

How serious was it and was it anything unexpected?
Dr Ros Jones
Over the last month, since news first broke about two young people dying from invasive meningococcal disease, much has been written in both the MSM and by more sceptical voices.
The first case occurred on 13th March in a student from Canterbury University and the normal tracing of household contacts for prophylactic antibiotics began. A second case from the same university, an exchange student, was reported the following day by French health authorities but with no clear connection between the two. But also on 14th March, a sixth former from a local secondary school in the city was sadly reported to have died. On 16th March, UKHSA reported 4 confirmed cases and by the following day there were 9 confirmed and 11 further suspected cases. Wes Streeting, Health Minister, gave a statement in the House of Commons on 17th March in which he described the outbreak as ‘unprecedented’. This was perhaps not totally accurate as clusters such as this do occur at intervals but having said that, his statement was factual and clear. There would appear to have been a prompt response, with contact tracing suggesting that most cases arose amongst students attending a particular bar in Canterbury. Antibiotic prophylaxis was provided and targeted MenB vaccine was also offered. Cases continued rising over the next four days to a maximum of 34 cases, of which 13 were then excluded as the relevant strain of Meningococcus B was not isolated from a normally sterile site. Thus there have been a total of 21 cases with sadly 2 deaths. No new cases have been reported since 25th March. The wave of cases would appear to have peaked within 10 days.
So what led to quite such enormous coverage, including internationally and is there anything we can learn?
Press coverage
The BBC went to town over this, as shown in the compilation below put together by Dearchurchleaders.substack.
It reached the New York Times on 18th March and ABC News followed the next day, also including reports of a death in Pennsylvania from pneumococcal meningitis. Several newspapers picked up on the ‘unprecedented’ description. On 20th March, the New York Post ran an article entitled Could UK’s deadly meningitis outbreak spread to the US? Here’s what experts say. Indeed, the press appetite for meningitis stories was such that outlets began recycling old cases to sustain the narrative. The Sun ran a piece during the outbreak about a twenty-year-old woman who had died after missed opportunities in her hospital meningitis care – a tragedy, certainly, but one that had occurred in 2025, entirely unconnected to the Kent cluster. The fact that a story over a year old was being re-reported as if it were current speaks volumes about how few actual meningitis cases there were to report.
Meningococcal disease
Meningococcus, or to give it its full name Neisseria meningitidis, is a bacteria which can be a common commensal in the nasopharynx in as many as 10% of healthy individuals at any given time, and as many as 25% of adolescents. The vast majority of cases of invasive disease are sporadic, with cases occurring every year, plus occasional outbreaks. What makes the bacteria breach the normal mucosal barriers and become invasive, leading to meningitis or rapidly progressing septicaemia, is not fully understood, but has been linked to factors such as smoking, overcrowding, poor general health and immune function. In this recent cluster, the role of vaping was also discussed as a possible risk factor. Undoubtedly there will be genetic differences too in susceptibility.
Peak risk ages for meningococcal disease, as opposed to carriage, are preschool and young adults. Infants and toddlers are known to be at higher risk from a number of bacterial illnesses, one problem for parents being the inability of young children to explain or localise their symptoms, leading to delays in diagnosis. For young adults, a different problem but also leading to late recognition is the move away from home into student accommodation and the similarity of early symptoms such as headache and lethargy being indistinguishable from a hangover. Your student house mates may leave you to sleep it off in the morning, where your mum would have gone in and checked on you. Delay in diagnosis and antibiotic treatment even of a few hours can have devastating even fatal consequences (similar increases in risk are seen for insulin-dependent diabetics in their first year at college).
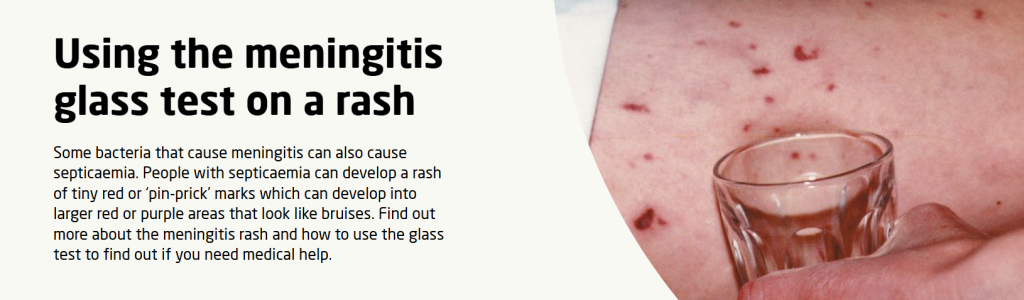
Meningococcal meningitis and septicaemia are statutorily notifiable by registered medical practitioners under the Health Protection Legislation (2010). Household contacts (or school dormitories or in student halls of residence, those sharing a kitchen would be included) are normally given a single dose of prophylactic antibiotics (ciprofloxacin or rifampicin), but the risk of invasive disease is low even in household contacts. Standard public health management includes informing students (or parents where there is a case in their child’s school) with a leaflet describing symptoms to watch out for and usually showing a picture of the ‘glass test’ which may help in distinguishing a haemorrhagic rash for a non-specific one. I have certainly seen secondary cases diagnosed early because of this simple test.
