UKHSA insist on using nonsense vaccine effectiveness measurements
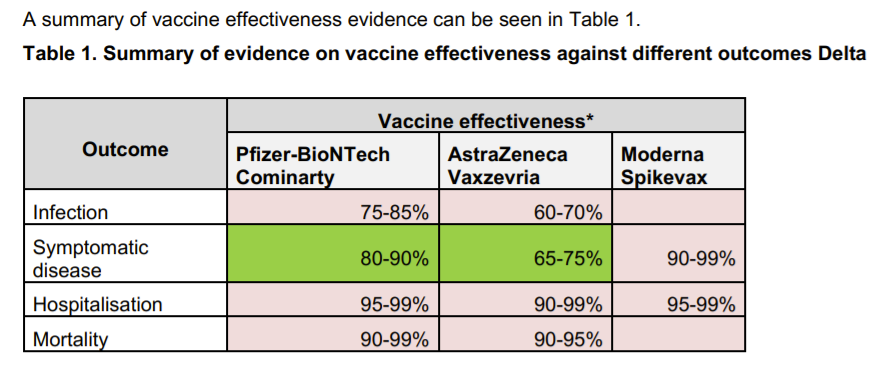
Each week UKHSA publish a table on vaccine effectiveness. Recently they have tried to stop people calculating vaccine effectiveness from the real world data. Rather than doing that, instead we can see what their claimed vaccine effectiveness would mean in the real world. On the basis that around half the vaccines given have been Pfizer and half AstraZeneca we can assume an overall vaccine effectiveness of the mean i.e. 70% against infection which is being claimed.
Using these conservative estimates with the real world data of the number of people testing positive, we have to conclude one of two things:
- The population of unvaccinated is much smaller than UKHSA measure or ONS estimate
- The unvaccinated are getting secretly infected and not being tested
Given the real world data, in order to achieve a vaccine effectiveness of 70% after 2 doses, there would have to be 7.5 million ghost adults in UKHSA’s NIMS database or 2.1 million ghost adults in the ONS estimates, leaving only 2.4 million unvaccinated adults in the whole country.
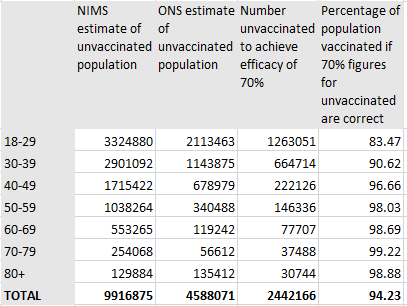
Our population distribution would become very skewed if this was correct, with over half the additional ghost people being under 40 years of age.
What if the real issue is not the population estimates but unvaccinated people not getting tested so often? How many secret cases in the unvaccinated would there have to be?
To get a vaccine effectiveness of 70% there would need to be an extra 200k cases in the unvaccinated and we would have to assume that 50% (ONS) or 80% (NIMS) of the unvaccinated positives had not been tested.
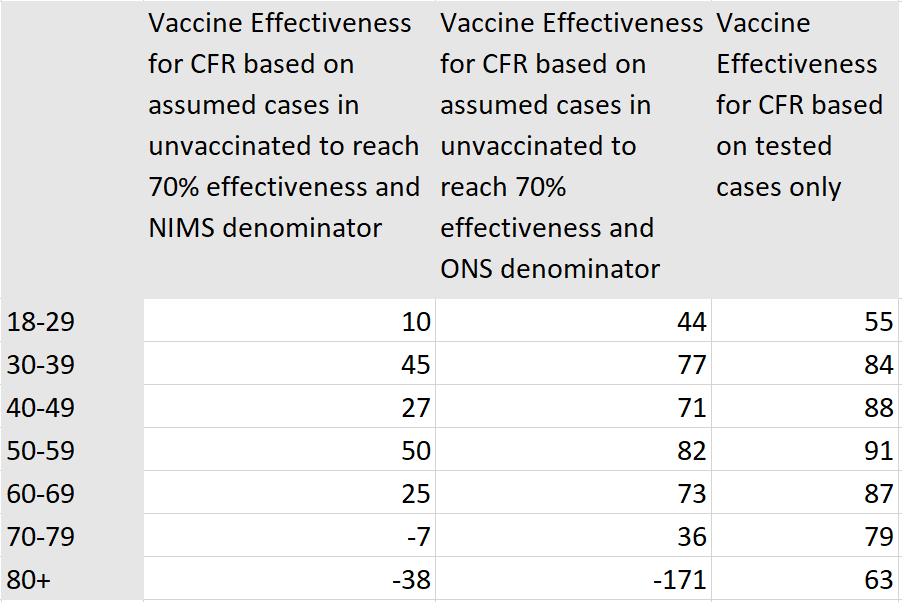
The problem with believing that, is that the vaccine effectiveness at reducing case fatality then plummets and reaches negative values in the elderly. On the other hand, using the calculation based on those testing positive, shows a consistent vaccine effectiveness value across age groups but with evidence of waning effectiveness in the elderly. (The numbers of deaths in the 18-39 year old category was thankfully too small for the calculations to be meaningful).
These findings would not be so dramatic if there were a combination of a smaller population alongside under-diagnosed cases in the unvaccinated. However, a far simpler explanation is that, like influenza vaccines, these vaccines are effective at reducing hospitalisations and deaths but ineffective at reducing infections, particularly after several months or when faced with new variants. Studies from Qatar and Sweden also show no evidence of a reduction in infections.
The case rates in the vaccinated are trending higher even as they are falling in the unvaccinated. UKHSA’s continued denial of reality will start to look more and more foolish if these trends continue. Finally, the failure to admit the likely higher rate of immunity from prior infection in the unvaccinated, let alone a willingness to measure that effect, will make them look more foolish still.
It is time for some honesty about the lack of effectiveness with regards to preventing infection and an end to vaccine coercion. Vaccination may provide temporary benefit to the individual but it has not been shown to benefit the wider community.
