

Andrew Bridgen MP finally secures an adjournment debate
Also available on Substack – Come and join the conversation with open comments
20 OCTOBER 2023, EXCESS DEATH DEBATE, HOUSE OF COMMONS, LONDON (transcript)
2:32pm : Andrew Bridgen (North West Leicestershire) (Reclaim)
“We have experienced more excess deaths since July 2021 than in the whole of 2020.
| Number of excess deaths according to Office for Health Improvements and Disparities | |
| Mar-Dec 2020 (there were fewer deaths than expected in Jan and Feb 2020 according to ONS) | 69,293 |
| Jul 2021 – Sept 2023 | 76,554 |
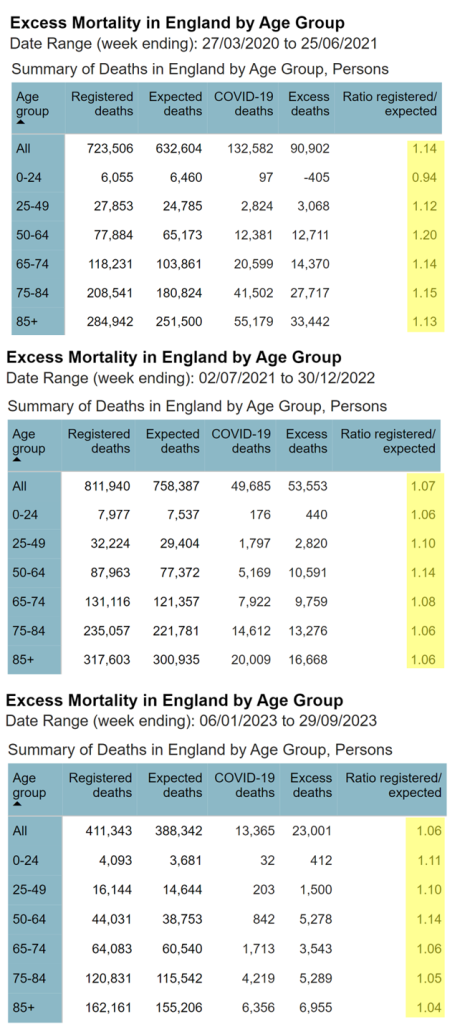
Unlike during the pandemic, however, those deaths are not disproportionately of the old. In other words, the excess deaths are striking down people in the prime of life (Fig 1).
But no one seems to care. I fear that history will not judge this House kindly. Worse still, in a country supposedly committed to free and frank exchange of views, it appears no one cares that no one cares. Well, I care, Mr Deputy Speaker, and I credit those Members in attendance today, who also care. I thank the hon. Member for Lincoln (Karl McCartney) for his support, and I am sorry that he could not attend the debate.
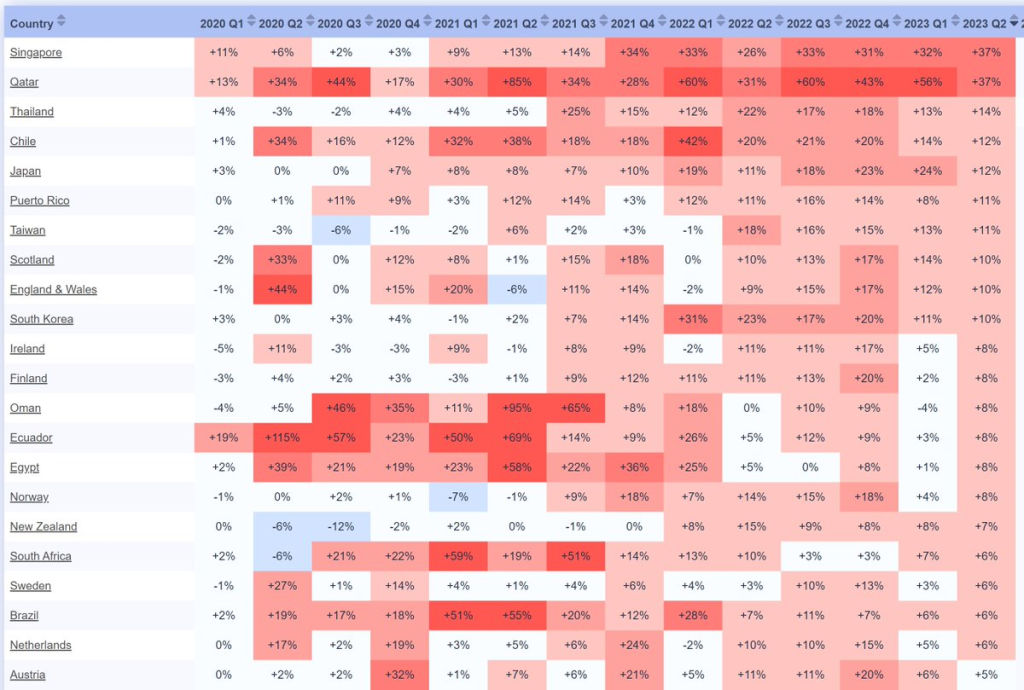
It has taken a lot of effort, and more than 20 rejections, to be allowed to raise this topic, but at last we are here to discuss the number of people dying. Nothing could be more serious. Numerous countries are currently gripped by a period of unexpected mortality (Fig 2), and no one wants to talk about it. It is quite normal for death numbers to fluctuate up and down by chance alone but what we are seeing here is a pattern repeated across countries, and the rise has not let up.
The media have let the British public down badly. There will be a full press pack going out to all media outlets following my speech, with all the evidence to back up all the claims I will make, but I do not doubt that there will be no mention of it in the mainstream media.
One might think a debate about excess deaths would to be full of numbers, but this speech does not contain many numbers because most of the important numbers are being kept hidden. Other data has been oddly presented in a distorted way, and concerned people seeking to highlight important findings and ask questions have found themselves inexplicably under attack.
How are excess deaths are determined?
Before debating excess deaths, it is important to understand how excess deaths are determined. To understand whether there is an excess, by definition, we need to estimate how many deaths would have been expected. The Organisation for Economic Co-operation and Development (OECD) uses 2015-2019 as a baseline, and the Government’s Office for Health Improvement and Disparities uses a 2015-2019 baseline modelled to allow for ageing. I’ve used that data here.
Unforgivably, the Office for National Statistics (ONS) has included deaths in 2021 as part of its baseline calculation for expected deaths, as if there was anything normal about the deaths in 2021. By exaggerating the number of deaths expected, the number of excess deaths can be minimised. Why would the ONS want to do that?
There is too much we do not know, and it is not good enough. The ONS publish promptly each week the number of deaths that were registered. While that is commendable, it is not the data point that really matters. There is a total failure to collect, never mind publish, data on deaths that are referred for investigation to the coroner. Why does this matter? A referral means that it can be many months—or, given the backlog, many years—before a death is formally registered. Needing to investigate the cause of death is fair enough, but failing to record when the death happened is not.
Because of that problem, we have no idea how many people died in 2021, even now. The problem is greatest for the younger age groups, where a higher proportion of deaths are investigated. This data failure is unacceptable and must change. There is nothing in a coroner’s report that can bring anyone back from the dead, and those deaths should be reported. The youngest age groups are important not only because they should have had their whole lives ahead of them. If there was a new issue cause of excess mortality across the board, it would not be noticed so much in the older cohorts, because the extra deaths would be drowned out among the expected deaths. However, in the youngest cohorts that is not the case.