If there is a second case in the same school or institution, then a bigger response would kick in with more active case ascertainment, which is what appears to have been the case in Canterbury, and follows established national guidelines. There seemed to have been some criticism in the press that action had been delayed, but this is not borne out by comparing the published case data with the current guidelines. One problem for public health in the Canterbury cluster was that the first case was in a university student but the first death was in a 6th-former, so even after the 2nd case it was not immediately apparent that this was a cluster. Once students more widely were informed and other cases were diagnosed, the possible link to a popular bar was highlighted.
A question that received remarkably little scrutiny was the scale of the antibiotic intervention. According to the Guardian, approximately 30,000 people in South East England were given ciprofloxacin prophylaxis. Ciprofloxacin is a fluoroquinolone antibiotic that carries an MHRA black-box style warning. The MHRA’s own Drug Safety Update reminds prescribers that fluoroquinolones can cause disabling, potentially long-lasting or irreversible side effects affecting tendons, muscles, joints, and the nervous system, and that they should not be prescribed for non-severe infections unless other antibiotics are considered inappropriate. A single prophylactic dose carries a lower risk than a therapeutic course, but across 30,000 mostly healthy young people, even rare adverse events become probable in aggregate: tendon injuries, neuropathies, and neuropsychiatric reactions are all recognised complications. Were these young people given informed consent? Were they told about the MHRA warning? Or were antibiotics simply handed out at walk-in clinics as though they were harmless?
It is also notable that UKHSA criticised an NHS hospital for not immediately formally reporting the cases saying they waited until there was a formal diagnosis via a confirmed test. This seems inherently reasonable. If UKHSA demanded the reporting of every young person presenting with a fever, a stiff neck or a bit of photophobia, it would create the illusion of an epidemic of meningitis where none existed.
Meningococcal vaccines
There are several strains of meningococcus and the first for a UK vaccine was MenC, introduced into the infant schedule in 1999. There was a steep decline in MenC but a subsequent rise in MenB which therefore replaced MenC in the infant schedule in 2015. MenC was then added to a multi-strain MenACWY, offered at age 14, with the intention of targeting the second spike of disease in late adolescence. This would appear to have been effective, though like many other vaccinable diseases much of the decline seemed to predate the vaccine rollout. None of the young people involved in this outbreak had been eligible to be vaccinated against MenB.
The problem with MenB, the strain in the recent Kent outbreak, is that unlike the MenACWY vaccine, its efficacy wanes after two or three years. It also does not prevent nasopharyngeal carriage. It has therefore only been recommended by the Joint Committee on Vaccinations and Immunisations (JCVI), as a three-dose infant schedule which covers the highest risk age group and then wanes at an age where risk is naturally falling. The same rationale could be applied if it was added into the secondary school schedule in the form of MenABCWY. The JCVI have been asked to look at this again.
In Kent, the initial management of contacts was with antibiotics but a targeted vaccination program was set up and then widened to include around eight thousand students and staff. It is a two dose schedule and unlikely to have any direct impact on containment as the outbreak which increased rapidly had decreased equally quickly within a week.
Unprecedented?
This description given in an official government statement and then repeated in the press will have added to the fear amongst students and their parents. But data in recent years does not fully support this. Carl Heneghan and Tom Jefferson presented the graph below in their Trust the Evidence substack.
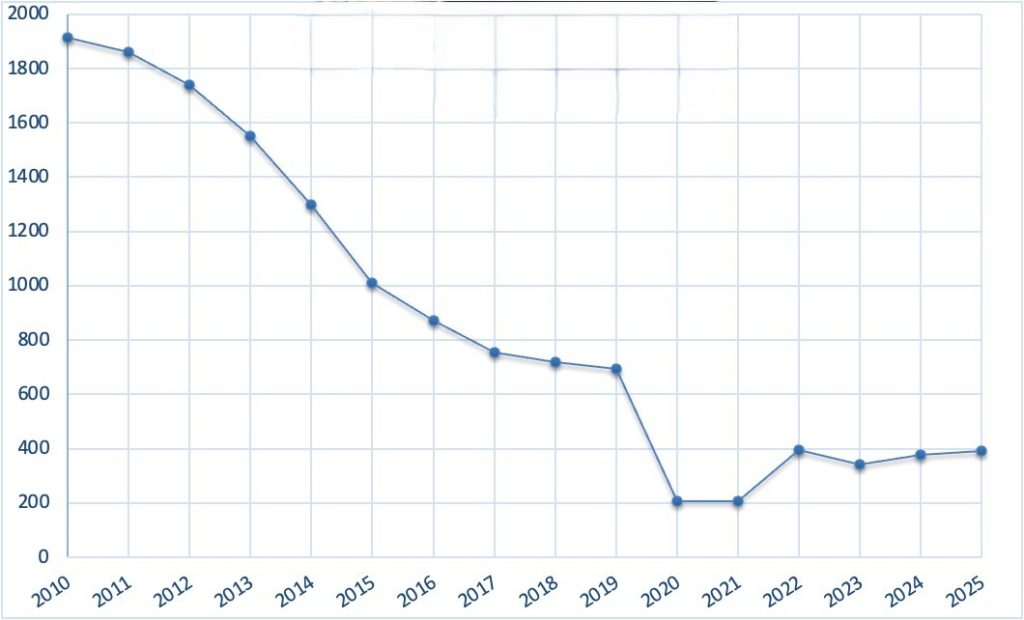
Meningococcal cases 2010 to 2025, England
But as they do agree in their article, the rapid rise and the occurrence of two fatalities was not typical of such clusters. It is not clear why this population of 16-25s in Kent would be any different than usual. Shared vapes at the club they attended have been suggested as a factor. Furthermore, given that around 50% of 12-15s took two mRNA doses in 2021 and evidence of immune dysregulation in adults is certainly well-described, I would also want to know their covid jab status.
