Why did the hospital fatality rate change?
There is something rather odd about the fatality rate for covid in hospitals. NHS England have published data on covid deaths and hospitalisations (which includes both admissions and diagnoses of inpatients). A ten day lag allows for covid deaths to be predicted from hospitalisations. It is quite right to point out that there may be inaccuracy in both the covid hospitalisation and covid death measure using PCR testing but assuming these inaccuracies are constant then the fatality rate should also be constant.
From May to October 2020 and from March 2021 onwards the hospital fatality rate was a predictable 11.5%. (The limited data available before then does not fit because testing was more targetted). Omicron not only led to fewer hospitalisations per case but also had fewer deaths per hospitalisation at 8.5%. Using 11.5% as the pre-omicron rate and 8.5% for omicron (from 1st Jan 2022), we can plot the expected hospital deaths against actual deaths and we see there was a problem.
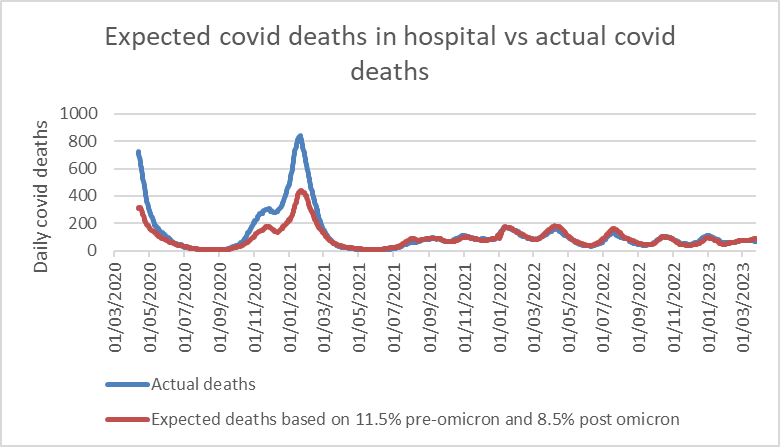
Figure 1: Hospital covid deaths predicted based on covid hospitalisations plotted against recorded covid deaths
For the whole omicron period there is a constant hospital fatality rate of 8.5%. However, pre-omicron the 11.5% fatality rate is exceeded for five months from April to early May 2020 and from late October 2020 to end February 2021. However, for May to October 2020 and March to December 2021, a total of 16 months, the hospital fatality rate was constant.
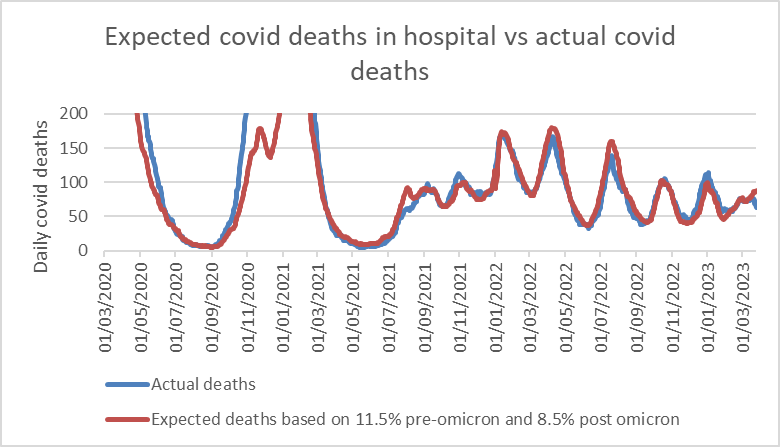
Figure 2: Zoomed in y-axis for figure 1. Hospital covid deaths predicted based on covid hospitalisations plotted against recorded covid deaths
Using a rate of 8.4% throughout means the pre-omicron era does not fit actual deaths as well.
