

Four different groups, including HART, requested core particpant status for the UK Covid-19 Inquiry Module 4 on vaccines and therapeutics. This was refused but we were all asked to submit a Witness Statement under Rule 9. When the inquiry hearings were postponed from July 2024 to January 2025, we set up the People’s Vaccine Inquiry and published our statements.
The Module 4 Report was published in April 2026 and our witness statements have still not been published on the Inquiry website. Hence we are reposting them all here on the HART website as a public record of those who spoke out to raise multiple concerns about the safety and efficacy of these products, and the regulatory and ethical failures.
Below is the statment by Dr Clare Craig on behalf of HART.
Module 4 Covid Inquiry: Vaccines and Treatments
Witness Name: Dr Clare Craig
UK COVID-19 INQUIRY
WITNESS STATEMENT OF DR CLARE CRAIG BM BCh FRCPATH
Contents
- EXECUTIVE SUMMARY
- ETHICS
- 2.1. The foundation of medical ethics
- 2.2. First do no harm
- 2.3. Overriding bodily autonomy
- 2.4. Lack of Informed Consent
- 2.5. Politics playing medicine: a very dangerous game
- 2.6. Risk / Benefit analysis was absent
- 2.7. Experimentation on Children
- a. Ethical principles
- b. Risks from covid for children were deliberately exaggerated
- c. Decisions taken were unethical and irrational
- d. Unethical decision making around children is continuing
- 2.8. Experimenting on pregnant women
- 2.9. Coercion
- 2.10. Mandates
- 2.11. Misrepresentation of the nature of covid gene therapies
- 2.12. Misrepresentation of the nature of covid gene therapies
- SWINE FLU: A DRY RUN FOR COVID
- 3.1. Use of inappropriate testing
- 3.2. Exaggeration of the threat
- 3.3. Governments decided a vaccine was the solution without waiting for evidence
- 3.4. Vaccine rollout pushed ahead
- 3.5. Reality: there was never a swine ‘flu pandemic
- 3.6. Outcomes of government responses
- 3.7. Recorded vaccine harms
- 3.8. Tamiflu anitviral drug
- 3.9. Reports and Inquiries to prevent a repeat of the mistakes
- BLOCKED MEANS OF ERROR CORRECTION
- 4.1. Institutional capture
- 4.2. Media capture
- 4.3. The Capture of Medical Journals by Pharmaceutical Interests
- 4.4. Weaponization of the Medical Profession
- 4.5. Regulatory capture
- 4.6. Pharmaceutical companies put profits before patients
- REGULATORY FAILURE
- 5.1 Introduction
- 5.2 Allowing the classification of gene therapies as “vaccines”
- 5.3 Failing to understand where the mRNA went and how long it lasted
- 5.4 Allowing the use of toxic lipid nanoparticles in an mRNA platform
- 5.5 Allowing the use of whole spike protein
- 5.6 Allowing approval of one product based on data from another product
- 5.7 Quality of the products
- 5.8 Differences between the process 1 and process 2 products
- 5.9 DNA contamination
- 5.10 Failure to insist on a submission for the molecule in question
- 5.11 Failure to understand which proteins would be produced by the body
- a. Measuring the size of proteins produced
- 5.12 Reducing the regulatory bar even further since original approvals
- a. Antibody levels as a surrogate
- b. Children’s trials
- i. 12 year olds and over
- ii. 5-11 year olds
- iii. Under 5 year olds
- iv. Moderna Bivalent booster
- c. Pfizer/BioNTech BA1
- d. Moderna BA.4/BA.5
- e. Pfizer BA.4/BA.5 booster
- 5.13 No insistence of thorough safety testing in trials / obliteration of the Control Group
- 5.14 Assumption that all safety issues would be evident within a few days of vaccination
- 5.15 Ignoring alerts from systems designed to spot safety problems
- 5.16 Ignoring anomalies in trial safety data
- 5.17 Allowing the destruction of the control arm ruining proper safety assessment
- 5.18 Failing to withdraw the vaccines on safety grounds
- 5.19 Batch issues
- 5.20 Bias in the covid trials
- a. Causes of bias
- b. Evidence of bias
- c. Failing to pay attention to secondary efficacy results
- d. Hiding waning efficacy in early trial data
- 5.21 Failing to police the marketing of the products
- 5.22 Other regulators
- PROTECTION FROM NATURAL IMMUNITY
- 6.1. Broad immunity
- 6.2.Vaccine versus post-infection immunity
- 6.3. Reinfections
- 6.4. Omicron
- VACCINE EFFECTIVENESS
- 7.1 Different vaccine platforms
- a. Choice of delivery system
- b. Choice of molecule
- 7.2 Benefits
- a. How could these novel products prevent infection?
- b. Changed definition of a case to make vaccines appear beneficial
- 7.3 Importance of what happens in first two weeks
- a. Broad observations
- b. Impact in care homes
- c. Impact overall
- d. Excuses for the problem
- e. Denial of the Problem
- f. Creating an illusion of efficacy
- i. The ‘doubling’ effect of ignoring the first two weeks
- ii. Recurring problem with further doses
- 7.4 False Claim: Vaccinations could defeat the virus and take us back to normality
- 7.5 False Claim: Vaccinations would prevent infection
- a. Number needed to vaccinate to prevent an infection
- b. Using the wrong denominator
- 7.6 False Claim: Vaccinations would protect those around them
- 7.7 False Claim: They had a realistic chance of personal benefit from the injections in terms of a reduced risk from covid
- 7.8 False Claim: Covid vaccination would reduce the risk of hospitalisation
- a. Intensive Care admissions
- b. Hospitalisations for other causes
- 7.9 False Claim: Covid vaccination would reduce the risk of death
- a. Trial Results
- b. Real World results
- 7.10 Misleading Claim: There were fewer deaths per case after vaccination
- 7.11 False Claim: 20 million lives were saved
- VACCINE HARMS
- 8.1 It takes time to do adequate safety testing
- 8.2 Diverse types of harm
- a. Lipid nano-particles
- b. Cell death
- c. Synthetic nucleotides
- d. Small vessel damage
- e. Autoimmune damage
- f. Endotoxin damage
- g. Contaminant DNA
- h. Unknown proteins
- 8.3 Difficulties measuring harm
- 8.4 Adverse Event Reporting Systems
- 8.5 Overall impact
- 8.6 Disability Data
- 8.7 Australia and Singapore: accidental ‘control’ groups
- 8.8 Immune impacts Original Antigenic Sin and Immune switching
- 8.9 Broad categories of harm
- 8.10 Myocarditis and other cardiovascular issues
- a. First indicators of myocarditis / pericarditis
- b. How common was it?
- c. Cases of Myocarditis in the Adverse Event Reporting
- d. Cardiovascular Adverse Events in Post-marketing Surveillance
- e. The Consequences of Myocarditis
- f. Outcome data for viral myocarditis
- g. Outcome data for post vaccine myocarditis thus far
- h. Post-mortem evidence
- i. Did covid cause myocarditis?
- j. Cardiac Arrests
- k. Sudden deaths data in trial
- l. Unexplained excess deaths
- m. Atherosclerosis
- 8.11 Deaths
- a. Problems with systems for highlighting increased deaths
- b. Investigating Deaths
- c. Excess Mortality
- d. Lack of Deficit
- e. Reasons for excess deaths
- 8.12 Fertility
- 8.13 Long Covid, or ‘Long-Vaccine’?
- TREATMENTS
- UNEXPLAINABLE TIME LINES
- 10.1. Previous outbreaks of unusual pneumonia did not lead to a similar response
- 10.2. Premature response in early 2020
- 10.3. Choice of vaccine molecule
- 10.4. Timeline issues regarding Swine Flu
- FURTHER INVESTIGATIONS REQUIRED
- STATEMENT OF TRUTH
Health Advisory and Recovery Team
I am submitting this witness statement in my role as Co-chair of the Health Advisory and Recovery Team, HART and as a qualified doctor and diagnostic pathologist. HART is a membership association made up of volunteer doctors, healthcare professionals, statisticians, scientists and other experts who have had concerns regarding covid related policy. We formed as a group in January 2021 to present our concerns as a body of professionals and to also allow us to share information, debate and learn from each other. No one in HART thought we would still be working on this over three years after we first started. Personally, I have worked full-time, unpaid, gathering evidence since August 2020. I have no conflict of interest.
1. EXECUTIVE SUMMARY
Not a single member of the British public who received a Covid-19 injection was able to give fully informed consent. The risks were censored, the benefits were falsified and it all occurred under state and corporate coercion. Every single dose administered was a breach of medical ethics and amounts to medical malpractice at a population level. This may seem like an extreme place to start, but it is the evident truth.
