

How many Russian flu deaths were toxicological?
Dr Clare Craig
Today historians debate whether Russian influenza (1889-1891) was caused by influenza virus or coronavirus. That is the wrong question. The more important question is what contemporary observers were saying about the medicines.
On 12 January 1890 the Parisian satirical magazine Le Grelot published a drawing it called “La ronde des médecins et des potards”: the round-dance of the doctors and the druggists. A circle of three skeletons leads a danse macabre; the physicians are all mesmerised as they exhale aerosols. With them a woman wears a “fleurs pectorales” dress, representing the herbal respiratory remedy. She is being given an enema, a common device in cartoons to indicate that she had been purged from the debate. There was no vaccination. Dancing merrily are two plump, cheerful female figures held by a grinning pharmacist with two others kissing them each on the cheek: one wears a dress reading La Quinine, the other Antipyrine. Across the top runs the banner, “Tout le monde l’a (repeat x3) – l’influenza!” All the world has – influenza.
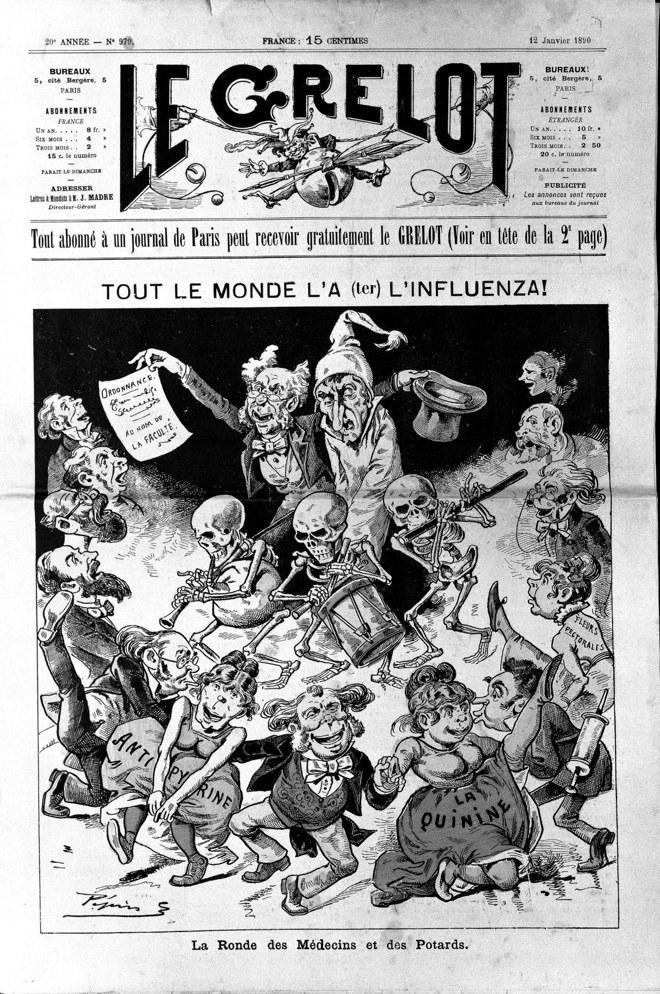
“La ronde des médecins et des potards,” Le Grelot, Paris, 12 January 1890. Wellcome Collection.
No French reader in January 1890 needed those two labels explained. Russian flu began in 1889 and was half way through its three year march across the world. Quinine and antipyrine were the celebrated remedies for this ‘influenza’. Quinine, from the bark of the cinchona tree, and is used to this day. Antipyrine was a new synthetic drug made from coal tar.
A synthetic drug
Antipyrine had been made for the first time only seven years earlier, in 1883, by the German chemist Ludwig Knorr, a pupil of Emil Fischer. Knorr had not set out to make a fever drug at all. He was trying to build a synthetic relative of quinine from phenylhydrazine, a product of the coal-tar dye industry. Initially he produced a pyrazolone which was methylated, on the suggestion of the pharmacologist Wilhelm Filehne making it into antipyrine. The name derived from pyrexia, the Latin word for fever.
It was among the first wholly synthetic drugs, and the first to be manufactured and prescribed on a truly industrial scale.
Was it a coincidence that waves of mortality from Russian influenza arrived at the precise moment medicine acquired its first mass-produced synthetic drug? Australian chemists in 1888 described their long search for “a good artificial substitute for quinine,” and Melbourne’s Argus in March 1890 reported the use of “antipyrin (dimethyloxy quinine), which is a form of quinine.”