The local public health consultant raised the possibility that the latest variant of MenB involved in the outbreak had mutated to become more transmissible or more severe and that scary prospect got picked up by the Telegraph in the headline: Mutant meningitis strain behind Kent outbreak.
One problem which may have given an impression that cases were rising very steeply is the use of PCR testing which will inevitably give false positives, with some suspected cases downgraded if cultures are negative. Having said that, invasive meningococcal disease can progress rapidly so a system which has a high sensitivity and results in a few teenagers receiving treatment they may not have needed is justified. The same cautious approach applies to treating suspected sepsis in the newborn or when immunosuppressed during chemotherapy.
It is also worth examining what counted as a “case” in this outbreak. UKHSA’s own definition of a confirmed MenB case required a clinical diagnosis of meningitis, septicaemia, or other invasive disease — with orbital cellulitis and septic arthritis given as examples. In other words, it was possible to be counted as a confirmed case in a “meningitis outbreak” without having meningitis at all. Nobody reading the terrifying headlines would have understood that. Probable cases included symptomatic contacts who had not yet had the relevant strain isolated from a sterile site. While these definitions may be epidemiologically defensible for surveillance purposes, their conflation with “meningitis” in public messaging shows a potential for inflating the numbers. Whether or not this occurred we cannot know.
Important public health messaging or Fear propaganda?
The more cynical have pointed out that this outbreak occurred only a few months after Exercise Pegasus, a national pandemic simulation exercise involving a mythical enterovirus with potential to cause meningitis especially in children. The table-top exercise included closing schools and enhanced public health messaging. Readers will remember that Event 201 in October 2019, was a simulation for a coronavirus pandemic which was then played out in real time only 4 months later.
Looking at students queuing up in the open air wearing face masks, suggests that the fear induced during the covid era is easily re-awakened.
On 25th March 2026, just as the Kent cluster fizzled out, the WHO published a statement which said they were following events in the UK closely, ready to help if needed. The statement also said, “Current WHO recommendations for meningococcal vaccination relate specifically to sub-Saharan Africa, where the burden of disease caused by these bacteria is highest. Global recommendations are expected in the coming year.”… “Through “Defeating meningitis by 2030: a global road map”, WHO and partners aim to eliminate bacterial meningitis epidemics, reduce cases and deaths from vaccine-preventable meningitis, and reduce disability and improve the quality of life after meningitis.
WHO/Europe is holding a workshop on 28–29 April 2026 to review progress in implementing the roadmap in the WHO European Region.”
Meanwhile, ‘vaccine hesitancy’ is listed by the WHO as a major risk to global health. Lo and behold, after the much-publicised Kent outbreak there has been a surge in demand across the country for routine MenACWY vaccines amongst teenagers who had missed theirs.
Conclusion
The Kent meningococcal outbreak has followed the usual pattern of clusters though possibly with a more rapid spread than in previous outbreaks. It is easy to be cynical and see the scary headlines as part of a pattern of Fear Propaganda. At the same time we risk ‘throwing the baby out with the bath water’ if distrust becomes baked in.
So let us recap what actually happened. Two young people tragically died of invasive meningococcal disease in one city – something that would be expected by chance roughly every five years. Several more were counted as “cases” even when they did not have meningitis. Thousands were vaccinated with a product unlikely to have had any impact on containment given the outbreak had already peaked. And tens of thousands of healthy teenagers and young adults were given a fluoroquinolone antibiotic carrying a government safety warning, with no public discussion of informed consent. The WHO weighed in. The Health Secretary described it as unprecedented. The New York Post asked whether it might spread to America. This is “public health” in 2026.
Having said that, and despite the Covid vaccine debacle leading me to seriously question the multiplicity of vaccines now given routinely (I wrote about this for HART several years ago), if there is one vaccine that as a retired paediatrician I would probably still recommend, it would be the meningococcal vaccines.
