HPV vaccine strategy part 3
see also: part 1 HPV Vaccine Efficacy and Part 2 HPV Vaccine Safety
Global Elimination: the WHO Pledge
The World Health Organization (WHO) has launched a global strategy initiative to eliminate cervical cancer: it proposes a vision of a world where cervical cancer is eliminated as a public health problem; its ambitious target, to be met by 2030, is for countries to be on the path towards cervical cancer elimination. This target, called 90–70–90, relates to 90% of girls fully vaccinated with HPV vaccine by the age of 15 years (before sexual activity); 70% of women screened with a high-performance test from 35 to 45 years of age to identify any cell changes; and 90% of women identified with precancerous cervical disease or invasive disease to receive appropriate treatment.
Cervical cancer control
In a recent presentation by Professor Jo Waller (Cancer Behavioural Science Centre, Queen Mary University of London), she discussed the use of behavioural science in diagnosis and prevention of cervical cancer control focusing on both vaccination and screening. She provided background statistics on the global burden of cervical cancer disease – estimated in 2022 to be 660,000 new cases and 350,000 deaths globally. The greatest disease burden is in sub-Saharan Africa and parts of Asia. The proposed aetiology of cervical cancer is via infection with Human Papilloma Virus (HPV), the putative causal agent that is sexually transmitted. Usually the immune system clears any problems, but when infection persists, it can cause cellular abnormalities and precancerous lesions that can ultimately progress to cancer. Prevention approaches include HPV vaccination to stop infection, and cervical screening to detect the presence of HPV and precancerous cellular abnormalities, as discussed fully in the first of this series of articles.
Reasons for falling HPV vaccine coverage
Reasons for falling HPV vaccine uptake partly relates to lockdowns. During lockdown vaccine uptake was low because it relied on a school-based approach. Other reasons are resources and staffing, school absenteeism, consent processes, vaccine hesitancy and the change to a one-dose schedule, which although more convenient, if a dose is missed the opportunity to catch up is more challenging. Professor Waller noted that there has been an increase in vaccine hesitancy, globally. On the topic of vaccine hesitancy, she discussed misinformation related to “conspiracist ideation” with vaccine hesitancy reasons linked to “attitude roots”. She listed as examples: “Big Pharma, government cover-up, population control, targeting marginalised groups, made-up threats, vaccination is unnecessary, the disease is not serious, misperception of risk, and vaccination is not for me”. Professor Waller developed and promoted the JITSUVAX empathetic refutational interview (ERI) to improve vaccine conversations offering tips on how to refute the vaccine hesitant beliefs. Many health-care workers find it challenging to discuss and recommend vaccination with people who have concerns about vaccines. The ERI is an evidence-based, four-step method she helped to develop to equip health workers with skills to ‘navigate’ those conversations. Techniques include how to build trust and address misinformation while maintaining rapport, and the importance of the role of healthcare professionals to ‘target’ information to address ‘knowledge gaps’ to promote HPV vaccine confidence within the general population. The aim, apparently, is to empower people to make their own choices about vaccination from the ‘best’ information.
There are many reasons for falling HPV uptake. Japan, for example, saw several legal cases launched in 2013 (not mentioned in Professor Waller’s talk) owing to the halting of clinical trials of the vaccine because so many harms were caused.
Social Ecological Model
As a health psychologist and behavioural scientist, Professor Waller described the multiple levels of influence on behaviour directed to increase screening and vaccination uptake. These include interpersonal (targeting an individual’s knowledge, skills and personal motivations) social, institutional (the rules and regulations of organizations), community (resources that promote social norms) and policy (local, state and federal policies).
She presented the ‘behaviour change wheel’, designed in 2011 by Michie et al as a framework to improve behaviour change interventions. Motivation, capability and opportunity are at the centre of the wheel, driving sources of behaviour. At the next level are the functions of interventions, which include education, persuasion, incentivisation, coercion, training, enablement, modelling, environmental restructuring, and restrictions! The outer layer of the wheel are components of the overarching policy, namely: guidelines, environmental/social planning, communication/marketing, legislation, service provision, regulation, and fiscal measures. Influencing behavioural outcomes is achieved with social motivations to produce behavioural changes through education and training, which links to policies.