The enormity of the lies now firmly embedded in the collective public consciousness are so multi-layered that it is hard to know where to start in dismantling them. It is almost impossible for an accurate account of the vaccine roll-out to be understood without investing time in unpicking each falsehood relating to the supposed justification for their existence in the first place.
The human desire to leave trauma and unhappiness in the rearview mirror and ‘just get on with life’ is another challenge we face. Unless we are prepared to realise and accept the extent of what was enacted on an unsuspecting and trusting public, history is destined to repeat itself. We must sit with ideas that are extremely unsettling and yet are provable with the evidence in front of us. We must admit to ourselves and publicly that we were played. Numerous mechanisms for error correction which are essential to democracy were broken. As well as a total failure of political opposition, there has been widespread media capture, regulatory capture and scientific institutional capture along with silencing of concerned experts on a scale that is completely mind-boggling. Consequently the truth has been hidden. Without this recognition, we cannot hope to present a true account of the events that have occurred.
It is not a stretch to say that certain pharmaceutical companies can behave in a criminally negligent and fraudulent way. This is a matter of fact when one considers previous lawsuits and fines that have been paid. Why then, is it a stretch to think these corporations have employed the same modus operandi in 2020? When drugs have caused harm in the past the profits have dwarfed the fines from later prosecution. Giant multinationals have learned the legal loopholes to ensure they hold no accountability for rushed-to-market products should harms become apparent. All gain, minimal risk, whatever the collateral damage to the population. It is worth reflecting on the opiate crisis in the USA when examining the details of the covid vaccine roll-out. Why is it beyond the imagination of most to think that a similarly criminal story may have been deployed? Why let a good crisis go to waste, as the saying goes?
One could argue endlessly about the intricacies of covid vaccine efficacy, vaccine harms, clinical trial data, risk analyses, mortality data and so forth. However, in the final analysis the only point that needs to be emphasised in this module is that the roll-out and media coverage of the covid injections was an ethical catastrophe from start to finish. Unless this point is documented by this inquiry and is fully understood by the public, the unconscionable response that favoured only the pharmaceutical industry will be repeated. The full collateral damage remains unknown as there is no appetite by the world’s governments to investigate outcomes in a meaningful way. As the saying goes, you will not find what you do not seek.
As evidence of harm slowly gathers, claims have been made that the population-level benefit outweighed the risk, meaning the harm caused was “worth it for the greater good.” Leaving aside the questionable ethics of this approach this is demonstrably not true. Multiple sources including SAGE, PHE and the ONS as well as many independent scientists reported on an increased infection risk in the period within two to three weeks of vaccination. The result of this increased risk is to create a statistical illusion. The data showed that people were becoming infected earlier rather than later in a wave following vaccination. By ignoring the first two weeks after vaccination and labelling these individuals as ‘unvaccinated’ for this time-period (claiming the vaccine couldn’t be ‘working’ yet so they still are classed as unvaccinated) the illusion of benefit was created in paper after paper. The big picture impact on the population as a whole showed that the claimed benefits did not exist. The lack of benefit confirms the fraud from the clinical trial data, reinforces the lack of informed consent and means every harm outweighed the benefit at an individual level.
Around 10% of the population were infected in each wave in a predictable manner as happens with influenza. The duration and intensity of each wave is comparable before and after vaccination. However, since the arrival of the far more mutated Omicron variant in 2022, which tends to remain in the upper airways, the intensive care admissions and deaths associated with each wave have reduced. This reduction was unrelated to interventions that preceded Omicron.
When someone has a high risk of dying the evidential bar required to justify a treatment is lower than for a healthy population for whom any benefit will necessarily be much smaller. However, treatments that showed promise with an excellent safety record were discredited and their advocates smeared. Research papers with design flaws that gave the impression of problems with safe drugs were published. These papers received disproportionate air time. When systematic reviews have been carried out to look at the whole breadth of the evidence these flawed studies skewed the results due to their size.
The medical regulator has failed the public in numerous ways from issuing temporary use authorisations on inadequate evidence, failing to demand such evidence subsequently and utterly failing to ensure communication of the uncertainties to the public. Instead of demanding a firmer evidence-based approach as the perceived crisis diminished, they in fact lowered the evidential threshold for children and for booster roll-outs. Furthermore, they were integral to the failure to adopt drugs with an established safety record that would have been useful as early treatments.
PCR testing (covered in my previous witness statement) is one of the lynch pins on which the falsehoods were built and yet remains to this day unchallenged by mainstream press and the medical community. These tests were knowingly misused to create as many ‘covid’ cases as possible for the daily podium theatre. This in turn gave the false impression of a horrific disease ‘ripping’ through society like wildfire leading to the next entirely false assumption that something extraordinary must be done!
The amplification of PCR viral detection methods were so extreme that they would inevitably create an inordinate amount of false positives. Extensive testing in hospitals, where people have a lower immune defence, would lead to high numbers of people sick with other conditions testing positive and high numbers of the dying testing positive. The speed at which the covid PCR test was brought to market raises serious questions about the peer-review process employed and yet this solitary test, devised in a matter of days and never refined or updated, is the cornerstone of the entire skewed global dataset.
Looking at the events of the last few years through a PCR lens gives a totally different impression to examining what happened using other existing measures of public health, such as people with symptoms of disease. It is fundamentally important that the inquiry understand how PCR testing was abused and we must prevent such abuse from happening in future. We should ask ourselves, without the barrage of clinically irrelevant PCR data and media hype, what would we actually know? This test, in conjunction with endless statistical ‘modelling’ has made a farcical circus of meaningless data with meaningless assumptions paving the way for extremely harmful policies to be rolled out. This point needs to be underscored because as you will read further in the document, this precedent using PCR and modelling data had already been set during the Swine flu debacle of 2009. When you read the account, we hope you will be struck by the stark parallels that have played out in 2020.
Data that could easily serve to answer fundamental questions about the vaccine was either never released to the public or stopped being released once it was clear that what it showed exposed falsehoods in the official narrative. Inevitably the evidence presented here will therefore be curtailed by the decisions to hide important data.
The media sold a story and created an immense degree of fear within the population. Trying to form a rational view about what happened through a lens of fear will always fail. In a real emergency, it would be the job of those in charge to quell fear to ensure that responses remained as rational as possible. Instead, our governments chose to ‘ramp it up’, using government-funded behavioural science units. This was unethical in the extreme. The psychological harms caused by this relentless (and expensive) fear campaign will be felt for generations to come.
Continuing to talk about a ‘pandemic’ needs to stop because there is no evidence that there was one (by any conventional definition), when one considers the all-cause mortality from 2020. And if there was no pandemic, there was certainly no need to rush a novel medical product to market and attempt to inject it into the arms of every man woman and child. The term “pandemic” was altered in recent years by the WHO to remove the requirement for many deaths in young people. In its current iteration the word can be repeatedly applied and abused whenever a mutation of a virus is detected. If a ‘pandemic’ doesn’t cause mass deaths, what threat does it pose? It is a meaningless label, designed to cause fear and make people accept the unacceptable because of the ‘emergency’. A normal seasonal pattern can then be weaponized to benefit the pharmaceutical industry. That is certainly the reality of what has happened, whatever the intention may have been.
The narrative running through the inquiry so far is a carefully rehearsed rendition by the perpetrators that everything done was legitimate and should simply have been done sooner and with more vigour. This is a 180° inversion of the truth. Doing nothing out of the ordinary to treat a passing respiratory virus would demonstrably have caused less harm and would have resulted in far fewer deaths, let alone the catastrophic impact on the economy which measurably affects population health outcomes.
I will end this summary with a quote from Tom Jefferson, an Oxford epidemiologist commenting on the Swine Flu debacle of 2009:
“Sometimes you get the feeling that there is a whole industry almost waiting for a pandemic to occur. The WHO and public health officials, virologists and the pharmaceutical companies. They’ve built this machine around the impending pandemic. And there’s a lot of money involved, and influence, and careers, and entire institutions! And all it took was one of these influenza viruses to mutate to start the machine grinding.”
2. ETHICS
2.1 The foundation of medical ethics
| Decisions made in the name of covid prevention have drastically undermined medical ethical principles and human rights, once deemed foundational and immutable. Disregarding them in a crisis undermines their status. They are principles and rights specifically designed to protect against possible abuses in the event of a perceived ‘crisis’. Acknowledgment and rectification of such breaches are necessary to prevent recurrence. |
2.2 First do no harm
A core medical ethical principle is to first do no harm. This principle was inverted and used to justify interventions rather than to ensure caution before doing anything at all. Doing nothing at all is a perfectly legitimate course of action when the alternative carries great risks of harm.
