

Government response to folic acid petition
Dr Clare Craig
There have been two parliamentary petitions regarding folic acid. Both have received a response.
- The first petition asked for folic acid to be kept out of wholemeal flour
- The second petition asks for an end to mandatory fortification and can still be signed here.
The NHS advises many people to avoid folic acid. The government claims people can avoid it if they need to. That claim is provably untrue and the adverse effects of medicating the whole population have clearly not been considered or addressed.
The responses are almost identical and do not properly address the issues raised. Parliamentary petitions are supposed to receive considered responses. Instead, both petitions received largely generic policy statements which are almost identical and failed to answer the questions being asked.
The first petition & response
The first petition was asking to:
- Ensure at least one non-wholemeal flour remains unfortified.
- Exempt organic flour from mandatory fortification.
Here is the first response – it never addresses the central request of the petition.
This is what they said:
“The Government is mandating folic acid fortification to reduce neural tube defects. The policy applies to non-wholemeal flour, reflecting the existing flour-type already subject to fortification.”
One sentence in and they clearly decided to pretend to not understand the petition. The petitioners know what the policy applied to and were asking that any flour to which the policy did not or should not apply, must remain folic acid free.
It goes on to say:
“Not fortifying wider than the type of flour that is presently fortified, means that individuals can avoid fortified flour if they choose to or need to. This includes wholemeal flour, gluten-free products and other flour types such as soya or spelt flour.”
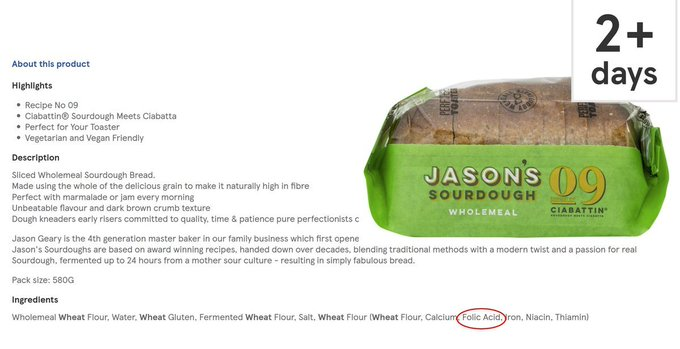
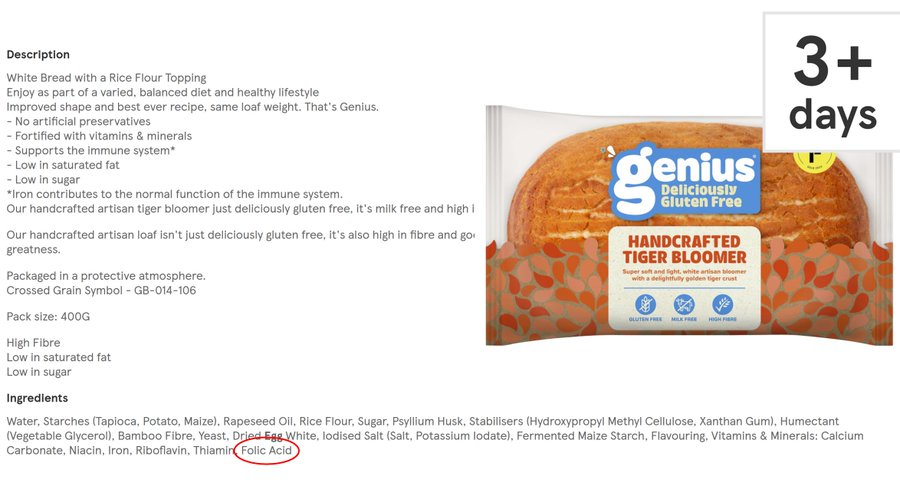
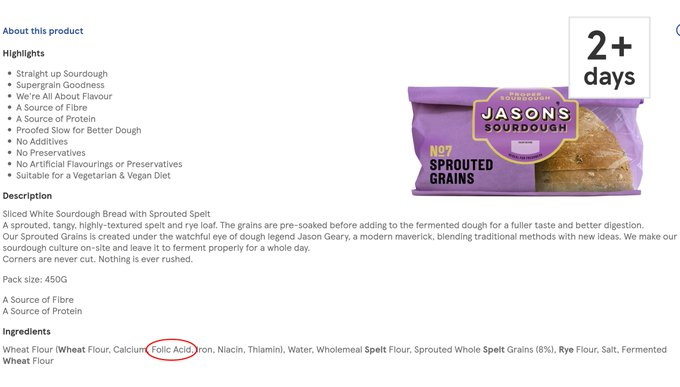
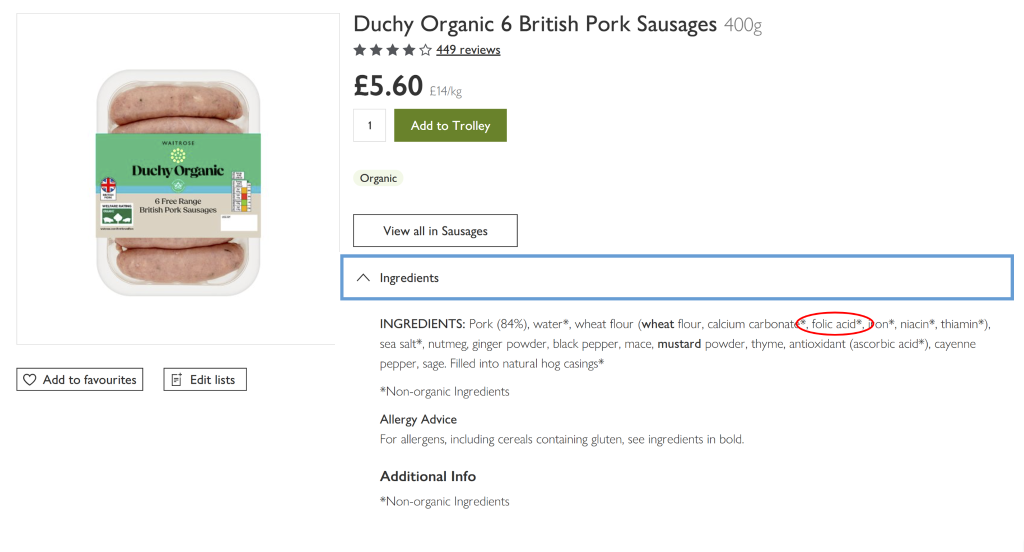
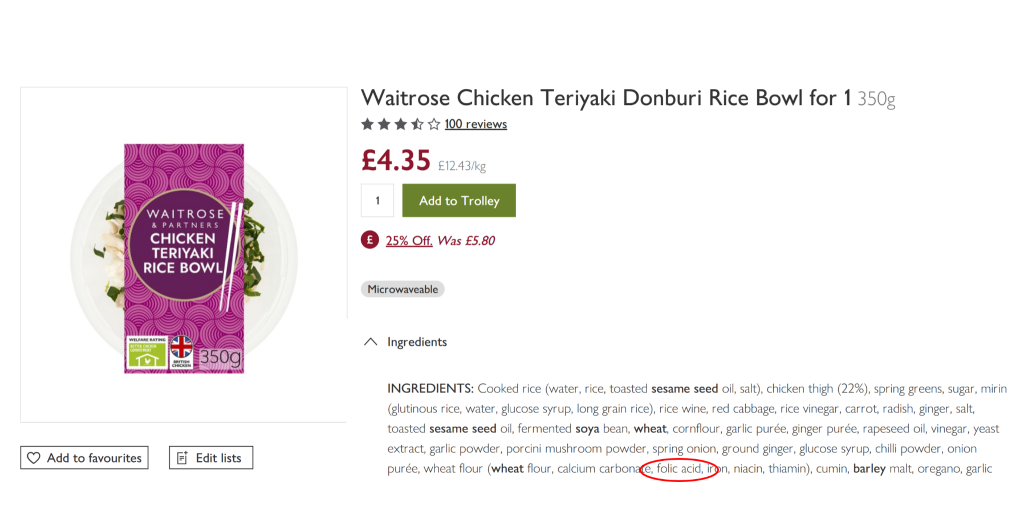
The whole point of the petition is that this is not true! These products are already being fortified because they failed to legislate to prevent it. Here are some examples of how individuals cannot “avoid fortified flour if they choose to or need to” by selecting such products:
Wholemeal bread:
Gluten free bread:
Spelt bread:
Further down they say:
“Fortifying at higher levels would allow for greater reductions in NTDs but this level was chosen to balance public health benefits with safety.”