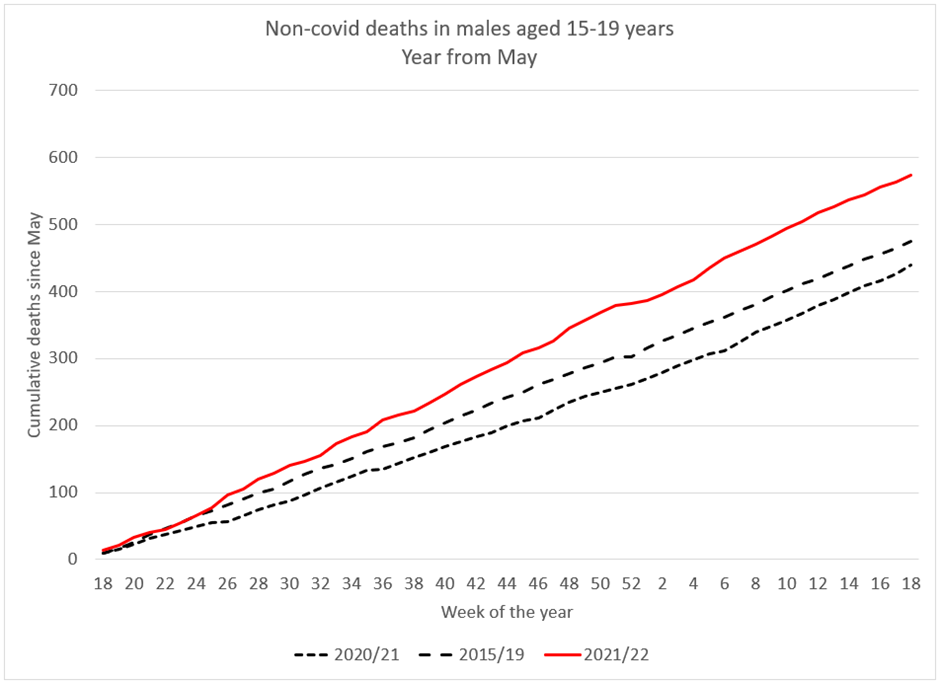
There were nearly two extra deaths a day in the second half of 2021 among 15- to 19-year-old males (Fig 3), but potentially even more if those referred to the coroner were fully included. In a judicial review of the decision to vaccinate yet younger children, the ONS refused in court to give anonymised details about these deaths. It admitted that the data it was withholding was statistically significant. It said: “the ONS recognises that more work could be undertaken to examine the mortality rates of young people in 2021, and intends to do so once more reliable data are available.”
How many more extra deaths in 15 to 19-year-olds will it take to trigger such work? Surely the ONS should be desperately keen to investigate deaths in young men. Why else do we have an independent body charged with examining mortality data? Surely the ONS has a responsibility to collect data from coroners to produce timely information.
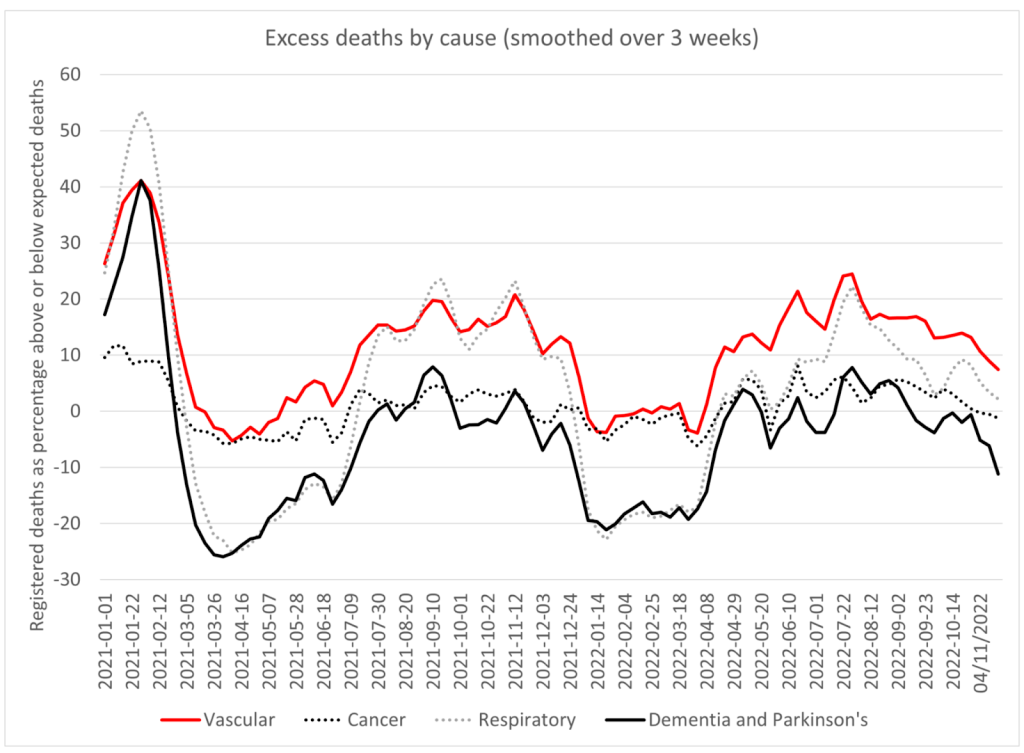
Let us move on to old people. Most deaths in the old are registered promptly, we do have a better feel for how many older people are dying. Deaths from dementia and Alzheimer’s show what we ought to expect (Fig 4): there was a period of high mortality coinciding with covid and lockdowns, but ever since, there have been fewer deaths than expected. After a period of high mortality we expect and historically have seen a period of low mortality, because those who have sadly died cannot die again.
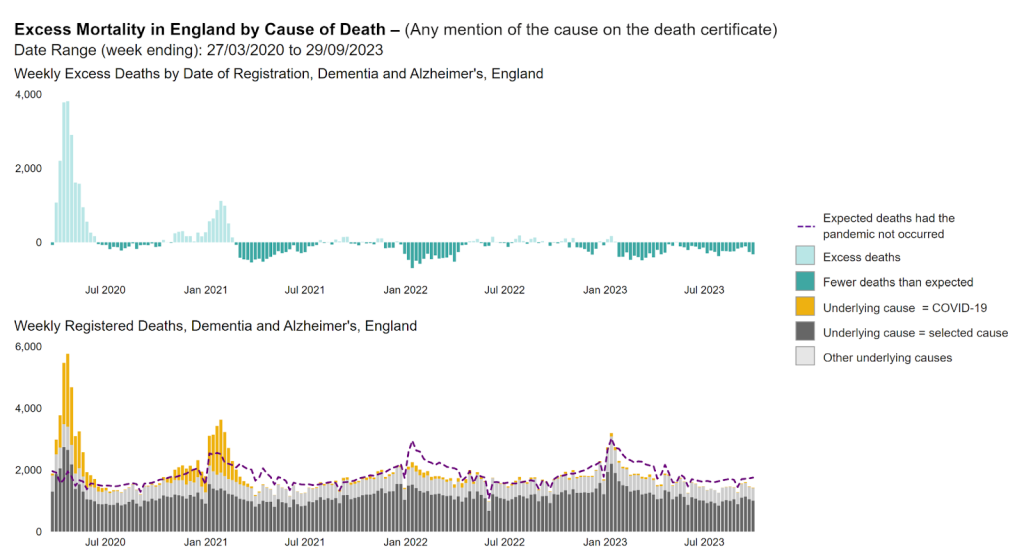
Those whose deaths were slightly premature because of covid and lockdowns died earlier than they otherwise would have. That principle should hold true for every cause of death and every age group, but that is not what we are seeing. Even for the over 85–year–olds, according to the Office for Health Improvement and Disparities, there were 8,000 excess deaths—4% above the expected levels—for the 12 months starting in July 2020. That includes all of the autumn 2020 wave of covid when we had tiering and the second lockdown and all of the first covid winter. However, for the year starting July 2022, there were more than 18,000 excess deaths in this age group—9% above expected levels. That is more than twice as many in a period when there should have been a deficit and when deaths from diseases previously associated with old age were fewer than expected. I have raised my concerns about NG163 and the use of midazolam and morphine, which may have caused—and may still be causing—premature deaths in the vulnerable, but that is, sadly, a debate for another day.