Trust in medicine requires that people are confident that doctors have at heart the best interests of the individual patient in front of them and are free to make those decisions using their professional and ethical judgement, without entertaining thoughts of the so-called “Greater Good”.
2.3 Overriding bodily autonomy
The Universal Declaration on Bioethics and Human Rights affirms that “the interests and welfare of the individual should have priority over the sole interest of science or society” (Article 3). This was clearly and repeatedly breached during the last few years. The requirement for full informed consent before administering any medical intervention, as laid out in international law and guidance from medical regulators,was also breached as described below
Bodily Autonomy is the inherent right of every individual to make their own decisions about their body, without interference. This includes the right to accept or refuse medical treatment, even when the majority or the experts would make a different choice. A person has every right to believe that they would take a personal risk for the benefit of society. They also have every right to try and persuade others of the moral superiority of that position. However, manipulation or coercing others who have a different opinion on the morality of the situation cannot be justified.
If we relinquish bodily autonomy, we have truly surrendered all of our power to the state. This is exactly what happened here in the UK in 2021.
GMC guidance states that:
“You must respect patients’ right to reach decisions with you about their treatment and care. You must not make assumptions about the decisions patients are likely to make, or try to influence their decisions by the use of authority, inducement or pressure.”
The government overrode GMC guidance under the pretext that it was invalid ‘under the circumstances’. There are no circumstances in which bodily autonomy can be overridden at a population level by the state.
There needs to be a clear acknowledgement by the Covid Inquiry that bodily autonomy was disregarded and, on the record, an assurance that it will never, ever happen again in future ‘pandemics’.
2.4 Lack of Informed Consent
There has been no acknowledgement that informed consent was absent during the vaccine roll-out. Worse still, it was replaced with coercion and financial incentives. A page entitled More leading businesses join vaccine uptake drive shamelessly remains on the government website.
“No jab, no job” mandates and financial incentives like pizza, cash prizes and travel vouchers obliterated the possibility of informed consent.
Social incentives were also deployed, with the use of celebrities telling people to ‘get their jab’ which is explicitly disallowed in regulations (see section 5.7 on MHRA blue guide).
Tactics designed to pressure and manipulate individuals removed their ability to evaluate risks and benefits without prejudice. A shocking example of this is the government-funded ‘can you look them in the eyes?’ advertising campaign.
In October 2020, before any approvals, WHO behavioural scientists suggested pressuring people with the idea they were protecting others and said, “putting emphasis on the economic benefits, such as being able to stay in the workforce and provide for one’s family, might also encourage vaccination.” In December 2020, the NHS partnered with the nudge team to find ways to persuade and threaten people. Their advice included coercing young people with a promise of “getting your life back” and “focusing on the potential regret” if they infected a loved one.
An NHS letter sent to 16-17 year olds gave four reasons to get vaccinated including being able to go on holiday, to sporting events, to festivals and to “enjoy recently restored freedoms and avoid further lockdowns.” While it is honest not to claim any potential benefit for this age group, this wording is not informed consent, it is coercion.
Psychotherapist, Dr Christian Buckland states that:
“using psychological pressures to change people’s behaviours without their knowledge not only [resulted in] all the harm [from] e.g. suicide rates, mental health problems …but it also invalidated everyone’s ability to give consent to the covid jab.”
The use of the word vaccine led people to expect a product that would be entirely safe and effective (or, at worst, to have a safety profile similar to previous products characterised as “vaccines”) and no caveats were given as to the uncertainties in this case. Furthermore, the truth that these were in fact gene therapies was not mentioned at all.
People will rightly weigh a catastrophic risk, such as dying or becoming permanently disabled differently to a less serious and temporary adverse reaction, yet all were bunched together as ‘rare’ and dismissed, if they were even mentioned at all. In many cases people were simply told they might just get ‘a sore arm for a bit’.
GMC “Good Medical Practice” states doctors “must work in partnership with patients, sharing with them the information they want or need in order to make decisions about their health” and that they must “listen to, and respond to, their concerns and preferences.”
The document specifies that patients must be informed of “the potential benefits, risks of harm, uncertainties about and likelihood of success for each option, including the option to take no action.” Doctors have an obligation to inform patients on known risks, uncertain risks, and “any risk of serious harm, however unlikely it is to occur.”
The Green Book, which is the UK government’s vaccine guidance, states, “For consent to immunisation to be valid, it must be given freely, voluntarily and without coercion.” What counts as coercion? The Encyclopaedia Britannica defines coercion as the use of threats or punishments to force certain actions including “economic sanctions, psychological pressures, and social ostracism.”
WHO said, “if the default in schools is to vaccinate all students, with the provision of allowing those who object to opt out, then vaccination rates will likely be higher than if the default is to provide vaccination only to those who opt in.” Informed consent requires an opt in process.
None of the covid vaccines were given with what could be described as “fully informed consent”. One particularly egregious example of this can be seen in respect of the Moderna vials. These were distributed in boxes of ten, and rather than having an information leaflet per dose there was a single leaflet in the box. It was a large piece of paper folded multiple times and the only words on it were “intentionally blank.” There cannot be informed consent without information.
The NHS consent form did not say anything about unknown side effects nor did it specify any expected adverse reactions, merely stating: “Please read the product information for more details on the vaccine and possible side effects by searching Coronavirus Yellow Card.” This approach was reckless in the extreme for an entirely novel medical product.
Nadhim Zahawi recognised the importance of consent when he said in February 2021, “Vaccines are not mandated in this country as Boris Johnson quite rightly reminded parliament, “That’s not how we do things in the UK. We do them by consent. We yet don’t know what the impact of vaccines on transmission is and it would be discriminatory… we have no plan of introducing a vaccine passport.”
2.5 Politics playing medicine: a very dangerous game
It is illegal to practise medicine if you are not a medical doctor. It is certainly not something that should be attempted en masse at the population level without seeing the individual patients;
The Government vaccine mandates meant that in effect, politicians were practising medicine. They were putting people in the position where they were forced to take a novel medical product, regardless of their individual circumstances or need, in order to keep their job. This is equivalent to prescribing, or put another way, playing doctor.
The Universal Declaration on Bioethics and Human Rights was completely ignored to combat a virus with what was known at the time to have extremely low lethality, although it must be stressed that even if the lethality was 50% this declaration should never have been overridden.
In its preamble the Declaration states:
“Recognizing that ethical issues raised by the rapid advances in science and their technological applications should be examined with due respect to the dignity of the human person and universal respect for, and observance of, human rights and fundamental freedoms”. This clearly did not happen with regards covid injections.
2.6 Risk / Benefit analysis was absent
When people are healthy, you cannot justify putting them at risk of harm without a full understanding of what the harms are or might be and what is not yet known. The precautionary principle was shattered by the covid injection roll-out.
Mortality was highly age and comorbidity dependent. This was completely misrepresented to the public. When the vaccines were given conditional marketing authorisation, a schedule was produced by the JCVI to prioritise the elderly and vulnerable, with those categories accounting for 98% of deaths in the first wave. This prioritisation was ultimately completely ignored.
The initial campaign was to vaccinate healthcare workers and “those most at risk.” By August 2020, before any trial results, WHO began their vaccine campaign “No-one is safe unless everyone is safe.”
Healthy young people were at negligible risk from covid and any consequences due to vaccine harm can have disproportionately more impact because their quality of life can be reduced for a greater number of potential years of life left.
With specific reference to children, the JCVI (which was unwilling to make a firm recommendation in favour of the vaccines) was overruled when the UK’s CMOs found an artificial justification for offering the vaccines (that school disruption which was caused by government policy would be reduced to the tune of 15 minutes more education per child). Societal benefits were prioritised over children’s health. They could not possibly benefit from the vaccine so taking it only ever represented risk to them. This is unethical in the extreme. Experimentation on children is abhorrent and yet this is exactly what happened. The full extent of the damage remains unquantified.
Children’s Campaign group UsForThem took Pfizer to the pharmaceutical marketing regulator after their CEO (Bourla) said the following prior to approval of the vaccine for 5-11 year olds “So there is no doubt in my mind that the benefits, completely, are in favour of doing it.” Pfizer was found guilty by the tribunal of misleading the public but Molly Kingsley was “asked by the UK regulator not to discuss the case until the appeal process was final. That took over a year, in which time the C19 jab roll-out to that age cohort proceeded.” In other words, the victory was meaningless as they were effectively gagged until after the roll-out to children.
