

How much do we really know about safety?
There are gaps in our knowledge about the risk from covid infection in pregnancy but even larger gaps regarding the risks of vaccination. What we do know, however, is that there have always been very good reasons to be cautious of giving medication in pregnancy.
How risky is SARS-CoV-2 infection during pregnancy?
Early in the pandemic, the fear was raised that Covid-19 was more severe during pregnancy. This would not be surprising, as that is true for any infection. There are several reasons for this. The immune system is relatively down-regulated in pregnancy (vital so that the mother does not reject the developing fetus which of course is 50% genetically ‘non-self’) making women more susceptible to infections. It is known that some viral infections, such as rubella and cytomegalovirus cause fetal abnormalities if caught early in pregnancy. In late pregnancy, respiratory infections are likely to be more problematic, as the diaphragm may be splinted by the growing uterus, making breathing shallower. Also any febrile illness may tip the mother into preterm labour. And finally there was the concern that passage of the virus across the placenta could infect the baby, as may be seen in untreated HIV infection.
Thus, there were good theoretical reasons to be concerned. On the other hand, Covid-19 severity was known to be highly related to older age groups and serious comorbidities whereas the majority of pregnant women will be young and healthy. In all, nine pregnant women died with Covid-19 between March and December 2020 from a total of 683,191 births that year. SARS-CoV-2 infections with the recent omicron variants are known to be much milder, including during pregnancy.
One problem with quantifying the risk of Covdi-19 in pregnancy arises from the routine testing – thus anyone admitted for obstetric reasons was tested and so hospitalisations in pregnancy will have all been counted as pregnant covid admissions where in reality many were admissions for pregnancy complications at a time of high SARS-CoV-2 prevalence.
Finally, the evidence that vaccination has reduced risk from covid in pregnant women is lacking.
What do we know about covid vaccine safety in pregnancy?
The honest answer to this is ‘very little’. All the randomised clinical trials have specifically excluded pregnant women. Indeed, participants in the trials had to affirm that they were not trying to become pregnant and that if sexually active they would take contraceptive precautions. These rules were also applied to potential fathers and an obligation to inform the trial investigators should pregnancy occur. Invariably, some participants in the trials did become pregnant but full information on the outcomes is not available.
It was known that Pfizer’s animal studies showed the lipid nanoparticles were detectable in the ovaries (see Table 4-2). Moreover, SARS-CoV-2 spike glycoprotein was found to share similarities with 27 human proteins that relate to egg production (oogenesis), uterine receptivity and placentation. It is also known that the pregnancy studies in rats involved a higher rate of pregnancy losses and fetal anomalies in the vaccine than the placebo arm, despite which, these limited studies were reported as showing no concerns. See this analysis of recently released Pfizer data.
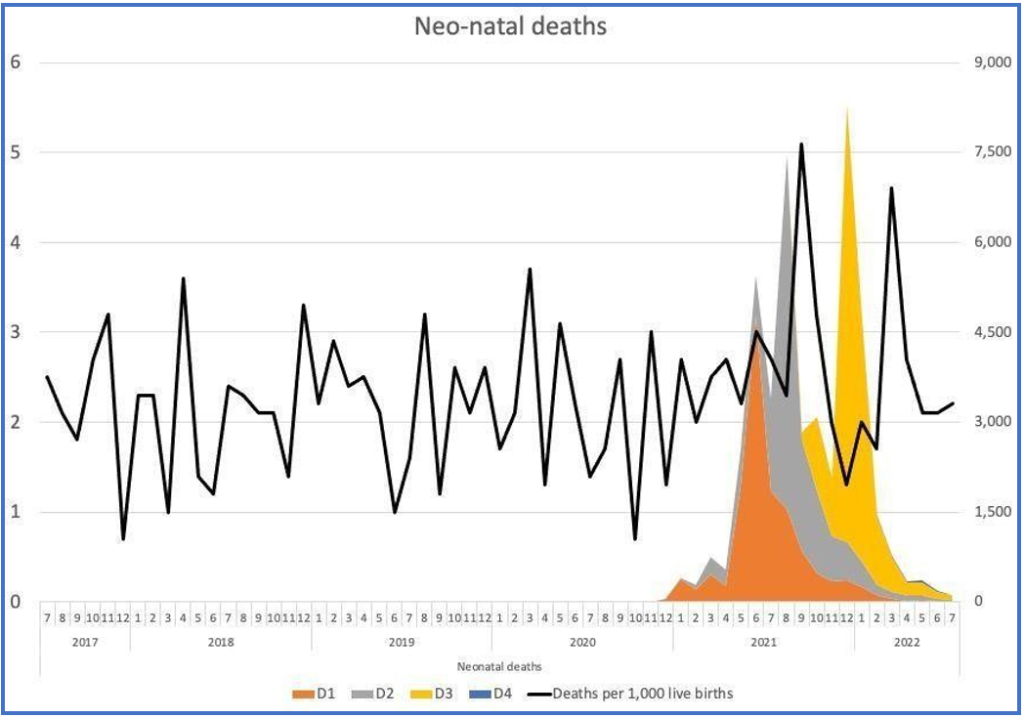
A detailed open letter to the president of the RCOG highlights the lack of information and some worrying signals of potential harm. One such signal is the increase in neonatal deaths in Scotland. It has already been concluded that these deaths were not related to Covid-19 itself but, like the excess deaths in the whole population, the officials and the MSM are ‘baffled’. Oddly, no-one has looked at the effect of vaccination beyond 28 days. Public Health Scotland declared there was no “plausible link” to vaccination to justify investigation, adding, “the outcomes of such analysis, whilst being uninformative for public health decision making, had the potential to be used to harm vaccine confidence at this critical time.” Indeed, Professor Sarah Stock, expert in maternal and fetal medicine at the University of Edinburgh, commented in May 2022: “The numbers are really troubling, and I don’t think we know the reasons why yet” but “stressed the Covid vaccine, which studies have consistently shown to be safe in pregnancy, was not a factor”. Professor Richard Ennos, also from Edinburgh University, has written challenging her logic.