This is an admission that safety considerations influenced the chosen dose.
The remainder of the reply is them justifying their policy, the dose chosen, the modelling done. It totally fails to address the two simple questions. But there is no come-back. The petition did not reach 100,000. Therefore it did not trigger the parliamentary debate that has never been held on this topic.
It ends by saying:
“Limiting mandatory fortification to non-wholemeal wheat flour helps preserve choice by maintaining the availability of unfortified wholemeal and non-wheat flours.”
This is just adding insult to injury. It is galling to claim that they have maintained “the availability of unfortified wholemeal and non-wheat flour products” when 24,000 people were asking them to please ensure they do just that because they have failed to do so.
The second petition & response
The second, and active petition, asking to end the fortification in all flour has also been responded to.
It begins:
“Folic acid fortification is an evidenced public health measure, not a medical intervention.”
Folic acid is a synthetic compound added specifically to alter human physiology. Whether one chooses to call that medication or fortification, its purpose is to change the biology of people who consume it. I would call such a product a drug. It behaves in every way like a drug not a food. When given to a whole population every single person’s body is changed by it. That does not happen if you increase the uptake of a type of food or a vitamin. It is a medical intervention. It is mass medication of the entire population.
“The policy applies to non-wholemeal flour, reflecting the flour-type already subject to fortification. The mandate does apply to non-wholemeal flour including brown flour, white flour, imported flour and organic flour. The UK Government is mandating fortification of non-wholemeal wheat flour with folic acid with the primary objective to increase folic acid intake among women of childbearing age, thereby improving blood folate levels and reducing the risk of neural tube defects (NTDs) during pregnancy. The policy is projected to prevent around 200 NTD-affected pregnancies annually—approximately 20 per cent of UK cases.”
We’ve already covered the failure to protect non-wholemeal flour from contamination. They are open about the aim. The reality is that their modelling predicting prevention of 200 affected births is based on two pieces of incorrect data. First, the clinical trial where 9 babies died (mostly miscarriages) for every “prevented” neural tube defect with the researchers who ran the trial suggesting that the affected babies were killed. Secondly, the CDC data claiming a benefit after rollout in the USA saw a reduction in affected live births during a period of improving ultrasound diagnostics but once terminations are factored back in there was no change.
“The population-level policy will have the wider benefit of increasing the intake of folic acid and improving folate status across the whole population.”
The first claimed benefit is “increasing the intake of folic acid.” That logic could be used to justify adding absolutely anything to flour. That is a direct consequence not a benefit. It is circular reasoning.
The second benefit “improving folate status across the whole population” is questionable to say the least. Yes, the evidence shows it will raise folate status across the population – but who says that is an improvement? Folate is essential for DNA synthesis and cell division. This is why there has long been concern that increasing folate availability could accelerate the growth of existing neoplastic lesions and increase the risk of new ones. For example, a small randomised trial found a statistically significant 2.6-fold increase in prostate cancer when men were given a daily 1 mg of folic acid supplement. That is a large dose but a bad diet could easily reach that level:
| Food | Assumption | Folic acid from fortification |
| 2 slices of toast | 60 g flour | 150 µg |
| Tea and biscuits | ~40 g flour | 100 µg |
| Meat pie | Pastry made with 80 g flour | 200 µg |
| Cake | Slice made with ~50 g flour | 125 µg |
| Supermarket pizza | Base made with ~150 g flour | 375 µg |
| Multivitamin | 400 µg | |
| Total | 1,350 µg |
Larger pooled trials have not found a statistically significant increase in prostate cancer but those trials ran for only around five years, and were never designed to detect a cancer that takes decades to develop. The exposure that actually matters here, low-dose intake sustained across a lifetime, has never been tested in a randomised trial and cannot easily be. As always, benefits are much easier to measure than risks.