NHS GPs were paid depending on who they injected with almost double payments in August 2021 for injecting a child aged 12-15 years. This amounts to financial incentivisation. The Financial and commercial arrangements and conflicts of interest section on the GMC website states “you must not ask for or accept – from patients, colleagues or others – any inducement, gift or hospitality that may affect or be seen to affect the way you prescribe for, treat or refer patients or commission services for patients.”
2.7 Experimentation on Children
a. Ethical principles
Adults should protect children, not vice versa. The UN Convention on the Rights of the Child dictates special safeguards and legal protection for children due to their physical and mental immaturity. All signatories have an obligation to uphold this. International law precludes giving experimental drugs to those without capacity to consent unless there will be a direct benefit;
Proposing children receive covid ‘vaccines’, despite being at statistically zero risk from the disease and while the products were still in phase 3 trials, in order to shield adults contravenes this principle. Never before has anyone suggested that it is acceptable to test novel medical products on pregnant women and children and yet it was done with jaw dropping nonchalance.
On 6 December 2023 it was reported widely that “One in four who had Pfizer Covid jabs experienced unintended immune response’. This kind of finding after the fact starkly illustrates why we should not experiment on children or pregnant women. Safety cannot be known a priori.
The decision making process which led to vaccinating children against covid-19 raises many concerns. In February 2021, Oxford University was advertising for children to join a trial of AstraZeneca at a time when there was almost no adult safety data. When this was queried with Professor Pollard, he replied, “I certainly agree with you that we are yet to establish the safety and immunogenicity of the vaccine in children and for this reason the parents and children/young people are fully informed before taking part in the trial about what is and isn’t known about the vaccine.” Less than a month after the first children were immunised, AZ was suspended in Denmark following the death of a young adult with blood clotting complications. Two months later it was discontinued in the UK for under 40s.
In June 2020, Professor Peter Openshaw in a Lord’s committee said about vaccinating children, “Sometimes it is possible to protect a vulnerable group by targeting another group.” By 2021 Members of SAGE and of JCVI were openly briefing that the vaccine should be rolled out urgently to children as soon as the adult programme was complete in order to prevent ‘upward transmission’ to vulnerable groups. In February 2021, SAGE member Professor John Edmunds was telling Andrew Marr on BBC, that “we can all spread the virus, and so until we’ve all been vaccinated and I include children here, then there is going to be a significant risk of a resurgence … I think there’s an argument for turning to children as fast as we can”.
A group of 50 doctors and academics wrote to the MHRA highlighting why it was irrational and not safe to do so. They were ultimately ignored.
b. Risks from covid for children were deliberately exaggerated
The PICANet report on COVID-19 stated that no Intensive Care Unit (ICU) child deaths were “due” to covid but the media reported on this as if all child ICU deaths were due to covid.
The case of Ismail Mohamed Abdulwahab 13 was the peak of this. He died 30 March 2020 after ‘testing positive’ for Covid-19 but in fact died of a breathing tube placed incorrectly. His story was used as propaganda to scare parents into believing covid was a risk for their child.
Worrying ‘educational materials’ were being used in London schools from April 2021, with graphic pictures of children with smallpox, tetanus and polio implying a similar threat to children from covid. There followed a slide saying “when can I get my covid vaccine?” These were endorsed by the National Education Union.
Omicron infected a large number of children in a short period and that included children who were in hospital at the time. Some groups used this to claim that Omicron was not mild in children but that was not the case.
The USA witnessed an algorithmic error that removed over 77,000 deaths from the covid tally, reducing child deaths labelled as due to Covid by 24%, after those numbers were used to promote child ‘vaccination’.[ii] People in the UK were exposed to this propaganda from the USA through social media.
c. Decisions taken were unethical and irrational
The statistical risk of death in a child was 0.0%. In the absence of potential benefit the possible outcomes were neutral or harm. Child safeguarding requires that adults prevent potential harm to children and the decisions made over covid vaccination in children can be viewed as a multilayered child safeguarding failure.
In May 2021, the MHRA granted a conditional marketing authorisation for 12-15-year-olds, based entirely on trial data from Pfizer who had studied only 1131 vaccinated children followed for 2 months. This is totally inadequate for an assessment of safety of a novel medical product.
In July, the JCVI looked at real world data from Israel and the US, whose children’s programme had already begun. They made a decision not to recommend its use in under 18s on the basis that the benefit risk balance was much too narrow and concerns regarding as yet unknown long term harms.
Two days after this announcement, the CMO asked the JCVI to hold an emergency meeting to reconsider their decision. The minutes of these meetings show several members voicing concerns particularly about myocarditis and the lack of follow-up of affected children.
By September 2021, it appears the political pressure was too great and they passed the decision to the CMOs. This is highly irregular.
Jeremy Hunt later said to the chair of the JCVI, “You refused to make that judgement even in September. In the end, we had to do a workaround using the chief medical officers.”
The “workaround” involved asking the CMOs to jointly create a justification based on “broader benefits” for the vaccination which was then used as political “cover” for going ahead with the programme in the absence of a firm JCVI recommendation.
The subsequent decision by the CMOs to recommend vaccination of adolescents was based on a modelling of reduced school closures. It equated to 15 minutes per pupil. This took no account of any school time lost due to the vaccination procedure itself (15 minutes is required to wait after a vaccine) let alone any vaccine side effects.
d. Unethical decision making around children is continuing
The NHS was still advertising in late 2023 for children to be vaccinated to help protect vulnerable and elderly family members, despite the known continuing infection rates after multiple boosters and despite higher rates in people with more doses. One in every £7 spent on marketing the covid vaccines was spent on advertisements for children. I was told of doctors who decided not to vaccinate their own children but continued to oversee vaccination of other people’s children.
Figure 1: Tweet from Department of Health and Social care suggesting vaccination of children to protect adults
Guidance given to doctors continues to include vaccinating healthy children if they live with a vulnerable adult.
2.8 Experimenting on Pregnant Women
Between March and May 2020, there were eight deaths of recently pregnant women said to be due to covid with ten deaths “with covid.” Of these ten, two were obese, three were drug users and only one was a white European ethnicity. The national audit on maternal deaths noted, “impacts of pandemic-related service changes have been noted in several chapters reporting on the care of women who died from other conditions.” It would be odd to believe that these impacts did not also affect the care given to women who died with a covid positive PCR test result.
By the end of 2020 the number of pregnant women who had a death said to be due to covid was only nine – i.e. there was only one further death for all of June 2020-December 2020 prior to vaccine rollout.
In 2020, 9 pregnant (or recently pregnant) women had deaths attributed to covid. If a miracle vaccine could prevent every one of those maternal deaths (some of which were complications of other issues) then 57,000 women and 57,000 unborn babies would need to be exposed to the vaccine. For an individual woman making a decision about a vaccine the chance of her benefiting would be 0.002%. It is totally unethical to expose pregnant women and their unborn babies to a novel therapeutic agent with inadequate safety data (and zero long-term data) when they only have a 0.002% chance of benefiting from it.
Before 2020, one in five pregnant women in intensive care were there because of pneumonia. Pre-covid one in every eleven maternal deaths were attributed to influenza. The picture is slightly complicated by the fact that women in respiratory failure, in intensive care may well test positive for a virus that is circulating in the air when the testing is set up to describe a single aerosol containing a handful of virus particles as positive as it was (see previous witness statement in module 3).
In England, in the 12 months up to April 2021 there was on average one obstetric death per month with eight deaths in the eight months leading up to April 2021. Strikingly seven of these eight women were from ethnic minorities. Three of them were drug users. None of them were treated with antivirals or other therapeutic drugs. These points were never communicated to the public, preventing informed consent. However, over the subsequent eight remaining months of 2021, before Omicron arrived, the death rate doubled to sixteen deaths per month. The rise was blamed on the Delta variant without a serious investigation as to whether these novel agents could be to blame.
For intensive care admissions the pattern was the same. In the period up to April 2021, before vaccination in pregnant women, there were 1.3 covid intensive care admissions of pregnant women per day across the country. From May to September 2021, during the vaccination campaign, this rose to 2.4 women per day.
In Scotland, the total number of pregnant women admitted to intensive care for any cause was 20 in 2019 and 25 in 2020. However, in 2021 it rocketed to 57.
On 11th October, NHS England said, “One in five of the most critically ill COVID-19 patients in the UK are unvaccinated pregnant women.” and this hit the headlines. They were referencing a total of 18 pregnant women who had lung bypass treatment since July 2021.
Up to March 2021 ten maternal deaths were attributed to covid. Four deaths of women with covid were actually due to delayed access to healthcare, “A woman had a cough for several days in late pregnancy but was anxious about attending hospital due to fear of COVID-19. She died at home without any contact with healthcare services. Two further women with severe COVID-19 symptoms declined admission to hospital initially and were critically unwell when they were admitted a few days later. Both died from COVID-19 pneumonitis. A fourth woman did not access any antenatal care due to concerns over COVID19 and died after giving birth at home.”
