
HART has been trying to raise awareness for over two years
If you would like to join the debate on our articles, comments are open and welcome on our Substack version, so please feel free to subscribe and join the conversation.
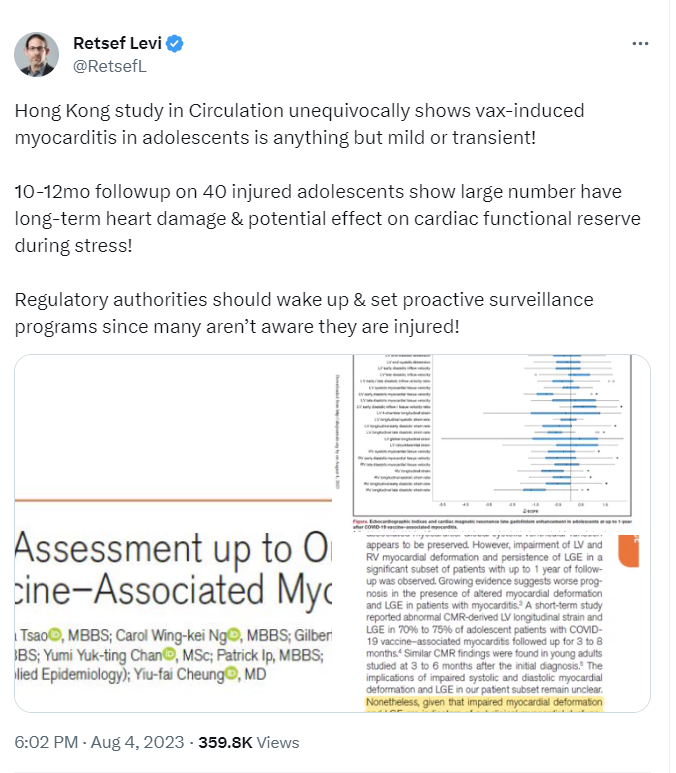
A new study performed on adolescents in Hong Kong who suffered myocarditis after mRNA injection in Circulation appears to be generating quite a lot of discussion over how common it is, and what the long-term outcomes are for those unfortunate enough to suffer from this side effect.
Broadly speaking, the more we learn, the worse it looks.
NB: This phrase also applies to every aspect of the injections, as well as to every intervention imposed by governments on their citizens.
In HART we have been writing about myocarditis regularly for well over 2 years now.
Our first public mention of myocarditis was in this open letter from UK doctors to Dr June Raine, Chief Executive, MHRA dated 17 May 2021, in which we expressed our “grave concerns regarding all proposals to administer COVID-19 vaccines to children”.
We mentioned it again in our “Vaccination Update” article dated 17 June 21 and then again a week later.
On 6 July 2021 we published a stinging criticism of Devi Sridhar’s extremely misleading statements made on Good Morning Britain, in which she downplayed the risks of myocarditis.
Our first longer article on the subject appeared in August 2021 and can be found here.
A year ago, we published an article warning that what is being reported as myocarditis may be the tip of the iceberg, since:
- active surveillance systems found substantially more cases than passive systems.
- The incidence of subclinical cases may dwarf the clinical cases.
Since then, we have also written about further worrying data emerging, especially regarding subclinical cases which are only found by measuring troponin levels systematically.
This is logistically simple to perform, so it is criminal that it wasn’t done as soon as the signal of potential harm emerged.
More recently, this study performed in Swiss healthcare workers has essentially affirmed the findings of the study performed in Thai adolescents above – albeit that this study was exclusively following the Moderna product, rather than Pfizer.
Now we have the latest study from Hong Kong referred to at the top of this article. Shocking though this might appear, it is possible that this study severely underestimates the extent of the problem for several reasons. Our concerns can be gleaned from the email we sent to the lead author:
Dear Dr Cheung,
I was most interested to read your findings contained within this study. (Cardiovascular Assessment up to One Year After COVID-19 Vaccine–Associated Myocarditis)
I was wondering if you could clarify a few things:
- You say the study covers all 40 cases of myocarditis identified. Can you expand on what criteria were originally applied for a diagnosis to be made, and how these cases were identified – was it just via a passive reporting system, or through active surveillance?
- What was the period studied – ie what date ranges did the myocarditis cases occur within?
- Is it possible to draw any conclusions about the relationship between persistence of symptoms and abnormalities at follow up, especially gadolinium enhancement? Were those without symptoms less likely to have abnormalities?
- Likewise, is it possible to draw any conclusions about the relationship between initial symptoms and persistent abnormalities at follow up, especially gadolinium enhancement? Were those without or with milder symptoms at initial diagnosis less likely to have abnormalities?
- You say 7 reported “non cardiac” chest pain. What is meant by that, and how was a cardiac origin ruled out?
Many thanks
Dr Jonathan Engler MB ChB
(United Kingdom)
With impressive speed, we received a response back overnight:
Dear Dr Engler,
Thank you for your interest in the our article.
For the points being raised:
- The Brighton Collaboration Myocarditis Case Definition was used. The patients admitted to one of the hospitals of the Hospital Authority in Hong Kong (the major publicly funded healthcare provider in Hong Kong that shoulders about 90% of the inpatient needs) with the diagnosis were proactively reported to the Advanced Incident Reporting System. These adolescents were referred to our centralized clinic for follow-up cardiac assessment.
- July 2021 to January 2022
- The symptoms were based on the history asked over the interm follow-up assessment and did not persist. It was not possible to draw conclusion between persistence of symptoms and persistent echo/CMR abnormalities. All of our patients had mild symptoms (chest pain with or without fever or palpitations) at presentation and none required intensive care and inotropic support at diagnosis. Hence, it was not possible to stratify patients into two groups (mild vs severe symptoms) to analyse the relationship between severity at initial presentation and persistent echo/CMR abnormalities.