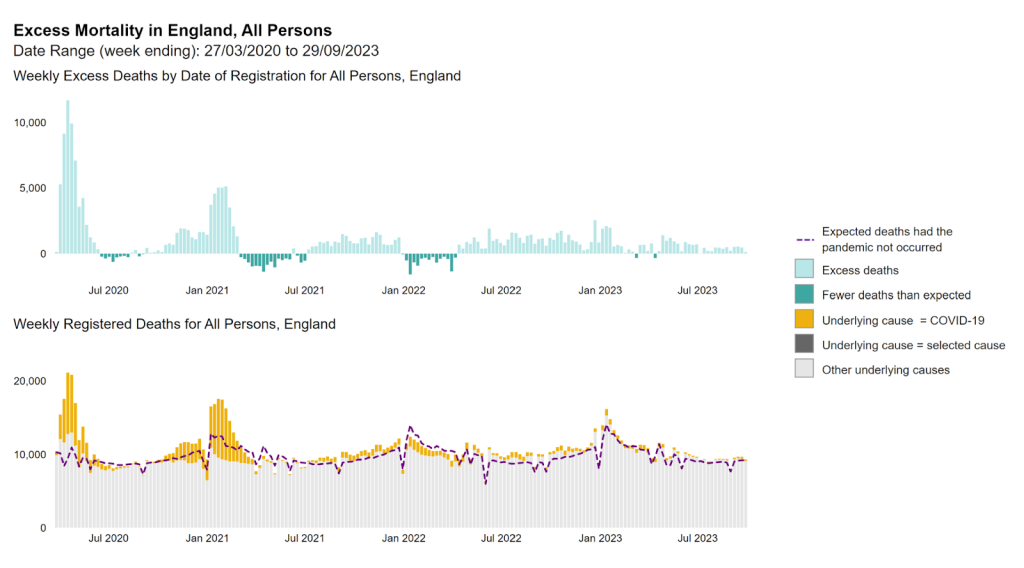
There were just over 14,000 excess deaths in under 65-year-olds before vaccination from April 2020 to the end of March 2021. However, since that time, there have been over 21,000 excess deaths, ignoring the registration delay problem, and the majority of those deaths—58% of them—were not attributed to covid. We turned society upside down before vaccination because of fear of excess deaths from covid, but today we have substantially more excess deaths, and in younger people, and there is a complete, eerie silence. The evidence is unequivocal. There was a clear stepwise increase in mortality following the vaccine rollout (Fig 5). There was a reprieve in winter of 2021-2022 because there were fewer than expected respiratory deaths, but otherwise the excess has been incessantly at this high level.
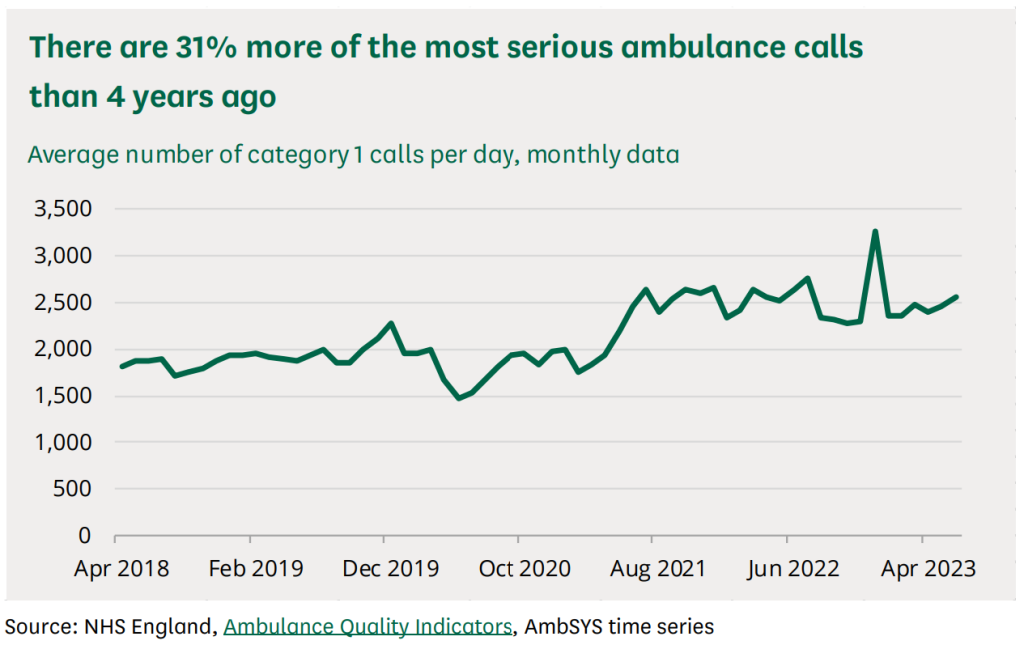
Ambulance data for England provides another clue. Ambulance calls for life-threatening emergencies were running at a steady 2,000 calls a day until the vaccine rollout. From then, they rose to 2,500 daily, and calls have stayed at that level since (Fig 6).
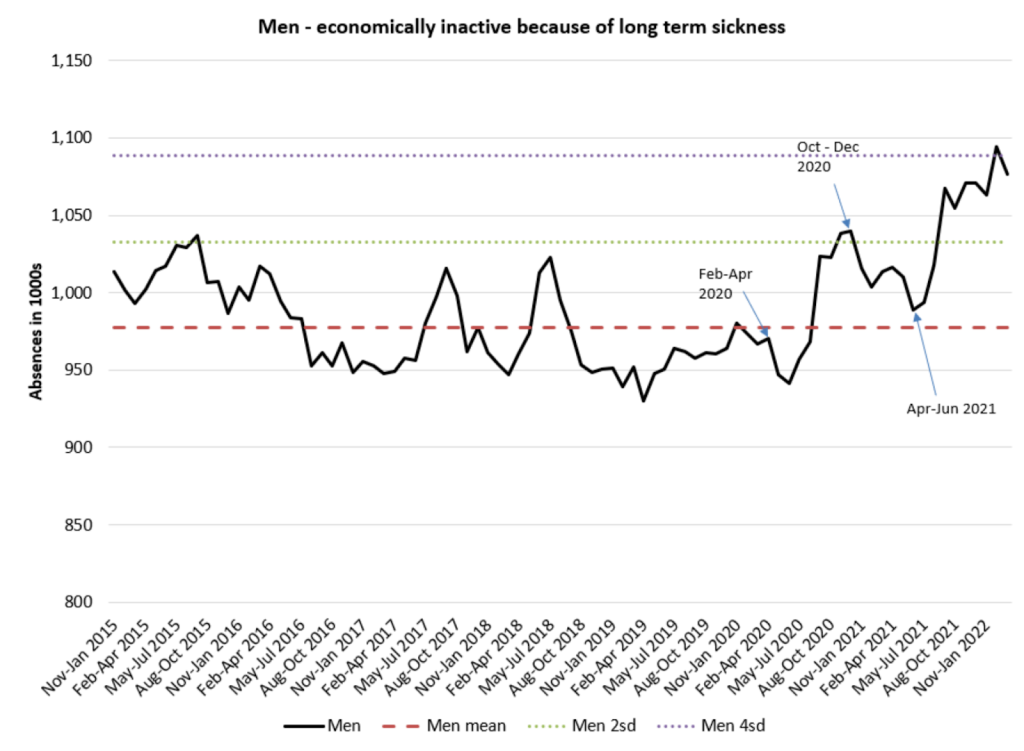
The surveillance systems designed to spot a safety problem have all flashed red, but no one is looking. Claims for personal independence payments from people who have developed a disability and cannot work rocketed with the vaccine roll-out and have continued to rise ever since (Fig 7a and b).