Although the official data claimed the intensive care admissions were all “unvaccinated” the UK’s Intensive Care National Audit & Research Centre defined “unvaccinated” as “Either no linked vaccination record in NIMS or first dose of vaccine received within 14 days prior to the positive COVID-19 test.” All failures to record a vaccine would be counted as unvaccinated regardless of what the families said or what was in the medical notes. Furthermore, during the first 14 days numerous cells in the body start producing spike protein and the immune system is so occupied with this that the white blood cells levels in the blood plummet. People are more susceptible to all viral infections in this period from cytomegalovirus, Epstein Barr virus, herpes zoster virus, herpes simplex virus and SARS-CoV-2. There needed to be proper analysis and investigation of pregnant women admitted during this period and it was not done. Instead, any women sick during this period were classified as unvaccinated which could have created the illusion that being unvaccinated was more of a risk than it was and that being vaccinated provided more protection than it did.
Before giving any drug in pregnancy, even to see whether or not it is safe, it must have an exemplary record for safety in other settings.
A study on Pfizer/BioNTech’s COVID-19 vaccine reported significant pre-implantation losses in rats, akin to early miscarriages. The loss rate was 9.8%, over double compared to the control and also nearly twice as much as an alternative spike molecule that was also tested. The report, which focused on the effects of the vaccine on 44 rats, also observed more than three times the foetal abnormalities in vaccinated rats compared to unvaccinated ones and more than double compared to the alternative spike molecule.
Despite these alarming findings, rather than addressing the safety concerns directly, the researchers and Pfizer opted to compare their outcomes to historical data from other rat studies. They used the highest previously recorded rate as a benchmark to claim their results weren’t unusual.
In May 2021, regulators let Pfizer reduce the size of their clinical trial from 4,000 pregnant women to less than 10% of that. Even then they did not report the outcome of 12 of the births. There was one stillbirth among the vaccinated women. No one can say for sure whether that was bad luck or a risk of 1 in 400. That’s why it was so important to do a properly sized trial in the first place.
For pregnant women with a covid admission the risk of having moderate to severe covid or an intensive care admission was lower in the vaccinated but not by a meaningful amount. For example if 300 pregnant women were admitted with covid then 3 would end up on intensive care if they were all unvaccinated compared to 1 if they had had two doses. Therefore, even among those who actually caught covid, 150 women would need to have two doses to prevent a single intensive care admission.
Figure 2: Moderate or severe covid and intensive care admissions as a percentage of covid admissions by vaccine status from data in BMJ
Consent forms for a trial on the Pfizer/BioNTech booster dose in children in 2022 stated, “If your daughter is pregnant, planning to become pregnant or is breastfeeding a baby, she cannot be in the study as there may be risks to the unborn baby or nursing baby. Nobody knows what these risks are right now.” The company had said nothing in public while there was an ongoing campaign to encourage pregnant and breastfeeding members of the public to take these doses.
Two babies were reported to have died after strokes when they had been exposed through breastmilk. These deaths were not included in the EU safety cohort because the exposure was “indirect”.
The original advice in December 2020 was to consider vaccination in pregnancy where “risk of exposure to Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV2) infection is high and cannot be avoided or or where the woman has underlying conditions that put them at very high risk of serious complications of COVID-19. In these circumstances, clinicians should discuss the risks and benefits of vaccination with the woman, who should be told about the absence of safety data for the vaccine in pregnant women.” This carefully caveated strategy, which ensured informed consent, was soon taken over by fear mongering directed at pregnant women which pressured them to vaccinate.
In November 2021, It became a legal requirement for women to take it to continue working in the care sector. This was profoundly unethical.
Pregnant women who had Moderna (which has a higher dose of mRNA) had a 42% higher risk of miscarriage than those who had Pfizer (slide 32). The overall risk seems low because many of these women were past the miscarriage risk period when vaccinated. The rate of induced abortion was 27% higher in those who had Moderna compared to Pfizer. It was not stated how many were for foetal anomalies (slide 32).
The Scottish data showed a clear correlation between vaccines given to pregnant women and subsequent neonatal deaths. There were only small numbers of neonatal deaths in total meaning a thorough investigation should have been carried out. Public Health Scotland started an investigation into 39 deaths but said they had not looked at vaccine status because “it was not possible to identify a scenario that would have resulted in a change to public health policy or practice.” and “had the potential to be used to harm vaccine confidence.”
As a reason not to investigate, fear of vaccine hesitancy is particularly egregious. If the investigation shows there is no link between neonatal deaths and the vaccination status of the mothers, then that surely would reduce ‘vaccine hesitancy’ but if a link is demonstrated then it should result in a vital policy change.
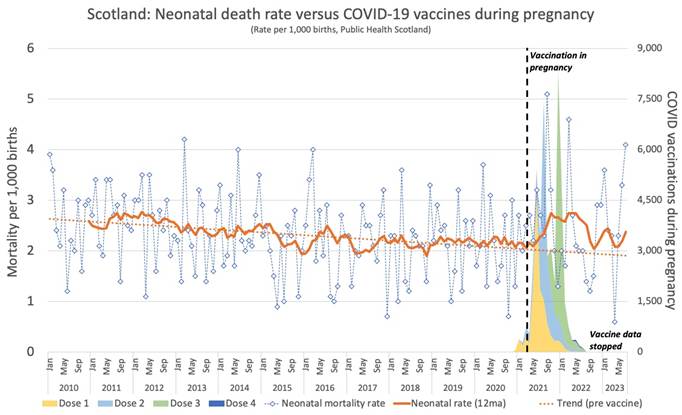
Figure 3: Scottish data showing doses given to pregnant women plotted against neonatal death rate (blue line) showing spikes in deaths with each spike in doses. Annual rolling average neonatal death rate is also shown (orange line)
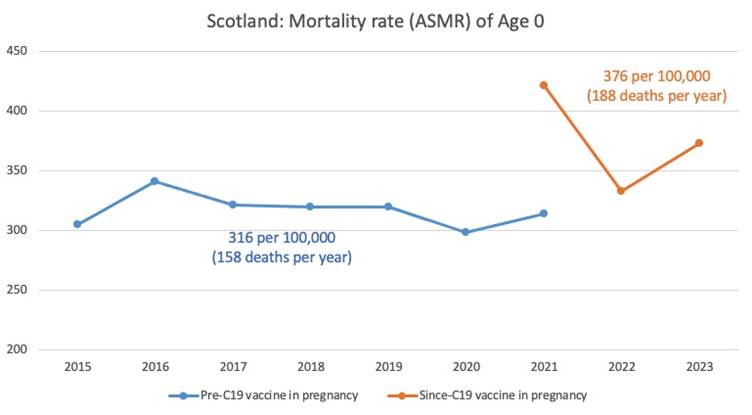
Figure 4: Scottish data on age standardised mortality rate at age 0 over time. 2021 has two data points for the period before and after rollout of vaccines to pregnant women.
In England and Wales, there were 1.09 deaths of babies under 1 year old in 2018-2020 whereas in 2021-2023 this rose to 1.38 babies.
Certain ionizable lipid nanoparticles can deliver their mRNA in a concentrated way in the placenta and have been proposed as a way of delivering placental treatments. An equivalent study has not been carried out in pregnant animals to demonstrate distribution of lipid nanoparticles and mRNA used in the covid vaccines.
A study on pregnant rats given a human sized dose of the Pfizer/BioNTech vaccine was published in January 2024. It is unknown how much spike protein would be produced in a rat compared to a human with that dosage of pro-drug. The offspring had “a substantial decrease in neuronal counts in critical brain regions, indicating potential neurodegeneration or altered neurodevelopment” and the male offspring had “a marked reduction in social interaction and repetitive patterns of behaviour.” This is the kind of study that should have been carried out before any pregnant woman was injected.
Ten out of thirteen women produced fatty vesicles called exosomes containing intact spike protein mRNA in their breast milk up to 45 hours after vaccination with Pfizer/BioNTech or Moderna.
It was known from November 2021 that exosomes expressing spike protein circulated in the blood up to 4 months after injection. It was previously established that exosomes can be shed in breastmilk. The long-term effects on the infant still cannot be known.
The WHO is still maintaining to this day that pregnant women should get a single covid shot with each pregnancy ‘regardless of prior vaccination’. On the basis of any rational risk-benefit analysis, these products should never have been given to pregnant women in the first place, let alone in each pregnancy.