“Folate, including folic acid””
Now they are trying to claim that the synthetic drug folic acid is part of the family of natural dietary folates. It is not. It is a synthetic chemical. Despite over half a billion years of plant and animal evolution and the vast diversity of plants, animals, fungi and microbes, nature has never adopted folic acid as a biological molecule. Life relies on reduced folates, not folic acid. Folic acid can be converted by the body into usable folate, and therefore can increase folate stores, but the conversion takes hours and for those hours the body is exposed to the unmetabolised synthetic drug circulating in the blood and binding too tightly to folate receptors, blocking normal function.
The full sentence reads:
“Folate, including folic acid, plays an important role in forming healthy red blood cells and maintaining brain health.”
It is true that people with folate deficiency develop a characteristic megaloblastic anaemia and may have impaired cognitive function. Importantly, however, this confuses the pathology of folate deficiency with the effects of exposing an entire population to synthetic folic acid. The evidence that folate deficiency itself causes cognitive impairment is much less certain, and intervention trials with folic acid have generally shown little or no cognitive benefit in adults. Folic acid has not been shown to improve cognitive function in people with dementia, and a systematic review involving more than 22,000 participants found no benefit in overall cognitive function or cognitive ageing from homocysteine-lowering treatment with B vitamins, including folic acid. One trial found modest improvements in some cognitive tests in people with low folate status, but the authors concluded that the evidence was insufficient to recommend folic acid even for people with cognitive decline.
More fundamentally, the Government is again conflating treatment with prevention. People with folate deficiency are already treated with therapeutic doses of folic acid; they do not require additional dietary exposure through mandatory fortification. Nor is there evidence of a reservoir of undiagnosed clinical folate deficiency that would justify medicating the whole population. Indeed, researchers have long commented that folate concentrations are distributed continuously across the population rather than forming a distinct folate-deficient subgroup.
“Previous efforts through public health campaigns to promote supplementation, as well as voluntary fortification by manufacturers, have had limited success. Despite longstanding UK public health advice recommending a daily supplement of 400 micrograms of folic acid before conception and during early pregnancy, uptake remains suboptimal, particularly among younger women and those from lower socio-economic backgrounds. Since almost half of pregnancies in the UK are unplanned, many women may not take supplements during the critical early weeks of gestation.”
The claim that 400 micrograms is needed is based on the flawed study on pregnant women mentioned above and also the rigging of the “recommended daily allowance” in the USA by industry.
“The policy has been carefully designed to be proportionate, targeting non-wholemeal wheat flour because it is widely consumed across the population and is the most effective vehicle for delivering the intended public health benefits.”
Proportionate? Do you think exposing 69 million people to a drug when only 600,000 pregnant women each year have any possibility of benefit is proportionate? For 68.4 million people the risks by definition outweigh the benefit because there is no measurable benefit in terms of outcomes other than a higher folate level to be had.
“This approach is consistent with long-standing UK fortification requirements for wheat flour, including the mandatory addition of calcium, iron, niacin and thiamine, which also apply to non-wholemeal wheat flour produced to organic standards. Not fortifying wider than the type of flour that is presently fortified, means that individuals can avoid fortified flour if they choose to or need to. This includes wholemeal flour, gluten-free products and other flour types such as soya or spelt flour. To ensure people can easily identify products that are suitable for them, added vitamins and minerals, including folic acid, must be labelled in the product’s ingredients list. This must also be declared when fortified flour is used as an ingredient.”