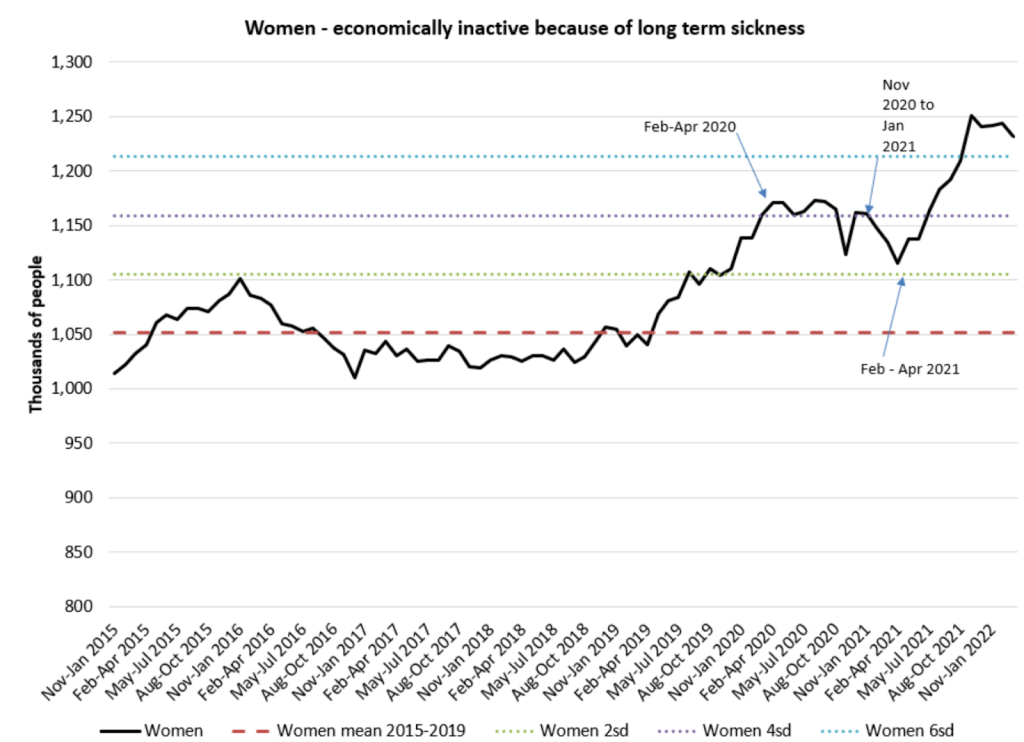
Fig 7a: Responses to ONS workforce survey shows plateauing of long term sickness in 2020, a fall in early 2021 and then a sharp rise after vaccine rollout: women
The same was seen in the US, which also started with the vaccine roll-out, not with covid (Fig 8).

A study to determine the vaccination status of a sample of such claimants would be relatively quick and inexpensive to perform, yet nobody seems interested in ascertaining this vital information. Officials have chosen to turn a blind eye to this disturbing, irrefutable and frightening data, much like Nelson did—and for far less honourable reasons. He would be ashamed of us.
Furthermore, data that has been used to sing the praises of the vaccines is deeply flawed. Only one covid-related death was prevented in each of the initial major trials that led to authorisation of the vaccines, and that is taking the data entirely at face value, whereas a growing number of inconsistencies and anomalies suggest that we ought not to do this. Extrapolating from that means between 15,000 and 20,000 people had to be injected to prevent a single death from covid. To prevent a single covid hospitalisation, more than 1,500 people needed to be injected. The trial data showed that 1 in 800 injected people had a serious adverse event, meaning they were hospitalised or had a life-threatening or life-changing condition. The risk of this was twice as high as the chance of preventing a covid hospitalisation. We are harming one in 800 people to supposedly save one in 20,000 people. That is madness.
The strongest claims have too often been based on modelling carried out on the basis of flawed assumptions. Where observational studies have been carried out, researchers will correct for age and comorbidities to make the vaccines look better. However, they never correct for socioeconomic or ethnic differences as that would make them look worse. That matters. For example, claims of higher mortality in less vaccinated regions of the United States took no account of the fact that this was the case before the vaccines were rolled out.
That is why studies that claim to show that the vaccines prevented covid deaths also showed a marked effect of them preventing non-covid deaths. The prevention of non-covid deaths was always a statistical illusion and claims of preventing covid deaths should not be assumed when that illusion hasn’t been corrected for. When it is corrected for, the claims of efficacy for the vaccines vanish with it.
Covid disproportionately killed people from ethnic minorities and lower socioeconomic groups during the pandemic. In 2020, deaths among the most deprived were up by 23% compared with 17% for the least deprived. However, since 2022 the pattern has reversed, with 5% excess mortality among the most deprived compared with 7% among the least deprived. These deaths are being caused by something different.
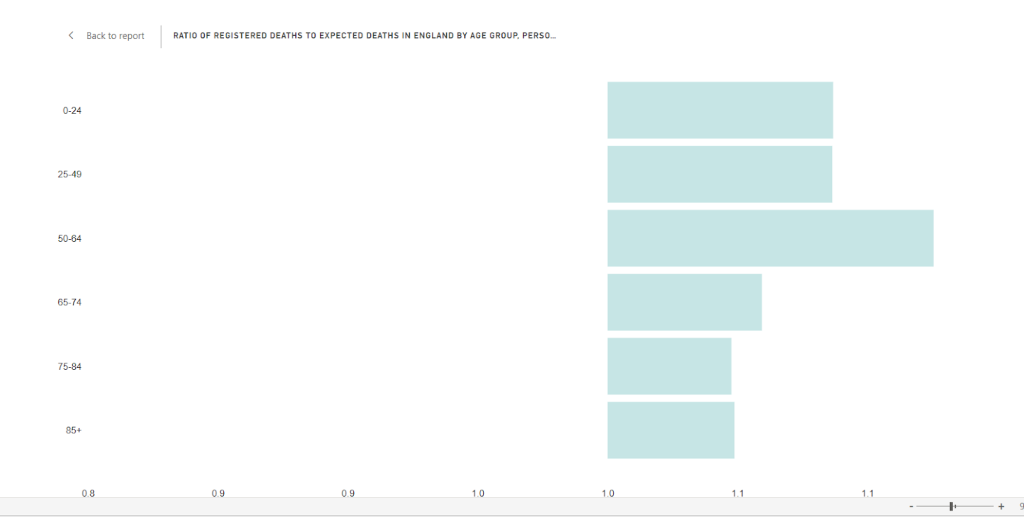
In 2020, the excess was highest in the oldest cohorts and there were fewer than expected deaths among younger age groups. However, since 2022, the 50 to 64-year-old cohort has had the highest excess mortality. Even the youngest age groups are now seeing a substantial excess, with a 9% excess in the under-50s since 2022 compared to 5% in the over 75 age group (Fig 9a).