2.9 Coercion
Behavioural Science was employed to manipulate the entire population using ‘nudge’ without consent, funded by taxpayer money. Hundreds of millions were spent on advertising to ramp up fear and sell the idea that the vaccine was the only solution. Despite early recognition that the SARS-CoV-2 virus posed no greater risk than influenza to the large majority of the population, fear levels among the general public were deliberately ramped up to disproportionate levels.
Inflated perception of risk of death
An early covid outbreak occurred on the Diamond Princess cruise ship in February 2020, where 8% of the mostly elderly passengers and crew had a symptomatic infection. After nearly a month of follow up there had been 7 deaths all of which occurred in those over 70 years of age. It is unclear what role the sudden introduction of novel high-risk and unorthodox treatment protocols, such as late-stage Remdesivir prescribing and mechanical ventilation had on these deaths. The mortality rate after a month for those with symptomatic infection was 0% for the under 70 year olds and 4.2% among the over 70 year olds. That would work out at an overall population mortality rate of 1% (half of that if asymptomatic infections are included as meaningful).
As late as 14th April 2020, when it was clear from a multitude of real world data and research papers that the mortality rate (for those with an actual infection) was going to be much lower than 1% (and orders of magnitude lower for the healthy under younger population), the WHO claimed the infection fatality rate was 3.5%, reboosting fear levels in the public.
A large proportion of deaths labelled as ‘covid deaths’ occurred in people already close to death. Any assessment of years of life lost and the overall impact needs to account for this. Neil Ferguson said, the proportion of people who died from covid that would have inevitably died soon anyway, “might be as much as half or two thirds of the deaths we see, because these are people at the end of their lives or [who] have underlying conditions.”
The NHS noted that 95% of Covid-related deaths occurred in individuals with pre-existing conditions and yet they were labelled ‘covid’ deaths in the public data, skewing data and ramping up fear.
Age was a major determinant in Covid mortality, with most deaths occurring among the elderly. Furthermore, a significant portion of covid deaths occurred due to infections in hospitals and care homes. Including these deaths in risk calculations for the healthy elderly community can be misleading. For instance, a sample of 30,000 patients who tested positive for Covid following a lengthy hospital stay before spring 2021 saw a mortality rate exceeding one in four.
Surveys from November 2020 revealed that the average person believed the mean age of death from Covid was 65. However, the actual mean age of a Covid death was 80, and the median age was 82, exceeding the average age of death in pre-Covid years.
Dr Colin Foad led a UK study surveying attitudes to covid and found, “people judged the threat of COVID-19 via the magnitude of the policy response.” It is worth noting that the perceived risk was massively inflated due to government messaging emphasising the covid threat. Mortality rates by age calculated by Cambridge University’s biostatistics department (see module 3 witness statement) indicate a stark contrast with public perception.
Fear
In a document drafted in March 2020 by the government’s Independent Scientific Pandemic Insights Group on Behaviours (SPI-B) unit, it was recommended that “the perceived level of personal threat needs to be increased among those who are complacent, using hard‐hitting emotional messaging based on accurate information about risk”. There was never any ‘accurate information about risk’. Quite the opposite.
Plans to increase levels of fear appear to have been carried out without any consideration as to how to limit or turn off their effects. Objectivity can be lost when people are fearful and there seemed to be a positive feedback loop whereby those responsible for the fear generation were also affected by it, justifying their belief in the need for more fear propaganda.
Because of the relentless propaganda campaign, by summer 2020 British citizens believed 6-7% of the population had died from Covid-19. In 2021, over 60% of people remained anxious about the lifting of restrictions.
People held the following false beliefs due to false claims made in PR campaigns:
- The virus was a mortal threat to them personally;
- Vaccinations could defeat the virus and take us back to normality;
- Vaccinations would protect those around them;
- They had a realistic chance of personal benefit from the injections in terms of a reduced risk from covid.
Pressure
The public were exposed to overly optimistic selling of the vaccines in the media and by those in positions of authority. Religious Leaders like The Archbishop of Canterbury who said “to love one another, as Jesus said, get vaccinated, get boosted” were used to increase vaccine uptake. Andrew Neil, a political journalist said, “It’s time to punish Britain’s five million vaccine refuseniks: They put us all at risk of more restrictions, so why shouldn’t we curb some of their freedoms?” Edwina Currie, former UK politician said, “I don’t want them sitting next to me in the theatre, I don’t want them standing next to me at the theatre bar. I don’t want them next to me or anywhere near me or even in the same carriage, on the train. So yes, they can exercise their freedom by staying at home.”
A Danish study showed vaccinated people were more discriminatory towards the unvaccinated than they were towards ex-criminals and drug addicts.
Discussion of denial of healthcare was also promoted. Esther Rantzen went further saying healthcare for any condition for unvaccinated people should be denied, “If you decide that you don’t want a vaccine or a booster, then you can decide not to go to hospital however ill you get and that is your right.” Piers Morgan, a daytime TV presenter said, “Those who refuse to be vaccinated, with no medical reason not to, should be refused NHS care if they then catch covid.”
A shocking NHS England document recommended that healthcare staff ‘leverage anticipated regret’ on the over-65s cohort by telling them they are ‘over three times more likely to die’ than younger people, and recommending a follow-up statement of, ‘Think about how you will feel if you do not get vaccinated and end up with Covid-19?’
Vaccine passports
The introduction of vaccine passports was highly coercive. Nicola Sturgeon admitted that when the vaccine passport scheme was launched, “one of its primary objectives was to help drive up vaccination rates.”
In the UK, in January 2021, the vaccine minister said, “No one has been given or will be required to have a vaccine passport.” The promise lasted only until December 2021. By November 2021, Sajid Javid, the then health secretary said he could not rule out barring those over 65 years of age who had not had a booster dose from trains or restaurants.
The WHO issues detailed guidance in August 2021 on digital vaccine passports. It proposes their use for accessing university education and work and suggests they might be used to exclude people from care homes, schools and airports and then unironically adds “They should never create inequity due to lack of access to specific software or technologies.” The WHO also recommended the linked data includes the date when the next dose is due and that there should be clear and transparent processes for revocation of a pass. They described the “digital health infrastructure” as a foundation to “support other digital health initiatives.”
Young people, some of whom had been incarcerated in their university halls, were easier to coerce and ended up with higher vaccination rates than people in their 30s.
2.10 Mandates
Mandates contravene everything set out pre-2020 in accepted medical ethics around bodily autonomy. There does not need to be any lengthy discussion here. There simply needs to be the admission that the mandates were wrong and should never be repeated here in the UK.
Given how evidently harmful and lacking in efficacy these products were, it makes the mandates for care workers even more unconscionable. Forcing one of the most valuable and yet financially undervalued groups of workers in the UK to forego their right to choose, was abhorrent, if not criminal.
The care sector is still reeling from the loss of around 40,000 workers most of whom never returned. The knock on effects on the NHS have been clear because difficulties with discharge leads to an inability to clear beds and backlogs in the emergency department.
Only when healthcare jobs were under threat did healthcare workers stand as one against mandates such that they had to be dropped at the last minute, after many who did not want to take the injections had already received them in order to remain employed by the NHS.
Because the word ‘vaccine’ had been used and because of the way the vaccines had been marketed there was a belief that infections would be prevented by those who took them. The WHO campaign “no-one is safe until everyone is safe” would have contributed to this idea along with the policy of trying to vaccinate the whole community, even children.
By June 2021, 85% of care home staff had had a first dose and 72% had had a second dose. There appears to have been no attempt to investigate why 13% of care home staff members had made the decision to have one dose and then chose not to complete the course. Only three upper tier local authority areas had vaccination rates less than 80%.
A study in Cambridge, published in August 2021, traced transmission using viral genetics and showed that the vast majority of infections acquired in hospitals were from other infected patients, not asymptomatic members of staff.
By September 2021, Robert Peston reported that the UKHSA data was showing a clear trend of increasing cases per 100,000 in the vaccinated population which were higher than the rates in the unvaccinated population. UKHSA responded to this by simply stopping reporting this data from March 2022.
In September 2021, there were warnings of the potential loss of care home workers, a sector in which staff shortages were already well known. Nadra Ahmed, executive chairman of the National Care Association, told The BMJ, “We’ve heard of providers shutting the doors, they just can’t go on any more.” The Government estimated between 17,000-70,000 care home workers would leave because of the vaccine mandate.
From October 2021, care home mandates became law. All registered providers of residential care became legally obliged to verify the medical status of each worker, including agency staff and volunteers. Medical information was no longer confidential.