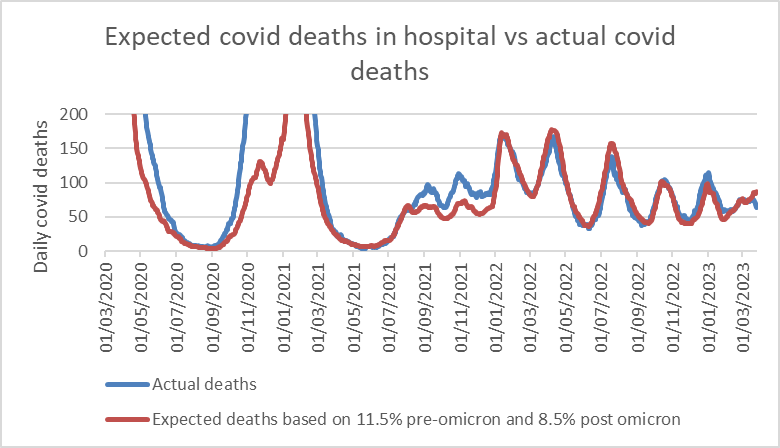
Figure 3: Zoomed in y-axis for figure 1 using a hospital fatality rate of 8.4% throughout
It is notable that the discrepancies in 2020 and 2021 occurred when hospitalisations exceeded 1,000 per day. There are a number of possible reasons for this. Firstly, the high fatality rate in April 2020 may have been partly from having a lower number described as covid hospitalisations compared to later on when testing was ubiquitous. However, the later differences were not due to reduced testing. Was that the level at which intensive care started to be rationed? Did staff absences impact on mortality at that point? Were end of life medications given out more readily when hospital staff were fearing the impact of the next doubling in admission numbers? Perhaps it was also a case of overdiagnosis. Testing was carried out in such a way that a single viral aerosol picked up in the airway of someone who was immune to covid would result in a positive test result and them being described as a covid hospitalisation. The levels of virus in hospital air would have been higher when there were 1,000 or more admissions per day. The dying are particularly at risk for such overdiagnosis and 47% of people dying of any cause test positive for respiratory viruses. Overdiagnosis of covid death was certainly an issue in the first covid winter with deaths from other causes below expected levels in England.
What is perhaps even more notable is that when admissions with omicron exceeded 1,000 per day there was no such impact. Were doctors more careful with their covid death diagnoses, more restrained with end of life medication, less panicked about intensive care pressures?
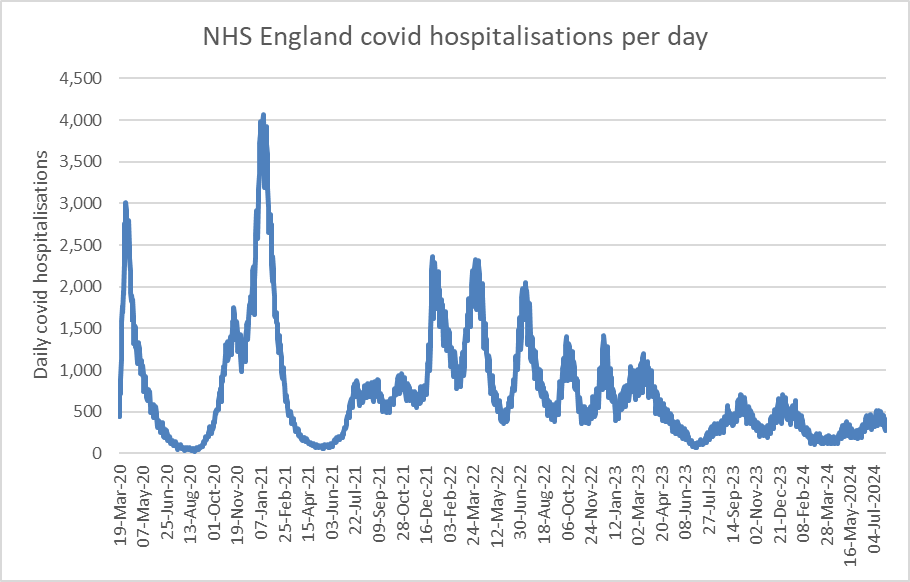
Figure 4: Covid hospitalisations per day which have been published up to July 2024 unlike the hospital covid death data which ended in March 2023.
Comparing the hospital fatality rate in May-October 2020 with the same months in 2021 shows a constant hospital fatality rate of 11.5% indicating no impact of vaccination on this rate. This is in stark contrast to the arrival of omicron when the hospital fatality rate fell by 26%.
The vaccine did not reduce the hospital fatality rate.
The Scottish Inquiry continues to expose the reasons for the higher hospital fatality rate during the waves of fear yet it is being studiously ignored.