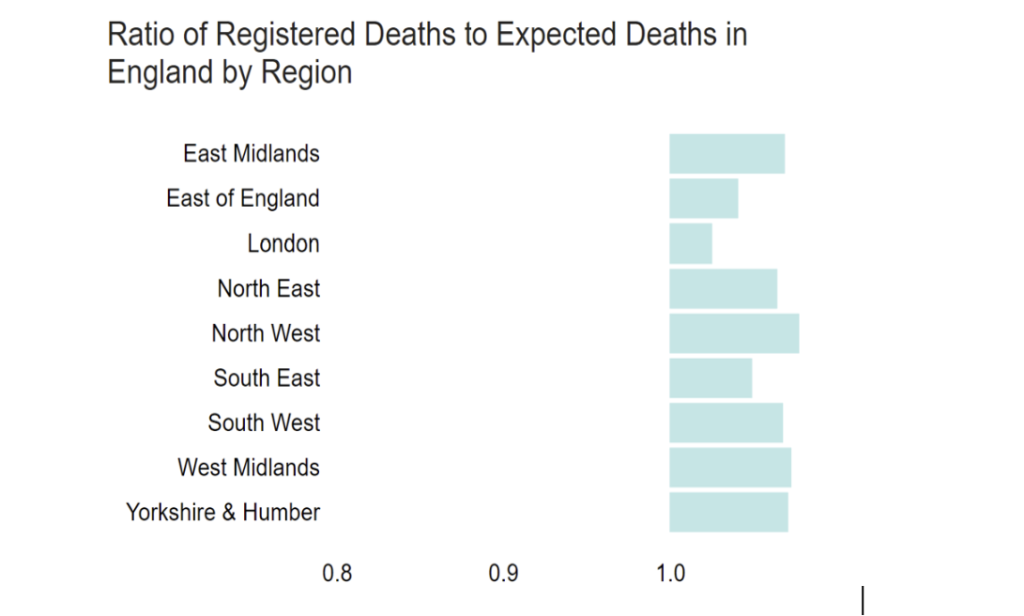
Despite London being a younger region, the excess in London is only 3%, whereas it is higher in every more heavily vaccinated region of the UK (Fig 9b). It should be noted that London is famously the least vaccinated region in the UK by some margin.
Studies comparing regions on a larger scale show the same thing. There are studies from the Netherlands, Germany and the whole world, each showing that the highest mortality after vaccination was seen in the most highly vaccinated regions.
So we need to ask: what are people dying of?
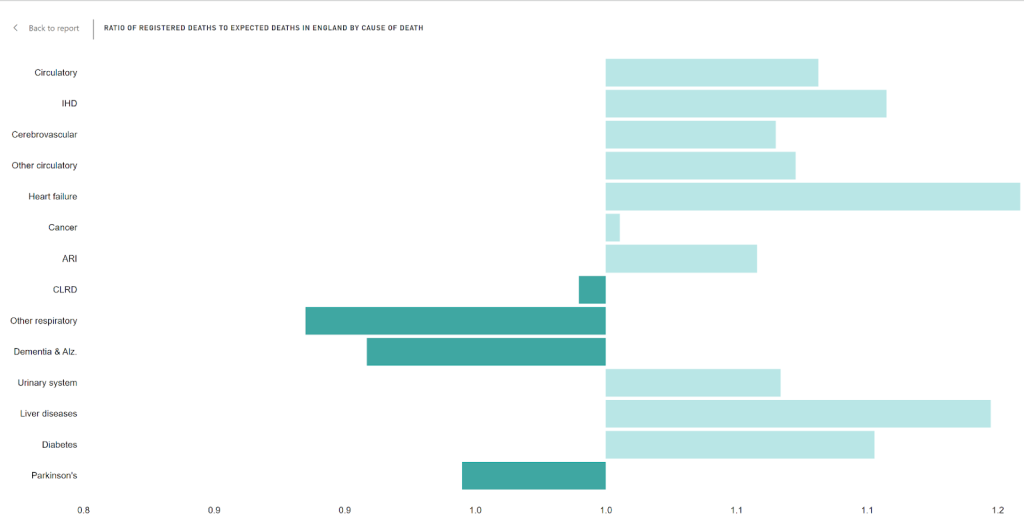
Since 2022, there has been an 11% excess in ischaemic heart disease deaths and a 16% excess in heart failure deaths (Fig 10). In the meantime cancer deaths are only 1% above expected levels which is further evidence that this is not simply some other factor that affects deaths across the board, such as failing to account for an ageing population, or a failing NHS. In fact, the excess itself has a seasonality, with a peak in the winter months. The fact that it returns to baseline levels in summer is a further indication that this is not due to some statistical error or an ageing population alone.
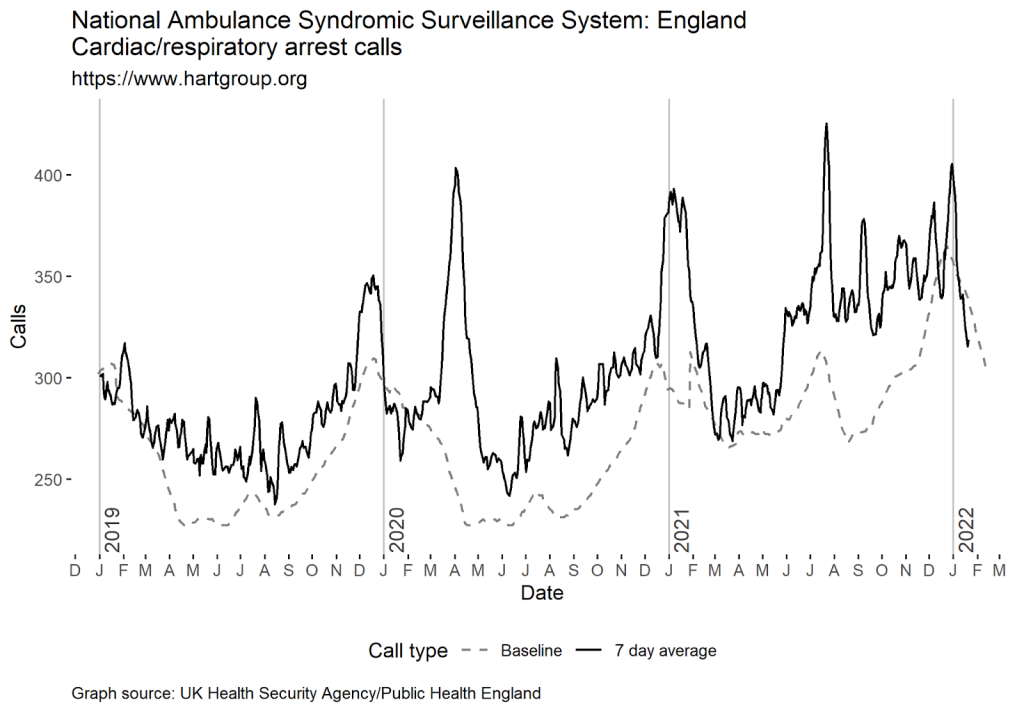
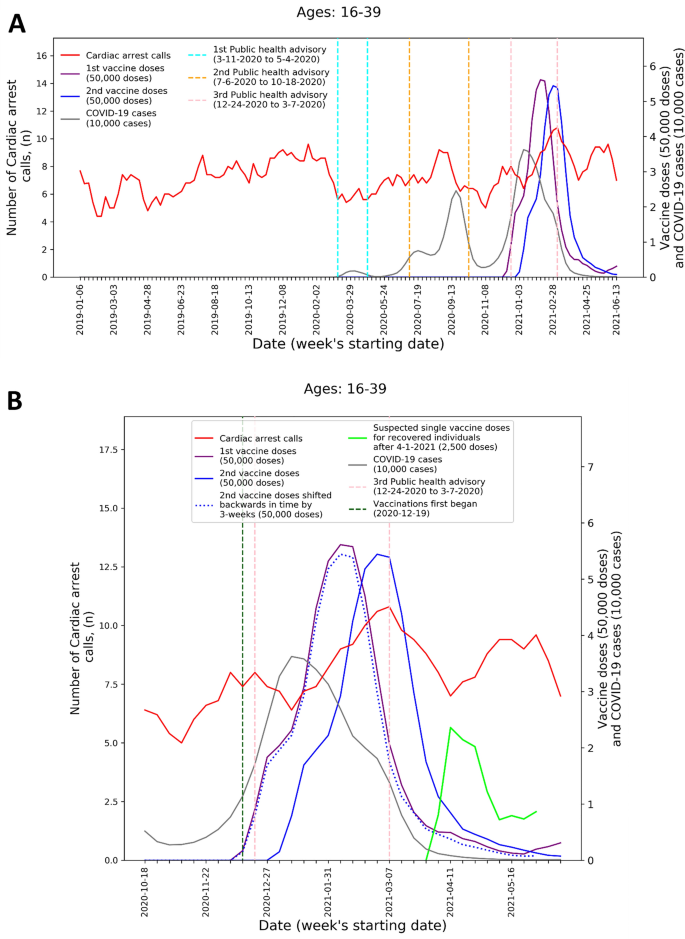
Dr Clare Craig from the HART—the Health Advisory & Recovery Team—first highlighted a stepwise increase in cardiac arrest calls after the vaccine rollout in May 2021 (Fig 11). HART has repeatedly raised concerns about the increase in cardiac deaths, and it has every reason to be concerned (Fig 12).
