

Two doses enough to see changes one year later
HART has previously published how repeated mRNA dosing led to change in antibody types from those that defend against viruses (IgG1 & IgG3) to a different type, IgG4, that instructs the immune system to ignore an antigen. Virus is consequently treated like food or pollen – still considered foreign but with no immune response is mounted. In adults this was first noted several months after the second dose in about half the subjects but a third dose of mRNA led to this class switching in the majority of people studied. This has the potential to make vaccine recipients more susceptible to SARS-CoV-2 infection rather than less, a possibility borne out by studies such as the large Cleveland study in which the greater the number of vaccine doses, the higher the rates of infection. But also even more worrying, could this be linked to potential increase in cancers?
Now, a new study of primary school children given only two doses has shown that IgG4 levels climbed significantly a year after the second dose. The study was small, only involving 14 children and there is an urgent need for a larger study to see if the results are replicated. But as the authors say in the abstract, “Understanding mRNA vaccine–specific IgG4 responses in all age groups is crucial as more mRNA vaccines will reach licensure in the coming years.” Note the assumption that mRNA vaccines will reach licensure, which implies licences will be granted regardless of the state of knowledge on these important immunological questions.
The paper, from Hamburg in Germany, opens with the usual magic words required for publication, “The new technology of mRNA-based vaccination proved to be one of the most important tools to fight the SARS-CoV-2 pandemic, allowing safe and effective mass vaccination, saving millions of lives and opening the possibility of developing wide-ranging future therapeutics.”
But they do then go on to say, “Meanwhile, some features induced by mRNA vaccination still need further investigation, among these the unusual induction of immunoglobulin (Ig) G4 antibodies.”
The group studied 14 children with bloods taken at baseline prior to two 10 mcg doses of the paediatric PfizerBioNTech mRNA vaccine, 28 days apart and then repeat bloods 5 weeks and 1 year after the second dose. The results showed “The children’s antibody response 5 weeks after the second BNT162b2 vaccination was dominated by the IgG1 and IgG3 subclasses, which subsequently decreased over time. By contrast, IgG2 and IgG4 levels were relatively low at week 5 after the second vaccination and increased in frequency until the late follow-up”. The results are clearly shown in the figure below, with 9 of the 14 children having higher levels of IgG4 at a year than was found 5 weeks post vaccination.
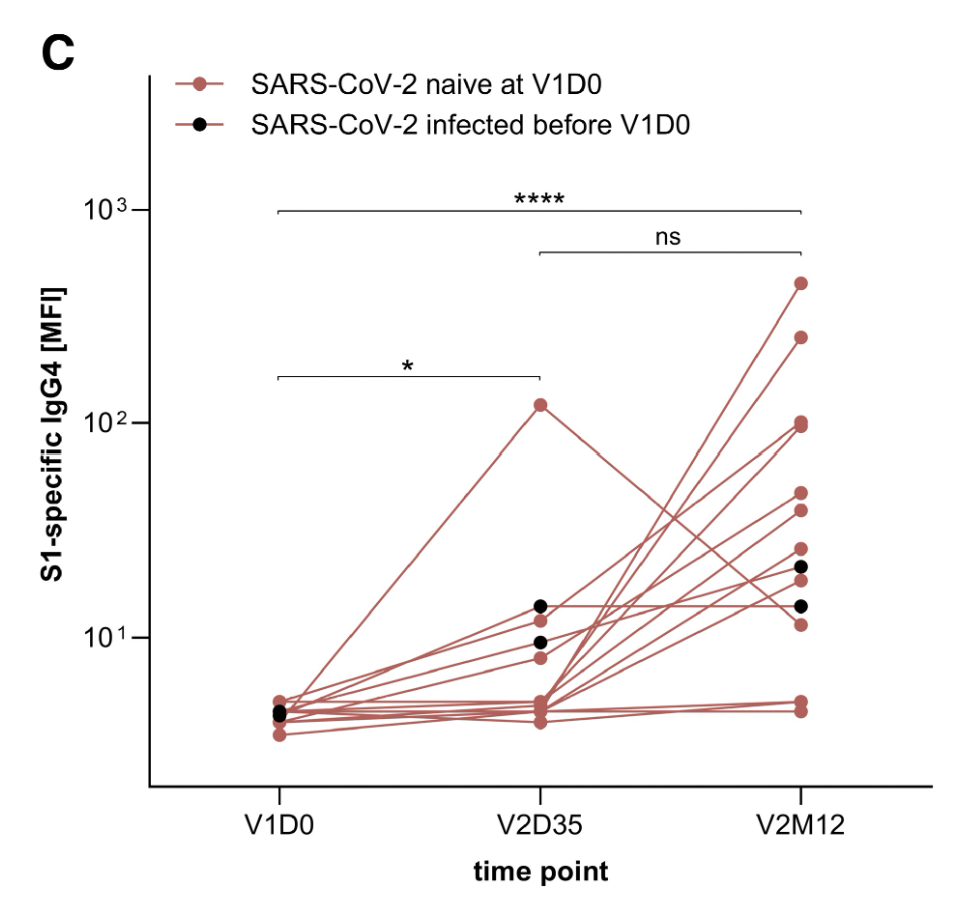
Figure 1: IgG4 to S1 region of spike protein. Measurements taken at dose 1 (V1D0), five weeks after dose 2 (V2D35) and a year after dose 2 (V2M12). Each child’s results are connected with lines and the black dots represent those who had a prior infection. Note the logarithmic scale with each point on the y axis being ten times greater than the previous point.
The authors say, “It remains unclear how the specific subclass kinetics with delayed IgG2 and IgG4 induction by mRNA vaccination, here first described in children, affects long-term immunity.” and it is noteworthy that all 14 of them were infected with SARS-CoV-2 omicron variant during the year post vaccination, which for any previous vaccine would have spelled zero efficacy. “Ah but,” I hear you say, “think how much sicker they would have been”. It certainly debunks any possibility of vaccinating children to protect their grannies.
In conclusion, the authors say, “IgG4 responses should gain more attention in health and disease, especially in the context of mRNA vaccination. Understanding the unusual mechanism triggering IgG4 production is crucial, as more mRNA vaccines are currently under development and could hit the global market soon.” I don’t disagree, but to my mind the primary question which as far as I can see has not been addressed in any of these papers, is not just why there is an IgG class switch but also why antibody levels would still be rising rather than falling so long after the last dose. The one thing they didn’t report was the presence or otherwise of circulating spike protein, and an email to the lead author has as yet received no reply.
Unlike standard vaccines, given at a standard dose, mRNA vaccines stimulate ongoing production of viral protein in unquantified amounts for an unquantified time period. For the unfortunate victims of vaccine-injuries, there seems to be no known ‘OFF’ switch.