Vaccine mandates were also planned for healthcare workers but Health Secretary, Sajid Javid, had previously described mandates as unethical. However, in January 2022 he chose to visit one of the hospitals with the lowest staff vaccination rates in the country and was challenged by consultant anaesthetist, Dr Steve James on the logic of his proposal. In particular he highlighted the short duration for which efficacy was claimed and the high proportion of staff who had already been infected.
Finally in March 2022, just as the deadline for the vaccine mandate to be applied to NHS staff, the government did a U-turn.
It is noteworthy that the change of policy followed a consultation showing 90% thought the mandates should be dropped. Presumably a consultation six months earlier might have shown 90% of the public favouring mandates but major public health policy should not be driven by focus groups and surveys. It should be based on scientific evidence and ethical and legal considerations.
Coercing people to have a medical intervention is an ethical red line which should never have been crossed leaving the sacrosanct principle of bodily autonomy in need of urgent reinforcement. There were three major reasons why mandatory vaccination was illogical from a scientific basis too:
- Firstly the vaccines did not prevent infection and transmission, Indeed vaccination actually increases the risk of infection in the first 7-10 days and since the arrival of Omicron.
- Secondly, many health care workers had already had SARS-CoV-2 infection leading to good naturally acquired immunity.
- Thirdly, the vaccine was a new technology with a poor record on short term safety and with as yet no long-term safety data. It is important to state that even if these points were not the case, it would still have been unethical and unjustifiable to [unfinished sentence…]
Despite having a heavily vaccinated workforce there were more staff absent due to sickness from September 2021 to August 2022 than the year before:
Figure 5: Daily NHS staff absences comparing year after threatened mandates to year before
2.11 Misrepresentation of the nature of covid gene therapies
Covid gene therapies were (and still are) misrepresented as vaccines. The evidence strongly suggests that this was done to circumvent legalities around emergency authorisation of medicinal products as certain exemptions could be applied to products termed “vaccines.”
The term unvaccinated was also misapplied, arbitrarily deciding that individuals receiving the shot were deemed ‘unvaccinated’ until 2 weeks after the first injection. Similarly, those within two weeks of the later doses were categorised as not yet having had that injection. This has the doubling effect of (a) distorting the genuine control group’s data and (b) hiding any signals/issues in the vaccine group during those weeks.
There was a blanket denial that these products were experimental. That was an outright lie as there was no long-term safety data. A normal time-scale for the development of a vaccine is 10-15 years. These products were brought to market in just under a year and were even injected into children and pregnant women. This was reckless in the extreme and is still hard to believe, given the known minimal risk of the disease by the time these products were rolled out to younger cohorts.
ABPI Code of Practice was broken. It states that you can’t talk about Relative Risk without Absolute Risk (Clause 6, supplementary information). It also states that the word ‘safe’ must not be used without qualification (section 6.4). These rules were put in place after the Thalidomide disaster.
The Blue Guide is the MHRA ‘law’ on what you can say when marketing a drug. All this was overridden (see Failure to police the marketing section 5.21).
2.12 Censorship and Smear Campaigns
Democratic societies uphold free speech not only as a fundamental right, but as one of its defining features; silencing individuals breaches not only their rights but the rights of the listener.
Free speech also acts as an important means of error correction. Dissenting voices have been silenced by a variety of means on social media, in the traditional media, in the scientific literature and even by preprint servers. As a result, important, but inconvenient truths, have not been heard, preventing catastrophic errors in covid policy from being exposed.
It is essential that the censorship infrastructure that was put in place by the UK Government and underlying departments is fully dismantled and appropriate remedies put in place such that the like of it can never again be recreated.
a. Two Categories of Censorship
This censorship process manifested itself in two broad categories:
(1) matters of fact and legitimate (if critical) viewpoints of government policy were often suppressed (“Truth Suppression”) and
(2) otherwise facile misconceptions, wishful thinking and (in some cases) outright untruths were promoted and amplified by state or quasi-authoritative media outlets (“False Information Amplification”).
These two categories of censorship combined with devastating effect to restrict the ‘Overton window’ of accepted public discourse. The dual impact of these two strategies was a catastrophic double whammy to the already precarious checks & balances provided (in normal circumstances) by constructive critique and investigative journalism. For all of us, this resulted in great harm and damage (and a weakened society and economy); others paid a dearer price, losing their livelihoods, their health and, in some cases, their lives.
b. Examples of Truth Suppression
Disclosures in a Louisiana court case revealed a “Censorship Enterprise” which “is extremely broad, including officials in the White House” and numerous other federal departments. The result was “intensive oversight and pressure to censor that senior federal officials placed on social-media platforms”. Closer to home, Big Brother Watch have outlined in their report (entitled the Ministry of Truth) how similar tactics were deployed in the UK resulting in, inter alia, the use of special relationships with social media companies to remove content deemed to be ‘disinformation’, but often applied to information that was correct, or — even more worryingly — to information that was merely of inconvenience to government policy (or unnamed officials within the Cabinet Office). The vaccine injured were repeatedly branded as anti-vax and their experiences as misinformation.
c. Examples of False Information Amplification
‘Celebrity’ doctor, Dr Sarah Kayat appeared on This Morning saying ‘after 12 days from the first vaccination of the AstraZeneca vaccine, you are 100% effective against hospitalisation and death’. Another celebrity medic, Dr Ranj Singh said publicly “what people don’t realise is one dose of any COVID vaccine gives you 100% protection against being hospitalised or dying.” Dr Hilary Jones said, “Those people who haven’t been vaccinated, we’d really love you to think again and be vaccinated because 90% of people in hospital are unvaccinated right now with Covid.” These false claims were never called out as misinformation in spite of overwhelming evidence showing these were false statements.
d. Attacking Individuals
Meanwhile, many clinician and scientists raising concerns were either reputationally smeared or disappeared from view. A particularly harrowing example was the treatment of Oxford epidemiologist, Professor Sunetra Gupta who was one of the main architects of the Great Barrington Declaration. In his book Spike, Jeremy Farrar, Wellcome Trust Director reveals that Dominic Cummings, a powerful government advisor, “wanted to run an aggressive press campaign against those behind the Great Barrington Declaration and others opposed to blanket Covid-19 restrictions.” The three were subsequently falsely accused of being right-wing libertarians with links to the Koch brothers and of causing unnecessary deaths.
Before discussing specific policies it is important to note that there were deliberate attempts to squash any debate of these policies. Censoring of alternative voices created a false illusion of consensus among scientists and within the population. Error recognition and correction was consequently hampered as criticism was simply not heard. This is extremely dangerous in the field of medicine.
Since early on in the emergency, broadcast media was driven by specific Ofcom guidelines into preventing any criticism or even questioning of government policy from being aired, at times when constant evaluation and discussion were badly needed. Not allowing debate from opposing viewpoints may be commonplace in totalitarian regimes, but should never happen in a liberal democracy.
This Ofcom “note to broadcasters” in particular — issued on 26 May 2020 — contains wording which would have had a severe chilling effect on free speech, advising that particular care needed to be taken when broadcasting: “statements that …. undermine people’s trust in the advice of mainstream sources of information about the disease”.
What was of particular concern was the speed and severity of Ofcom’s directives. Eamonn Holmes was singled out after agreeing with an interviewee on her position rejecting a conspiracy theory. However, he allowed room for thoughtful discussion saying,
“what I don’t accept is the mainstream media immediately slapping that down as not true when they do not know it’s not true… It is very easy to say it is not true because it suits the state narrative. That’s all I would say as someone with an enquiring mind”.
John Stuart Mill is clear on the importance of having debate, even with people you believe to be wrong, so that those who are right can win people over rather than come across as dogmatic, thereby undermining their own arguments. OfCom admonished him for saying words that ‘could have been interpreted as a rebuke of the ‘mainstream media’”. The mainstream media are not high priests and OfCom is not there to protect them but the public.
A Conservative MP, Neil O’Brien, who was then working as a parliamentary private secretary in the justice department, set up a website with the specific objective of attacking individuals (including doctors, scientists and journalists) who expressed any viewpoint contrary to SAGE messaging. The website is still live and contains a substantial number of claims, presented as facts, which are now discredited, thereby illustrating the uncertainties inherent in the subject matter, which, instead, Mr O’Brien tried to paint as “settled”. Neil O’Brien worked in the justice department from August 2019 until September 2021 when the website was published. He was later promoted first to Michael Gove’s department and became Parliamentary Under Secretary of State at the Department of Health and Social Care between 7 September 2022 and 13 November 2023.
Big Brother Watch has exposed how the government funded attempts to silence and discredit “dissident” scientists using tactics reminiscent of the soviet era rather than an enlightened Western democracy. The Government set up several opaque surveillance strategies to monitor people who are “critical of the government” and “tackle a range of harmful narratives online”.