Four participants in the vaccine group of the Pfizer trial died from cardiac arrest compared to only one in the placebo group. Overall there were 21 deaths in the vaccine group up to March 2021, compared to 17 in the placebo group. There were serious anomalies about the reporting of deaths in this trial, with the deaths in the vaccine group taking much longer to report than those in the placebo group. That is highly suggestive of a significant bias in what was supposed to be a blinded trial.
An Israeli study clearly showed an increase in cardiac hospital attendances among 18-39 year olds that correlated with vaccination not covid (Fig 13).
There have now been several post–mortem case studies demonstrating a causal link between vaccination and coronary artery disease leading to death up to four months after the last dose. We need to remember that the trial safety was cut short to only two months, so there is no evidence of any vaccine safety beyond that point. The decision to unblind the trials after two months and vaccinate the placebo group is nothing less than a public health scandal. Everyone involved failed in their duty to the truth, but no one cares.
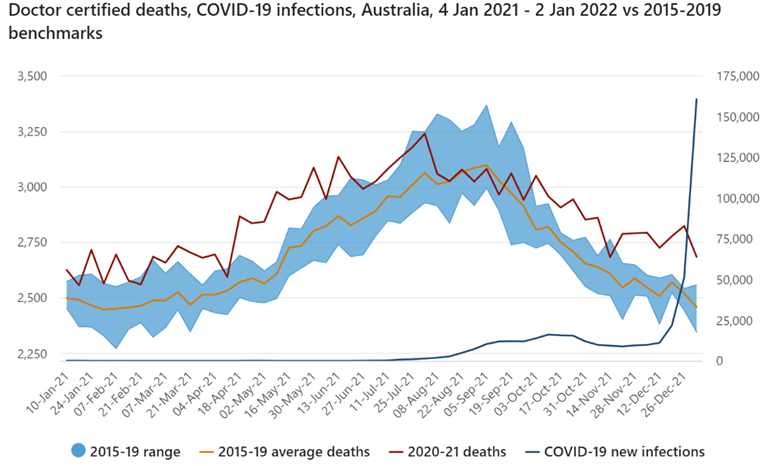
The one place that can help us understand exactly what has caused this is Australia, which had almost no covid when vaccines were first introduced, making it the perfect control group (Fig 14).
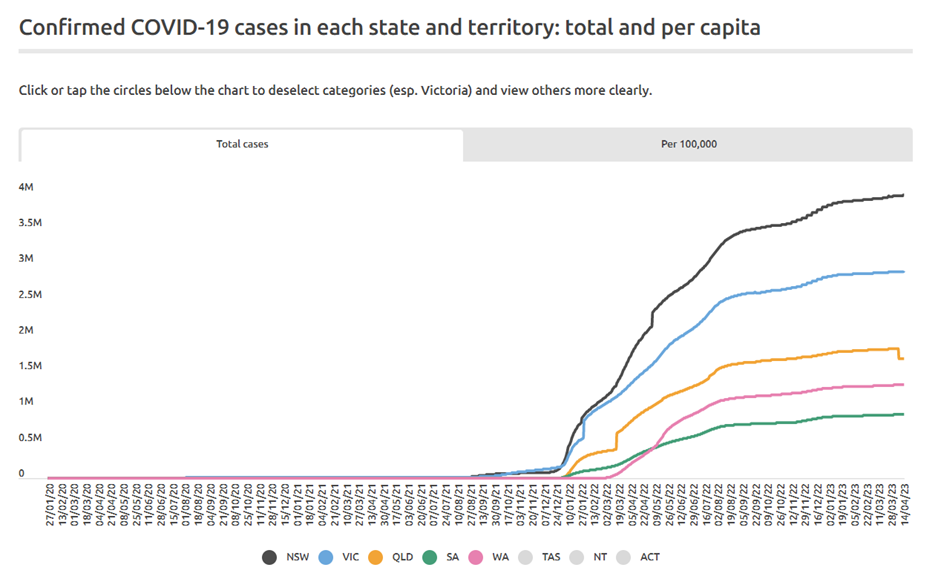
The state of South Australia had only had 1,000 cases of covid across its whole population by December 2021, before omicron arrived. What was the impact of vaccination there? For 15 to 44-year-olds, there were historically around 1,300 emergency cardiac presentations a month. With the vaccine roll-out to the under 50s, this rocketed reaching 2,172 cases in November 2021 in this age group alone, which was 67% more than usual (Fig 15).