- As aforementioned in point 3.
- This was based on assessment by the paediatric cardiologist through history, physical examination and a normal ECG. The pain was assessed to be either non-specific or suggestive or musculoskeletal in origin, with no suggestion of being pericardial or anginal in origin.
Once again, thank you for the interest and the interesting points being raised.
Best wishes,
YF
Yiu-fai Cheung, MD
Bryan Lin Professor in Paediatric Cardiology
Department of Paediatrics and Adolescent Medicine
Hong Kong Children’s Hospital
School of Clinical Medicine
LKS Faculty of Medicine
The University of Hong Kong
Hong Kong
So our concerns are several:
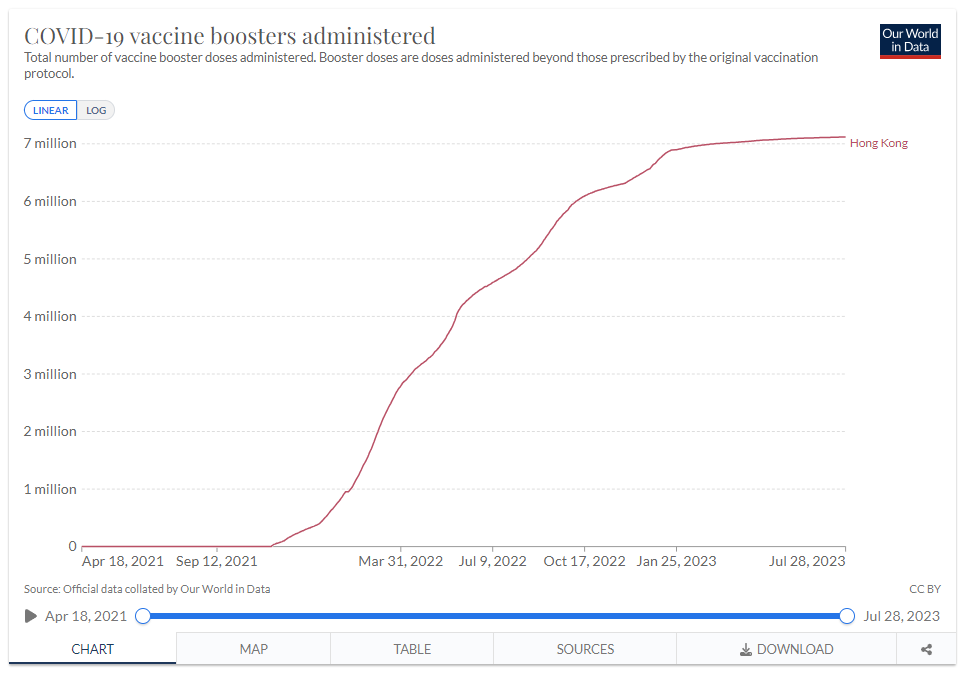
1. The study only covers a 6-month period during which the total number of doses administered rose from around 4m to 10m. It now stands at over 20m.
In particular, it is to be noted that boosters didn’t really get going until the last month of the study period, after which over 6 million doses were injected. This study may only be identifying a small proportion of cases, particularly if the boosters are worse.
2. It seems that they are only considering confirmed, hospitalised cases. The study adds nothing to the question of longer-term harms from either milder cases not requiring hospitalisation, or sub-clinical cases.
The answer to the question about non-cardiac chest pain does not provide much reassurance. 18% reported such pain at 10 months follow up. These adolescents had a history of myocarditis, and the pain is easily confused with musculo-skeletal injury.
So in summary, this study adds no reassurance in relation to:
- incidence rates, including milder and subclinical case;
- whether milder / subclinical cases suffer long-term harm.
It has been several years since this signal emerged. That there are still so many unanswered questions, including that of the mechanism of harm, is quite astonishing.
This clip of the answers being given by a Pfizer employee to questions from an Australian Senator is jaw-dropping.
In subsequent correspondence with the authors, we voiced our outstanding concerns and shared our work:
Subject: RE: Your myocarditis study
Thank you so much for the rapid response.
In summary, it looks like your study may underestimate the extent of the problem since:
- The incidence relies on active hospitalized cases only
- We do not know the rate of mild cases not requiring hospitalization, nor subclinical cases
- We do not know whether these have a normal long-term prognosis
- The period of study only includes one month (the final month) when the boosters are included – many were boosted, presumably some multiply, after the study
- The period of study excludes a substantial part of the earlier rollout.
You may be interested that our group has been writing extensively on this topic for 2 years now.
https://www.hartgroup.org/?s=myocarditis&submit=Search&swpmfe=652ea0d21b1427a1bfa685e40d9bc1de
Best wishes
Jonathan
We received the below response:
Dear Jonathan,
Many thanks for sharing the insightful articles written by your group over the past few years.
I agree that there is a possibility of underestimation given the reasons as you have correctly highlighted.
Through publishing our results, notwithstanding the limitations, we hope that the international academic community can add more data to shed light
on the long-term clinical and functional implications of the subclinical abnormalities found in our study. We eagerly await to see these data from other groups of investigators.
Best wishes,
YF
Yiu-fai Cheung, MD
Bryan Lin Professor in Paediatric Cardiology
Department of Paediatrics and Adolescent Medicine
Hong Kong Children’s Hospital
School of Clinical Medicine
LKS Faculty of Medicine
The University of Hong Kong
Hong Kong
The concern expressed by the lead author that this problem should be properly investigated should shame other cardiologists, especially those in the “Western” world, who have mostly adopted an ostrich-like posture in relation to this topic.
