak could affect between 40,000 and 160,000 people”. Yes you’ve guessed it, not the killer novel coronavirus but the killer well-known measles virus. At that point it was London where the mini-outbreak was occurring although cases there were already declining steadily and have continued to do so (see figure 3 below).
Fear mongering now being the order of the day, and vaccine-hesitancy apparently a major risk to global health, we suddenly find that MMR vaccination is mandatory for Birmingham school-children. It is not quite expressed like that but the effect is the same.
If there is an outbreak of measles in your school or nursery and you are unvaccinated, you will have to stay home for three weeks. (Note an outbreak can be declared after 2 cases).
Two questions immediately spring to mind. First, who is to blame for the fall in uptake of childhood vaccines? Is it really those of us who have been cautioning against covid vaccines for children or is it more likely those regulators and governments who have been pushing a new vaccine with inadequate safety testing onto healthy children at virtually no risk from SARS-CoV-2 infection? UsforThem’s recently commissioned survey would suggest the latter has played a significant part in reducing parents’ trust in government advice for other vaccines, not just for Covid-19. They reported:
- Only half the public (52%), and just 40% of 18-35 year olds, think the Government was honest about the risks and benefits of Covid vaccination.
- Just 60% of parents of children under 18 say they would now be likely to give their child vaccines recommended by the Government (down from 84% having said that they would have done so prior to the pandemic).
The second important question is why measles, which occurred regularly in childhood in the past, is now considered to be so dangerous as to be classed as a National incident? Is this ‘Crying wolf’ – maybe?
As shown below, deaths from measles in England and Wales had almost disappeared more than a decade prior to the arrival of the measles vaccine.
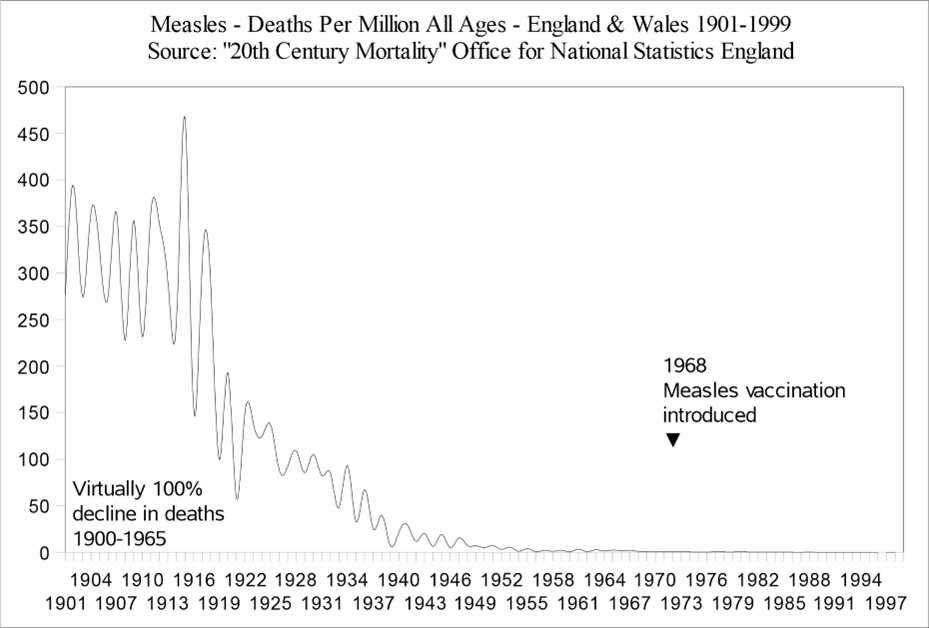
Figure 1. Data from Twentieth Century Mortality CDROM Measles mortality. ONS.
Of course, measles can still be a killer in low-income countries, in the face of malnutrition, and extremely rarely even in well-nourished populations. But characterising measles as a high mortality disease is clearly not applicable in 21st century Britain. Even hospitalisation risks have been significantly overstated. In her Ministerial statement, Maria Caulfield said, “One in five children with measles will need to be admitted to a hospital for treatment – which could put additional pressure on the NHS.” (note the ‘protect the NHS’ message thrown in for good measure). This 1 in 5 statistic is headlined in the Mirror with a picture of a rather miserable but alert child in a hospital bed. It is not clear where Ms Caulfield obtained the data to support the claim, but an outbreak in Europe in 2018 reported as high as 61% admission rates. However, a rapid response to that article, quoted nationally collected data for England and Wales between 1948-1962, which gave an admission rate of only 3%. Why the difference? Are children today so much less healthy, or are today’s parents (or indeed GPs) so much more anxious that children are being admitted unnecessarily? Also what is the denominator? Many children in the past with measles would have simply been cared for at home and therefore not notified. A HART member recently visited a friend whose child had measles and whose mother was reluctant to call her GP for fear of an ear-full regarding her son’s unvaccinated status. She is likely not alone.