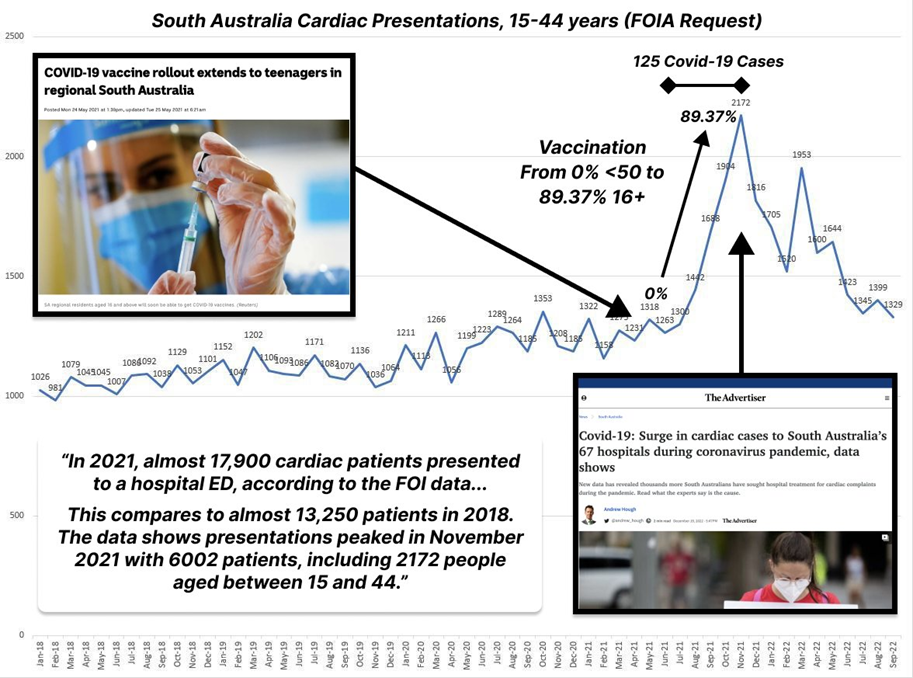
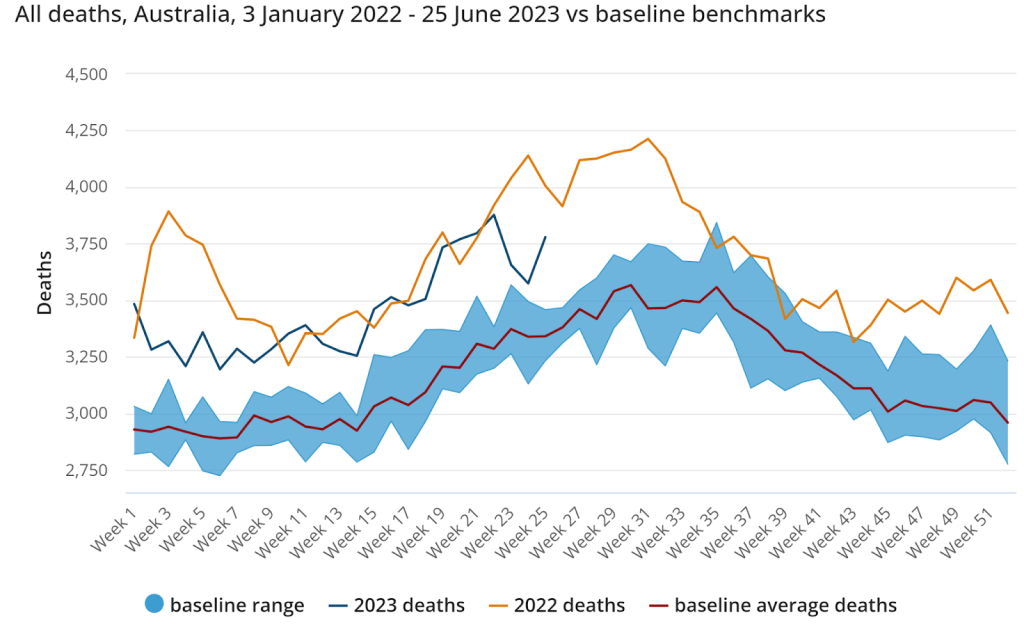
Overall there were 17,900 South Australians who had a cardiac emergency in 2021 compared to 13,250 in 2018, a 35% increase (Fig 16). The vaccine must clearly be the No.1 suspect in this, and it cannot be dismissed as a coincidence. Australian mortality has increased from early 2021 and that increase is due to cardiac deaths.
These excess deaths are not due to an ageing population, because there are fewer deaths from diseases of old age. These deaths are not an effect of covid because they happened in places that covid had not reached. They are not due to low statin prescriptions or undertreated hypertension, as Chris Whitty suggested, because prescriptions did not change and any effect would take many years and been very small. The prime suspect must be something that was introduced to the population as a whole, something novel. The prime hypothesis must be the experimental covid-19 vaccines. The ONS published a dataset of deaths by vaccinated and unvaccinated. At first glance, it appears to show the vaccines are safe and effective. However, there were several huge problems with how it presented that data. One was that for the first three-week period after injection, the ONS claimed there were only a tiny number of deaths — the number the ONS would normally predict to occur in a single week. Where were the deaths from the usual causes? When this was raised, the ONS claimed that the sickest people did not get vaccinated and therefore people getting vaccinated were self-selecting for those least likely to die. Not only was that not the case in the real world, with even hospices heavily vaccinating their residents, but the ONS’s own data showed that the proportion of sickest people was equal in the vaccinated and the unvaccinated groups. That inevitably raised serious concerns about the ONS data presentation. There were so many problems with the methodology used by the ONS, that the Statistics Regulator agreed that ONS data could not be used to assess vaccine efficacy or safety. That tells us something about the ONS.
Consequently, HART asked the UK Health Security Agency to provide the data it had on people who had died and therefore needed to be removed from its vaccination dataset. That request has been repeatedly refused, with excuses given including the false claim that anonymising the data would be the equivalent of creating it even though there is case law that anonymisation is not considered the creation of new data. I believe that if this data was released, it would be damning.
Was it all worth it?
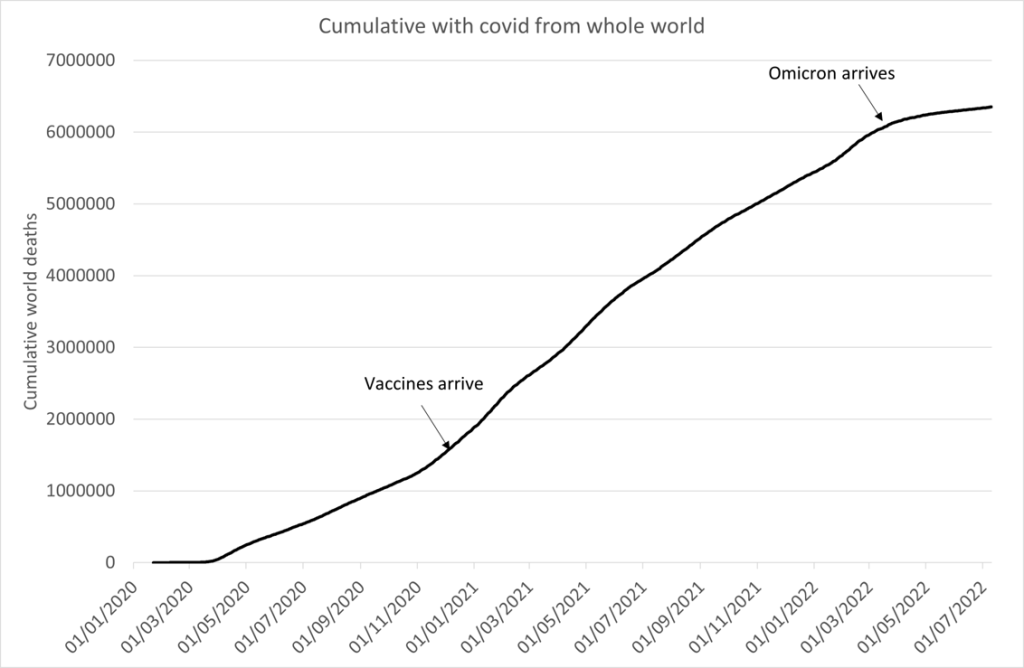
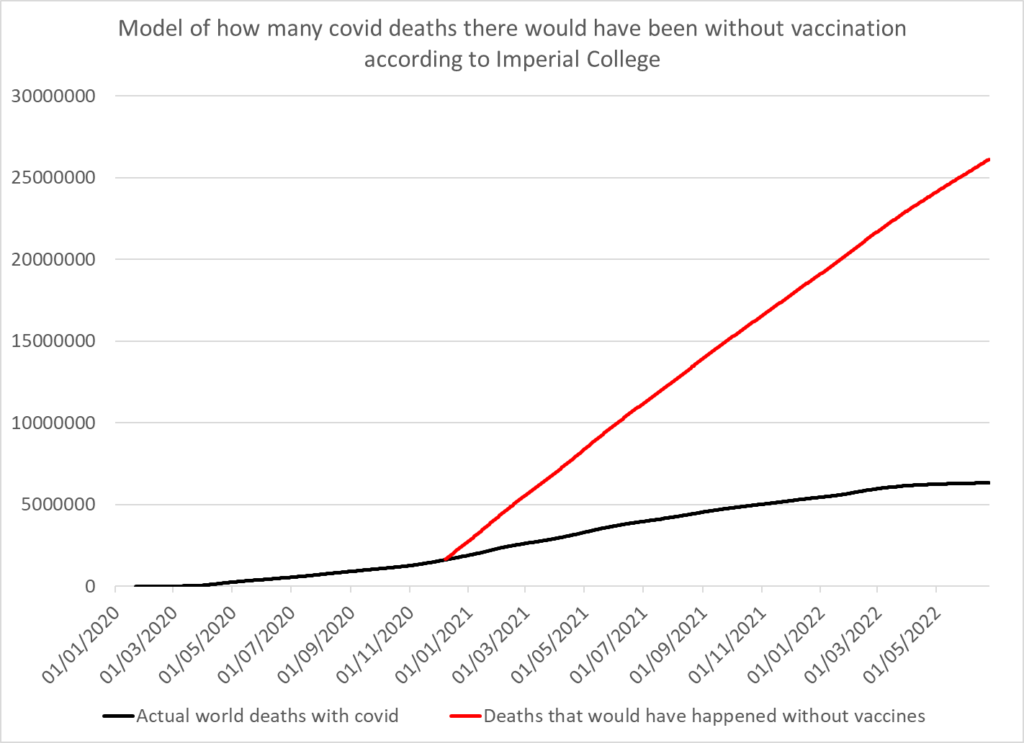
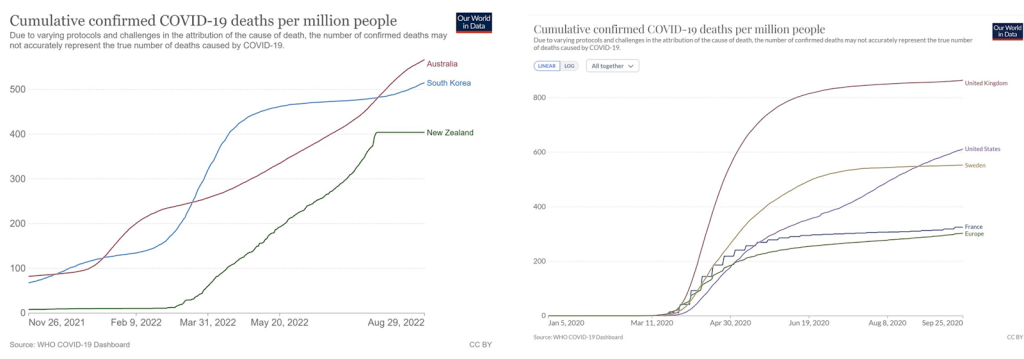
Some claim that so many lives have been saved that any amount of harm, suffering and death caused by the vaccines is a price worth paying. They are delusional. The claims of 20 million lives saved was based on now discredited models which assume that covid waves do not peak without intervention. There have been numerous waves globally now that demonstrate that is not the case. It was also based on there having been more than half a million lives saved in the UK. That is more than the worst-case scenario predicted at the beginning of the pandemic. For the claim to have been true, the rate at which covid killed people would have had to take off dramatically at the beginning of 2021 in the absence of vaccination. That is a ludicrous claim and it bears no relation to the truth (Figs 17 and 18).
In the real world, Australia, New Zealand and South Korea had a mortality rate of 400 deaths per million up to summer 2022 when they were first hit with Omicron. How does that compare? With the Wuhan strain, France and Europe as a whole also had a mortality of under 400 deaths per million up to summer 2020. Australia, New Zealand and South Korea were all heavily vaccinated before infection, so tell me: where was the benefit? The UK had just over 800 deaths per million up to summer 2020, so twice as much – but we know Omicron is half as deadly as the Wuhan variant. The death rates per million are the same before and after vaccination. So where were the benefits of vaccination (Fig 19)?