An inquiry has been launched in September 2022, but is likely to take 6-9 months – the temporal link to the vaccines would at least suggest a much more urgent need for investigation.
It is not only in the UK that concerns have been raised. Australia has had an extraordinary fall in live birth rate in the last two months of 2021 (2022 figures are not yet available). The results are so extreme that it must surely be some sort of reporting error. But Germany and Sweden have also seen a sharp drop in fertility rates in recent months which have been analysed here, looking a Covid-19 infections, unemployment rates and vaccination rates.
A hugely concerning peer-reviewed preprint has been published showing reduction in stem-cells from umbilical cord samples after Covid-19 infection but much more marked effects following vaccination. The paper has been reviewed here. These cells are an integral part of the newborn infants developing immune system.
Historical pharmaceutical catastrophes and cautions
The most widely known example of severe harm resulting from a drug used in pregnancy is Thalidomide. Launched in 1953 as a tranquiliser, the drug company was taken over the following year and it was relaunched in 1958 as an anti-sickness medication, despite undergoing no specific testing in pregnancy. Over the next 3 years, over 10,000 babies were born with severe limb defects and some also deaf or blind and many thousands are thought to have died. Women had trusted the authorities that all safety checks had been carried out, but sadly irreversible and catastrophic harm resulted before the drug was eventually withdrawn. It was the Thalidomide scandal which led to the setting up of the UK Yellow Card system.
The prescribing of diethylstilbestrol to pregnant women resulted in harm to female fetuses, which only became apparent when the exposed girls themselves reached adulthood. It took 30 years before the late cancer risks were fully recognised and the use of diethylstilboestrol in pregnancy was stopped. Similarly, sodium valproate, an effective anticonvulsant, when given in pregnancy can cause ‘fetal valproate syndrome’, with severe effects on cognitive function. Its teratogenic potential was known from animal studies prior to its launch in 1972, yet even as recently as 2020, women were still not fully informed. It is noteworthy that a BMJ letter in 1981 sounding caution came from a group in Finland – the same country who first noted narcolepsy in children following Pandemrix vaccination. The shortcomings of our healthcare system, described as “disjointed, siloed, unresponsive and defensive” are evident in the Cumberlege Review published July 2020 – ‘First Do No Harm’.
It is against this background that the British National Formulary has strict cautions on prescribing in pregnancy, stating:
“Drugs can have harmful effects on the embryo or fetus at any time during pregnancy. …Drugs should be prescribed in pregnancy only if the expected benefit to the mother is thought to be greater than the risk to the fetus, and all drugs should be avoided if possible during the first trimester. During the second and third trimesters drugs can affect the growth or functional development of the fetus, or they can have toxic effects on fetal tissues.”
“Not all the damaging effects of intrauterine exposure to drugs are obvious at birth, some may only manifest later in life. Such late-onset effects include malignancy, e.g. adenocarcinoma of the vagina after puberty in females exposed to diethylstilbestrol in the womb, and adverse effects on intellectual, social, and functional development.”
Most vitally the BNF reminds us, “Absence of information does not imply safety.”
We can only hope that in the case of the Covid-19 vaccines, this does not turn out to be prophetic.