We have covered their pretending to have introduced protections that do not exist for non-wholemeal products above. They then try and justify the decision based on committees and modelling and
“The decision to fortify non-wholemeal wheat flour with folic acid has a long history and has been considered both by the Scientific Advisory Committee on Nutrition (SACN), which advises the four UK governments on nutrition-related matters, and its predecessor, the Committee on Medical Aspects of Food and Nutrition Policy. Folic acid fortification was recommended by the SACN in 2006, after an extensive review of the evidence on folate and health, which is available at the following link: https://www.gov.uk/government/publications/sacn-folate-and-disease-prevention-reportSince then, there have been several further evidence reviews and modelling work (for example: https://www.foodstandards.gov.scot/science-and-evidence/stochastic-modelling-to-estimate-the-potential-impact-of-fortification-of-flour-with-folic-acid-in-the-uk) to establish the level of folic acid to be added to flour, as well as to address concerns about potential adverse effects.”
Note this second admission of “potential adverse effects.”
“The policy has been subject to public consultations, including the 2019 Department of Health and Social Care and devolved governments consultation (available at the following link: https://www.gov.uk/government/consultations/adding-folic-acid-to-flour/outcome/proposal-to-add-folic-acid-to-flour-consultation-response) on the proposal to fortify flour with folic acid (including a question on the effect on small businesses), and the 2022 Department for Environment, Food and Rural Affairs (Defra)-led consultation on the Bread and Flour Regulations.”
Let’s take a look at the response to that consultation when people were asked how fortification should be carried out:
“The baseline option of fortifying non-wholemeal wheat flour with folic acid had support from 9% of participants, similarly the option to fortify all types of flour, including wholemeal and other grains received 9% support. Fewer respondents (3%) were in support of the option to fortify non-wholemeal wheat flour that is only used to make bread. The option to fortify all types of flour, and other non-wheat products, such as gluten-free received 34% support.
Thirty-eight per cent of respondents expressed support for no mandatory fortification of folic acid in the UK. The reasons for this view and the UK and devolved administrations’ responses can be found in the sections on questions 4 and 11 below as well as throughout the document.
Finally, 7% of respondents did not answer the question.”
Thus their consultation found 55% in support of some form of fortification against 38% who wanted no mandatory fortification of folic acid. Only 9% supported the option that they chose: “fortifying non-wholemeal wheat flour with folic acid”. But the supporting information to the consultation gave no information of potential harms from folic acid. A consultation response made in ignorance of the scientific facts should not be used to support this unscientific plan.
They go on to say,
“These consultations allowed members of the public, industry and health professionals to provide feedback and were a key part of policy development. Feedback to the Defra consultation highlighted consumer choice as a key concern. Limiting mandatory fortification to non-wholemeal wheat flour helps preserve choice by maintaining the availability of unfortified wholemeal and non-wheat flours. In addition, the policy does not apply to flour produced by small mills (definition based on their limited production capacity).”
Back to the core issue of lack of choice (let alone informed consent). As well as many wholemeal and gluten free products already having folic acid added since this legislation was passed, there are even small mills which have started adding it to their flour. Even chasing down a small mill to supply flour to make your own bread does not guarantee that you won’t be exposed. For example, Shipton Mill will be adding it to many (but not all) of their flours.
Who should avoid folic acid?
“The NHS provides guidance for individuals who may need to avoid folic acid, for example, due to specific medical conditions or interactions with medication. People in this situation are advised to seek advice from a healthcare professional.”