The years of enthusiasm
The drug was embraced as a panacea and saviour and no reasonable caution was evident. It could reduce a fever by several degrees within hours and that alone was considered evidence of success. By 1885 colonial papers were relaying claims that the drug could be given at ten grammes in twenty-four hours with “no unpleasant consequences,” and that it worked for everything from typhoid and diphtheria to scarlet fever and consumption. By 1888 it was being promoted as an “infallible remedy” for sea-sickness, credited with “all the virtues of a prophylactic and a cure”. Any drug used prophylactically in the healthy can have the largest negative impacts. Fear of an illness becomes enough for intervention creating a potential positive feedback loop based on the harm caused. Even the journalist who reported the sea-sickness cure paused to add that “the same kind of claim has been made over and over again for a score of other remedies.” Pharmaceutical evangelism is not a modern invention.
A principal remedy of the pandemic
For Russian Influenza the contemporary record leaves no doubt that it was a principal treatment. The Argus reported in March 1890 that antipyrine subdued the fever and relieved the pain “within from 10 to 20 minutes.” Newspapers that April described doctors dispensing “their quinine, antipyrine, phenacetin and so on.” By the autumn of 1891 one report stated plainly that “the principal remedy given in general cases appears to have been anti-pyrine, but the supply of this drug has run out,” adding that “attempts of wholesale houses to obtain supplies from other colonies have failed” — a point Sydney’s Daily Telegraph made independently that same October. A drug barely seven years old had become, in places, the default pharmaceutical response to an epidemic. It was used so heavily that the colonies ran short of it.
The warnings
The recognition of the harm caused was real but documenting it was slow. Under the heading “The Dangers of Anti-pyrin,” a Victorian paper in June 1894 reported that investigation had “formally established” that the drug could produce “cardiac weakness and irregularity, cyanosis, … collapse and death.”
In 1894 Dr J. Jarvie Hood of Grafton published a case in the Medical Gazette. A recovering patient was “attacked with influenza, headache and pain in the back being excessive,” and Hood prescribed antipyrine, “every two hours till relieved.” Her skin worsened after the first dose; after the second, he wrote, “the effect of this was indeed dire,” with old healed lesions breaking out afresh. She recovered only once the drug was stopped. His emphasis was precise and damning in its ordinariness: only ten grains had been taken in all, “yet with such serious effect.”
The same year a Sydney correspondent set down the mechanism with uncomfortable clarity. Antipyrine, he wrote, “is one of the most deadly drugs in the whole pharmacopeia when given without judgment or in too large doses.” It lowers not merely the fever but the circulation, and so “in most cases of influenza the pulse is quick, but weak, a sure sign that the administration of anti-pyrin will be attended with danger.” He went further than most: “What a sight it would be if in any large cemetery there were written on the tombstones the real cause of death, not that assigned in the medical certificate. ‘Anti-pyrin’ would be the brief curt epitaph on a large number.”
It is worth sharing that vivid description but it was only published in a newspaper. Alongside it, Dr Isaac Burney Yeo, consulting physician at King’s College Hospital published in The Lancet in 1895. He condemned “the routine and somewhat reckless use of such drugs as antipyrin and salicin, which I observe is still common in the treatment of influenza.” These drugs, he held, “possess no real antitoxic influence over this affection,” and so leave the patient “exposed to all the serious after-effects of the influenzal intoxication,” even rendering him “more susceptible to some of them.” Patients so treated, he added, “are very subject to recurrent attacks of cardiac debility,” and he had been “struck by the pale, exhausted, worn, and shrunken aspects of some of these convalescents.” It had taken nearly a decade for a senior consultant, in the leading medical journal of the day, to describe the harm from this novel drug.
Blaming the disease
The symptoms physicians ascribed to Russian influenza and the adverse effects they ascribed to antipyrine were pretty much the same symptoms.
| Severe influenza | Antipyrine toxicity |
| Prostration | Alarming depression |
| Profuse sweating | Excessive sweating |
| Weakness | Loss of power in the legs |
| Circulatory collapse | Partial or complete collapse |
| Delirium | Mania |
| Cardiac involvement | Cardiac weakness and irregularity |
| Cyanosis in severe cases | Cyanosis |
| Death | Death |
A physician of the 1890s watching an influenza patient sink after antipyrine had no reliable means of telling disease progression from drug toxicity, and when the patient died the death was certified as influenza. A drug capable of producing collapse and death at ordinary doses was being given, at enormous scale, to patients whose own illness was blamed for producing collapse and death. Those deaths were then certified as due to Russian influenza and no-one looked again.
Was it a coronavirus?
There is debate as to whether Russian influenza was due to an H3 subtype influenza or was in fact human coronavirus OC43. In 2005 Vijgen et al dated the divergence of the human coronavirus OC43 from its bovine relative to around 1890 and proposed that its emergence caused the Russian flu. These arguments were reignited in 2020 to claim that coronaviruses had caused mass death in the past. A 2023 reanalysis by Shaw and Gatherer places the split nearer 1898–1902, and many influenza virologists remain unpersuaded.