The regulators have failed in their duty to protect the public. They allowed these novel products to skip crucial safety testing by letting them be described as vaccines. They then failed to insist on safety testing being done in the years since the first temporary emergency authorisation. Even now, no-one can tell us how much spike protein is produced on vaccination and for how long — yet, another example where there is no data for me to share with the House.
When it comes to properly recording deaths due to vaccination, the system is broken. Not a single doctor registered a death from a rare brain clot before doctors in Scandinavia forced the issue and the Medicines and Healthcare products Regulatory Agency (MHRA) acknowledged the problem. Only then did these deaths start to be certified by doctors in the UK. It turns out the doctors wee waiting for permission from the regulator and the regulator was waiting to be alerted by the doctors. This is a lethal circularity. Furthermore, coroners have written Regulation 28 reports highlighting deaths from vaccination to prevent further deaths, yet the MHRA said in response to a freedom of information request that it had not received any of them. The systems we have in place are clearly not functioning to protect the public.
The regulators also missed the fact that in the Pfizer trial, the vaccine was made for the trial participants in a highly controlled environment, in stark contrast to the manufacturing process used for the public roll-out, which was based on a completely different technology. Just over 200 participants were given the same product that was given to the public, but not only was the data from these people never compared to those in the trial for efficacy and safety, but the MHRA has admitted that it dropped the requirement to provide this data. That means there was never a trial on the Pfizer product that was actually rolled out to the public, and that product has never even been compared to the product that was actually trialled.
The vaccine mass production processes use vats of Escherichia Coli and presents a risk of contamination with DNA from the bacteria, as well as bacterial cell walls, which can cause dangerous reactions. This is not theoretical; there is now sound evidence that has been replicated by several labs across the world. The mRNA vaccines were contaminated by DNA, which far exceeded the usual permissible levels. Given that this DNA is enclosed in a lipid nanoparticle delivery system, it is arguable that even the permissible levels would have been too high. These lipid nanoparticles are known to enter every organ of the body. As well as this potentially causing some of the acute adverse reactions that have been seen, there is a serious risk of this foreign bacterial DNA inserting itself into human DNA.
Will anyone investigate? No they won’t.
What will it take to stop these products?
Their complete failure to stop infections was not enough; we all know plenty of vaccinated people who have caught and spread covid.
The mutation of the virus to a much weaker variant— omicron— was not enough.
The increasing evidence of serious harms to those of us who were vaccinated was not enough.
And now the cardiac deaths and deaths of young people are apparently not enough either.
It is high time these experimental vaccines were suspended and a full investigation into the harm that they have caused was initiated. History will be a harsh judge if we do not start doing evidence-based medicine. We need to return to basic science and basic ethics immediately, which means listening to all voices and investigating all concerns.
In conclusion, the experimental covid-19 vaccines are not safe and are not effective. Despite there being only limited interest in the Chamber from colleagues—I am very grateful to those who have attended—we can see from the Public Gallery that there is considerable public interest. I implore all Members of the House, those who are present and those who are not, to support calls for a three-hour debate on this important issue. Mr Deputy Speaker, this might be the first debate on excess deaths in our Parliament—indeed, it might be the first debate on excess deaths in the world—but, very sadly, I promise you it will not be the last.”
Watch the full debate here