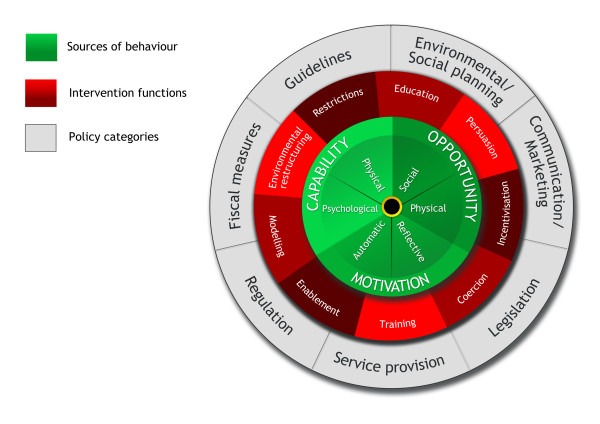
Figure 1. The Behaviour Change Wheel
Tackling ‘Misinformation’
A paper published by Janne Bigaard and Silvia Franceschi in Molecular Oncology on HPV vaccination showed how coverage can be boosted via tackling ‘misinformation’. In Japan, and Ireland, approaches have been used to increase HPV vaccination uptake, which include parent-centred interventions, provider-centred interventions with communication and recommendation approaches. Practice-centred and health-care settings included reminders, prompts, access programmes (vaccination in schools), performance feedback and navigators. Other mechanisms included targeting parents as well as providers, such as paediatricians, as noted in a paper on interventions to improve HPV vaccination uptake. Parents can be “targeted at the knowledge, attitudes, beliefs, and support levels.” Provider level influence through knowledge, recommendations and communications has been successful. At the practice level, vaccine access, reminder/recall systems, peer/patient navigators, and provider-targeted strategies are used. Broadly, this entails education and training programmes, performance feedback, vaccine messaging, prompt systems, and vaccine bundling. Uptake of HPV vaccines ‘targeted’ at parents is higher when this vaccination is ‘bundled’ or given with other immunisations offered at the same age – usually in schools often without parental consent and making use of ‘Gillick competence’.
In 2025, the screening intervals for 25–49 year olds were extended from 3 years to 5 years. From this year, the following will be introduced: self-sampling for non-attendees and removal of every 3-year sampling for vaccinated cohorts. Finally, digital invitations will be introduced, with an important contribution of behavioural science, such as explaining acceptability of new innovations and programme changes, developing communication strategies to facilitate “informed choice” and increased participation, as well as mitigating adverse psychological impact of a positive screen result.
Interestingly, a recent study from the US has looked at giving HPV vaccine earlier, at age 9-10 years ie two years earlier than current recommendations. It appeared parents were receptive to the idea and the authors noted that “discussions at ages 9–10 years were shorter because sexual activity was not perceived as salient.” This might be considered the opposite of informed consent, give it to the children without any tricky discussions over what it is for. Such a strategy might increase uptake but at the cost of efficacy, since the vaccine would be waning further at the time of onset of sexual activity.
Elephant in the Room: No Informed Consent
The glaringly obvious issue with the use of behavioural science in persuading adults and adolescents alike to be HPV vaccinated is the impact on informed consent. The HART team has written about this on numerous occasions with regard to covid vaccines. Just recently, Gary Sidley has provided an excellent piece that complements this article, in highlighting how informed consent and the ‘first do no harm’ principles have been trampled on by healthcare policies and by most professions, including doctors, nurses and psychologists. He explains the mismatch between the ethics code and healthcare activity, and how the erosion of the code of ethics was all too apparent during the covid era. Effective practice should involve 1. doing no harm, 2. gaining informed consent, and 3. raising awareness if wrongdoing is witnessed. Sadly, these principles were abandoned during the covid pandemic, and seemingly extend to a lack of ethics surrounding the HPV vaccine. The WHO also states that if a parent does not wish to have their child vaccinated, they should keep their child off school on a vaccination day. This highlights how the behavioural science to increase uptake of these vaccines is so pervasive and includes breaching medical privacy.
Behavioural Science in Public Health
The overall message from Professor Waller’s presentation has several concerns.
- First, the behavioural scientists seem to consider it acceptable for coercion – or rather undue influence, and the use of psychological tactics to ‘educate’ or influence young girls and women to take a so-called preventative vaccine and to undergo invasive screening.
- Second, the hugely ambitious goals of the WHO 90–70–90 target by 2030 indicate the extent to which vaccine coverage and screening uptake is being prioritized, and in a very short 5-year timeframe.
- Third, the framing of vaccine hesitancy as being ‘conspiracy-theory’ based and that the concerns of parents whose children have been injured has ‘no scientific basis’ and is presented as lacking in credibility, is a highly dismissive stance in light of the past 5-years of vaccine tyranny we have observed during the Covid era.
- Fourth, that behavioural science has been used for decades and is a well-orchestrated approach used by the healthcare industry to encourage ‘uptake’ of a so-called preventative therapy – in this case prevention of HPV infection and, by extension, cervical cancer (despite the high natural clearance rate).