Moreover, there is a cheap readily available vitamin which should be in use, but its existence gets no more coverage in the UK press than did vitamin D as an immune booster in the face of SARS-CoV-2 (or any other infection, come to that). WHO has for many years recommended Vitamin A supplements routinely and also in high dosage given at the outset of measles infection, this advice repeated as recently as August 2023. A Cochrane review published in 2005 confirmed that “two doses of vitamin A (200,000 international units (IUs) on consecutive days) reduced the mortality in children aged less than two years (RR 0.21; 95% CI 0.07 to 0.66)”. Why is this not mentioned in the latest National measles guidelines?
Meanwhile, measles cases fluctuate month on month and with mini-outbreaks every 5 years or so, as they always have done. Is 2024 really going to be so much worse than 2013?
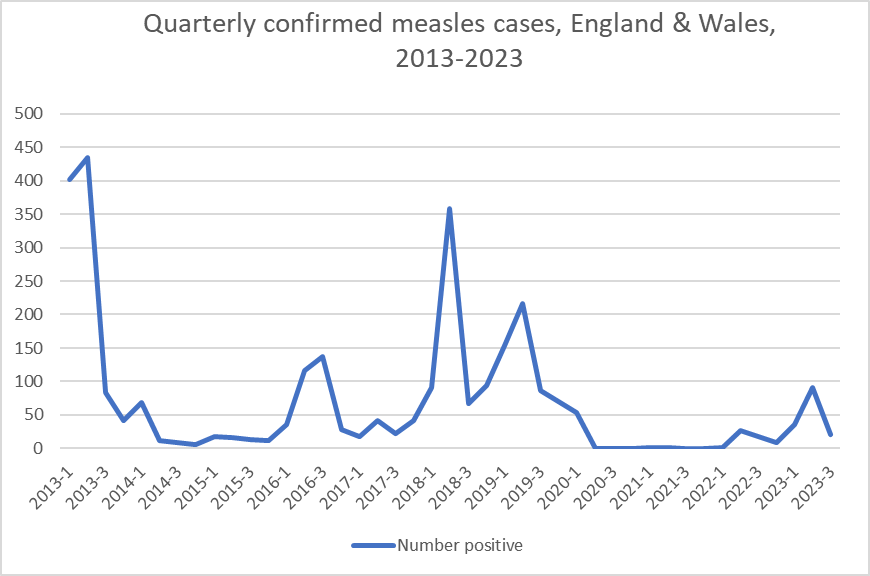
Figure 2. Measles notifications, 2013-2023, taken from UKHSA data.
Talk of a major outbreak in London of somewhere between 40,000-160,000 cases covered by the BBC in July 2023, certainly didn’t materialise (see Figure 3). Note the latest data point on the chart shows cases increasing nationally, but this is based on unconfirmed cases for the latest data point, but confirmed figures for all the earlier points (confirmed numbers always lower, once antibody results become available, since not every rash is measles).

Figure 3. Laboratory confirmed measles cases by month of onset, London and England.
It is known that measles is more serious either in infancy or in adults, so assuming MMR vaccine hasn’t actually become mandatory overnight, why not let measles circulate naturally in schools, given that those who are immunised should be protected and those parents who declined, in theory at least should have understood this would mean that their child might get measles. For a small number of children with immune deficiency, will it really be safer to have sporadic cases ongoing than to have a short sharp outbreak following which their unimmunised classmates will have life long immunity? Perhaps someone has done some modelling on this question! Passive protection with immunoglobulin is available too. Most schools however, at any given time will not have a pupil or staff member requiring such protection.
One concern which has been raised is of an increase in young infants with measles – is this related to antibody levels in their vaccinated mothers being lower than used to occur with naturally-acquired immunity and hence protection of newborns by antibodies across the placenta wearing off more quickly? It is noted in the latest National measles guidelines that of those born before 1970, over 99% had protective antibodies, compared to only ~90% of those born between 1970 and 1989.
The UKHSA, with its declaration of a National incident, is obviously hoping there will be an increased uptake of MMR vaccine. It is not clear whether sending unvaccinated children home is a carrot for the other parents or a stick for these. Either way, it smacks of a lack of informed consent freely given. And will any campaign consider mentioning potential side effects, as listed in the patient information leaflet?
Meanwhile the Independent has gone one step further with an article loudly demanding that measles (and potentially several other vaccines) should be made mandatory in order to access state education child benefits:
The key to making vaccination mandatory is to confront parents with a hard choice, by making free state education conditional on certain vaccinations being carried out at prescribed times – a vaccine passport, if you like. The same could apply to child benefits. The parents remain free to choose – but the choice to risk other people’s health comes freighted with penalties.
Is this the face of things to come? Miri Finch of Informed Consent Matters, clearly doesn’t think so.