Importantly, because of those death certificates, no one is questioning what caused the excess mortality. Even if viruses mutate, that is not enough of a reason for mass death. Only a fraction of the population are susceptible to respiratory virus infections each year and our multifaceted immune systems protect all but the frailest from dying.
Even though doctors pointed to the drugs at the time, that story has been buried in history while the story of a viral pandemic has been amplified.
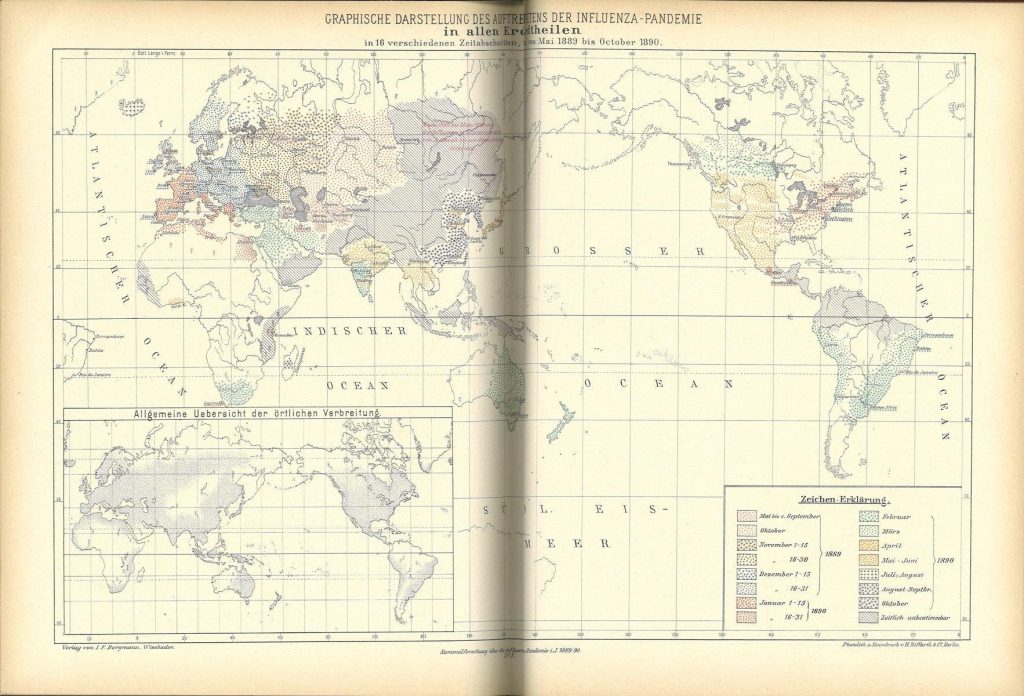
Map showing global spread of Russian flu mortality waves from 1889 to 1890.
It is notable that the death waves took eighteen months over two whole years to cross the globe and continued for four years. This is a feature that is much more in keeping with a spread of hysteria accompanied by drug overdosing than the spread of an aerosolised virus which can spread long distances.
Parallels with 1918
In 2009 Karen Starko, writing in Clinical Infectious Diseases, argued that the mortality of the Spanish influenza may have been amplified by salicylate (aka aspirin) toxicity and pulmonary oedema, such that “a significant proportion of the deaths may be attributable to aspirin.” Very high aspirin doses were recommended in 1918 by the US Surgeon-General, the US Navy and the Journal of the American Medical Association, in the weeks before the October death spike. If that question is reasonable for aspirin in 1918, it is no less reasonable for antipyrine in 1890. And the antipyrine signal is in one respect the stronger of the two. Starko’s case for aspirin had to be reconstructed nine decades later, whereas the case against antipyrine was made by physicians at the time, in The Lancet and in the case literature, within a few years of the epidemic itself.
Instead of removing the danger, the drug survived under the generic name phenazone and remained in use long after the Russian influenza era. It continued to be used until being usurped by aspirin which had originally been made from willow bark but was mass production from coal tar products by the turn of the century.
Impact of antipyrine
A substantial proportion of the mortality attributed to influenza may in fact have been iatrogenic. The toxicity at ordinary doses is documented . A published case reported a grave reaction to ten grains, and a newspaper warned that investigation had “formally established” deaths even in skilled hands. The fact that the link was reported by contemporary experts in The Lancet as well as in newspapers is strong evidence that the impact was profound.
However, it is not possible in retrospect to quantify the mortality impact.
The tragedy is not merely that antipyrine may have contributed to mortality. It is that the possibility was recognised at the time, recorded in medical journals and newspapers, and then almost entirely forgotten.