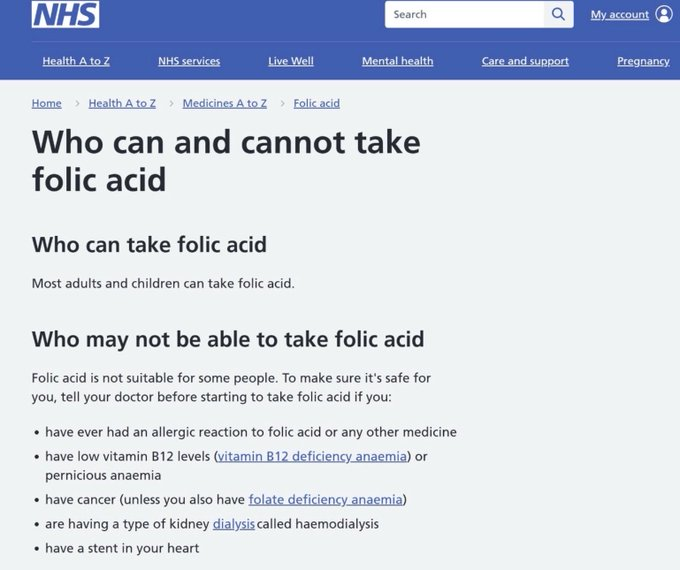
Giving people folic acid when they have undiagnosed pernicious anaemia can lead to severe neurological damage. By definition, these people do not know they have any reason to avoid folic acid. Folic acid corrects the anaemia of B12 deficiency, so the blood picture looks normal and the warning sign vanishes while the neurological damage carries on. The government acknowledges this, saying the level of fortification had to be restricted due to: “the risk of masking B12 deficiency”.
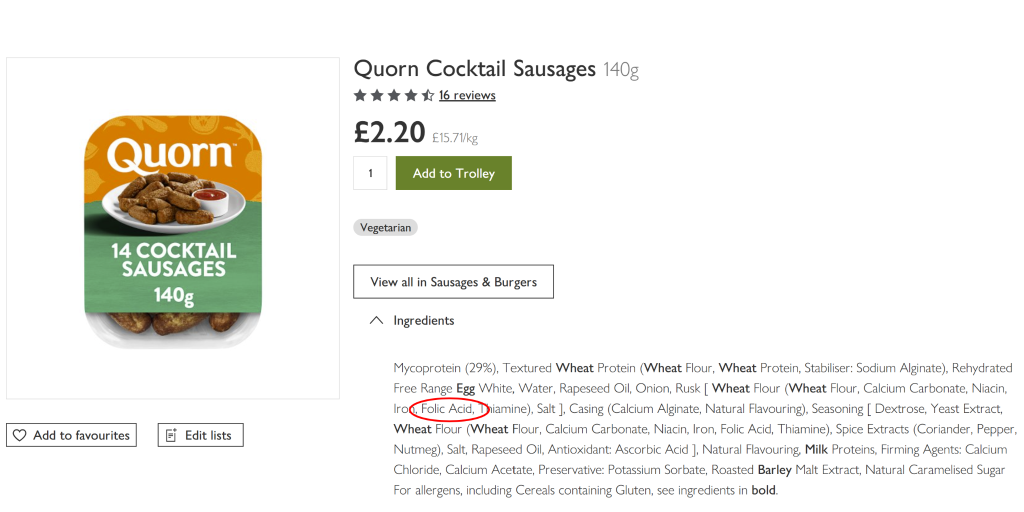
What practical advice is an NHS clinician supposed to give someone who has been advised to avoid folic acid once it has become part of the national food supply? “You are now living in a world that is flooded with a product that would be toxic to your body. Go carnivore or paleo.”? Even that advice would fail:
It really has found its way into all sorts of food you might not associate with flour:
“Foods in the UK have been voluntarily fortified with folic acid for many years, including products such as breakfast cereals and spreads, without evidence of adverse health effects.”
This exemplifies the government attitude to public safety. Millions of people are exposed with no attempt made to measure negative outcomes and then they conclude it happened “without evidence of adverse health effects.”
“The UK Government and devolved governments are exploring how we will evaluate the impact of the policy.”
I wonder if their attempts to evaluate the impact will include measuring miscarriage rates, prostate cancer rates, neurological damage in those with pernicious anaemia?
Overall both responses are hugely disappointing and show a failure to engage with the serious issues on this subject. Both responses largely restate the Government’s existing policy. Whatever one’s view of folic acid, that is not how parliamentary petitions are supposed to work.
It is not too late to sign or get your friends and family to sign to trigger a proper parliamentary debate and enable some public conversation and the beginnings of the information communication needed for informed consent.