- Fifth, there is a concerted and well-coordinated programme used to influence girls, adolescents and women to undergo screening and vaccination at a young age and throughout both fertile and non-fertile age groups.
- Sixth, if the vaccine was having any tangible benefit in preventing cervical cancer, one might think that screening would be unnecessary in any woman who had been vaccinated against the ‘viral pathogen’.
- Finally, it is clear there is a priority effort to discredit any views that do not adhere to those that fully support HPV vaccine and screening programmes or to obscure views that cannot be ‘controlled’.
Lessons Learned
Clearly, most prevention and public healthcare professionals have gleaned little from the Covid debacle. Many in the public are now aware of vaccine injuries disclosed through pharmacovigilance records (such as the UK Yellow Card Report System, or the VAERS system in the USA) and other alternative media outlets. Moreover, that covid-vaccine injuries and deaths since the rollout of covid injections have dwarfed the combined vaccine injury and death data captured on VAERS in the past 30 years combined – is a testament to how unsafe the covid injections are. This factual inconvenience has done little to quash the cognitive dissonance of academics and vaccine promoters, who prefer to disregard the possibility that any vaccines may cause more harm than benefit. The fact that behavioural scientists openly admit and seemingly promote the use of coercion as a means to influence vaccine uptake is alarming. So much for the principles of informed consent. The notion of voluntary participation of the individual to receive an experimental or an approved therapeutic when they are at minimal risk of being harmed by any purported pathogen, illustrates how ‘bodily autonomy’ principles are waning. The lack of full safety data provided to parents and adolescents alike when weighing the risk/benefit of taking such vaccines, is a stark illustration of how ineffective our healthcare governance policies have become.
Vaccine Scepticism
It is interesting that HPV vaccine coverage in some countries (such as Japan) – even before Covid – was low owing to concerns of the health harms caused by HPV vaccines and which have not demonstrated an irrefutable effect on the prevention of cervical cancer. Vaccine uptake rates rose following certain public health prevention approaches, illustrating that behavioural science is a powerful tool in shaping societal ‘norms’ and pressures to undergo an intervention or screening. As noted, when the public opinion is backed up with survey evidence, it is interesting to consider how the Covid pandemic might have unwittingly damaged the trust of the public for cancer vaccines and screening. So embedded is the public health screening and vaccination programme for HPV and cervical cancer, that there was an uproar when screening intervals changed from every 3 years to every 5 years.
Vaccine uptake is dwindling, not just for Covid, but also for HPV and other vaccines, in light of a multitude of health harms and adverse effects resulting from their administration. Recently, the HART team chronicled the growing skepticism among the general public. A UK survey showed that 37% of respondents have an increasing mistrust in politicians, especially in relation to the Covid pandemic and vaccines. In a survey when people were asked “If there was another pandemic on the same scale as Covid, how likely would you be to follow government instructions to isolate?”, the results were revealing: 28% said they would be unlikely to do so. 37% thought it was ‘probably or definitely true’ that the government exaggerated the pandemic to control people. This shows how the public are seeing through the veil of mainstream noise and are beginning to mistrust and question (rightly so) the very organisations that are orchestrating these top-down control approaches. The likelihood then of achieving the WHO’s 90–70–90 goal, could begin to look shaky. Furthermore, the strident vaccination and screening programmes for HPV-related cervical cancer, as well as mRNA Covid vaccines and now cancer gene-based therapies, completely ignore the precautionary principle. This emphasizes caution, pausing to reflect and reviewing evidence before rolling out new innovations that could prove disastrous.
Campaign group UsforThem undertook a parental survey in 2023, which revealed:
- Only half the public (52%), and just 40% of 18-35 year olds, think the Government was honest about the risks and benefits of Covid vaccination.
- Just 60% of parents of children under 18 say they would now be likely to give their child vaccines recommended by the Government (down from 84% having said that they would have done so prior to the pandemic).
Conclusion
We have witnessed the global rollout of Covid-19 vaccines, and many other injections that have been hastily approved with poor or non-existent adequately conducted randomised clinical trial data. Behavioural science has been at the helm to enable policy development and to maximise acceptability and uptake of vaccination and screening rollout. It highlights a broader appreciation of the facilitators of vaccine uptake and how this ‘science’ has been used to optimise and change uptake and behaviour. Questioning the safety or efficacy of covid-19 shots led to the ‘anti-vaxxer’ label and refusal to discuss. It is scant wonder that scepticism has increased. Since behavioural science has been such a powerful tool to help produce a ‘compliant’ society and to discredit and silence any ‘sceptics’, it has arguably helped to enhance disastrous narratives during the pandemic preparedness arena.
The question we should ask is: is there a place for behavioural science in society?