Some of this dirty work was outsourced – at taxpayer expense – to army units and private companies such as Logically.ai (TheLogically Ltd), which claims to “‘intercept [misinformation and disinformation] threats before they become widespread.” Logically.ai appointed Brian Murphy, a senior Department of Homeland Security and former FBI executive as ‘Vice President of Strategic Operations’.
Members of HART and others who signed an open letter to the MHRA setting out the safety and ethical concerns of vaccinating children were each reported to the Counter Disinformation Unit. At no point has anyone stated which of the facts within that letter were considered disinformation. A record was kept of me by both the Cabinet Office and the Counter Defence Unit within the Department for Digital, Culture, Media and Sport. The information held on me included me asking questions, comments made in discussion within my area of expertise on covid testing and sharing of articles in the mainstream press.
There are numerous instances where information that was declared to be ‘misinformation’ by ‘fact checkers’ turned out with time to be true. A fact check on the lab leak theory had to be retracted. The WHO called aerosol spread misinformation in March 2020 and then conceded that long distance aerosol spread was real by December 2021. The idea that vaccines caused menstrual irregularities was described as misinformation and has since been acknowledged as genuine adverse effects by the European medical regulator. The fact that natural immunity would provide protection was called misinformation but that too has been shown to be true. It remains against YouTube’s rules to post content that says the vaccines do not reduce transmission or contraction of disease, while the evidence shows that the rate of infections are highest in the most vaccinated. In December 2020 Nadim Zahawi declared that there would be no vaccine passports, only for the government to perform a volte-face a few months later.
Despite there never being any proper evidence that the vaccines stopped spread (something that a Pfizer executive admitted to the European Parliament recently), the government insisted on using coercive tactics on the population (e.g. “the vaccine protects your loved ones”) for months after it became obvious that the vaccinated were catching covid as frequently (if not more so – see section 8.8) than the unvaccinated.
Following an illegal hacking incident, six months’ worth of HART’s private internal group messaging was leaked and made public. Logically.ai (in receipt of government funding) then gleefully dissected and publicised this ‘leak’, attempting to frame our activities as being somehow subversive by publishing out-of-context quotes from these informal chat logs. Yet the thrust of the criticism seems to be that HART members were openly discussing the possibility that the government was over-frightening the public and unethically using covert nudge strategies to increase compliance, notions which hardly seem controversial today.
We reported the hack to the police, who agreed that this constituted an illegal hack. The police issued a URN number and one of the perpetrators was identified, but no prosecution ensued.
Several of HART’s members have been hauled in front of regulators, seemingly merely for expressing alternative points of view. Although no suspensions or worse have resulted, these incidents clearly have a “chilling effect” on the willingness of professionals to speak out against perceived wrong-headed policy, severely interfering with the usual correction mechanisms the public assumes are in place. For the individuals concerned, they amounted to extraordinary levels of stress, time and money to effectively defend themselves.
A vocal critic of covid policies, Dr David Cartland has shared his annual appraisal report which said,
“In addressing issues within this domain we have some conflicting views to consider. From your own perspective you are convinced that you have followed GMC guidance by ‘whistleblowing’ your concerns around COVID and COVID vaccines. If we view this activity on its own and without any other context, we would acknowledge and applaud your concern for patient safety and your bravery in ‘whistleblowing.’ By a bizarre twist of fate these are the issues that many of the people who disagree with you feel makes you unsafe as a doctor. We need to be able to say when we feel processes are unsafe and I applaud you for voicing your concerns. However, we also have to work within a group consensus and sometimes this is difficult. For most of us this means putting our collective heads down and shrugging our shoulders. You have not been prepared to do this but it is to people other than this appraiser to decide if that is of itself unsafe.”
Without the ability for professionals to question group consensus we lose vital error correction mechanisms which will lead to harm.
tThere was also a promulgation of articles in reputable publications suggesting that “those who spread misinformation about vaccines” should be criminalised. When this appears in a medical journal, the result is more self-censorship within academia and it contributes to an environment where questions cannot be asked, criticism is not heard and errors are not corrected.
e. Data Withheld
Data that was critical to answering important questions was either never published or was withdrawn from publication when it started to show problems. For example, UKHSA produced a weekly report of covid case rate, hospitalisation rates and death rates by vaccination status. Every month the rates in the vaccinated worsened until at the point where the rates in the vaccinated overtook the unvaccinated the data stopped being published. Other data sources that also showed a similar or higher infection rate in the vaccinated compared to the unvaccinated stopped publishing in early 2022 including data from Public Health Scotland, Iceland and Ontario.
The ONS produced a deaths by vaccination status database but failed to produce data by vaccine type. Although the initial release had weekly data and small age groups, later releases had only monthly data and grouped everyone under the age of 39 together. The reports became more infrequent over time and the last report was released in August of 2023 with data that only went up to May 2023. Whereas previous releases accounted for the majority of total deaths in the country this release only included a fraction and there has been no release since.
On 2nd February 2023 I asked through an FOI for the UK Health Security Agency to release anonymised record level data on vaccination dates and deaths for over a year. They admit they have it. The MHRA admits that all this data has been released to Pfizer, AstraZeneca and Moderna. Despite the Information Commissioner’s Office telling them that there is case law showing that anonymisation of data in the way I suggested does not count as creation of new data they are claiming it does and using that as an excuse not to release the data. The latest response from the Information Commissioner’s Office is that I have to wait 6 more months before a case officer will be assigned to this issue. This is not acceptable.
3. SWINE FLU: A DRY RUN FOR COVID
| To fully understand the covid vaccine roll-out, the history of the Pandemrix roll-out for the 2009 H1N1 ‘swine flu’ is extremely important to appreciate. The parallels are impossible to ignore and the event even features many of the same individuals as the 2020 covid event (Drosten, Fauci, Ferguson, etc.). The detailed recommendations and pitfalls outlined in the government reports of those who investigated this event were completely ignored in 2020. |
3.1 Use of inappropriate testing
Christian Drosten ‘won the race’ to produce swine flu PCR’ in 2009 (he also won this race in 2020, in a jaw-dropping peer-review process that lasted approx 2 days). The PCR test was then abused to create clinically irrelevant cases via the detection of clinically irrelevant ‘asymptomatic cases’, skewing prevalence perception. This paved the way for emergency use authorizations.
3.2 Exaggeration of the threat
The WHO controversially altered the wording of ‘pandemics’ on their website, removing references to a pandemic’s impact and severity as a necessary condition. The World Health Organization (WHO) declared a public health emergency of international concern on 25th April 2009. Fraser, Ferguson et al published a paper on 11 May, 2009 stating that one-third of the population would become infected within six to nine months. They commented that Mexico experienced a mortality rate of 0.4 to 1.4 percent among those infected. If applied to the UK, this projected a potential death toll between 82,000 and 290,000. MSM was then used to spread this message. All broadsheets ran with some version of this story. WHO’s director-general then warned on July 21st, 2009, that it would become the ‘most substantial flu pandemic ever recorded’.
3.3 Governments decided a vaccine was the solution without waiting for evidence
Contracts for the vaccine were signed in many countries before any trial evidence was available. Authorisation under “exceptional circumstances” in both Europe and the USA in September 2009 was given despite not all vaccines being tested on target groups, such as children and pregnant women.
The claim that traditional egg based influenza vaccines could not be made fast enough was used to justify the use of vaccines with adjuvants that were patentable and therefore could make more of a profit. This was recorded in an EU report which said, “The fact that only patented products received authorisation was the reason why the vaccines could be monopolised by a few companies and sold at much higher prices than seasonal vaccines, which are traditionally produced in chicken eggs and could have been provided much faster by many laboratories all over the world using non-patented procedures… Given that new flu virus variations are detected almost every year, the virus could possibly have been treated by flu vaccines in stock, instead of having to produce a special product in a very short time,”
3.4 Vaccine rollout pushed ahead
Vaccine roll-out happened in the absence of
- a genuine threat;
- evidence of efficacy and safety of the products;
Children and pregnant women were prioritised despite there being no data on these groups. Without any evidence, a media campaign was launched with headlines such as Fast-tracked swine flu vaccine will be safe, officials insist(The Guardian, July 2009). A GlaxoSmithKline press release from October 2009 revealed that, despite only having trial results from 130 participants, 7 million doses had already been distributed. Larger-scale trials involving thousands of patients were still ongoing. Fast-forward to February 2010, and 31 million doses had been administered globally. 132 million doses were purchased by the UK government and in total, 5.5 million Britons took the vaccine.
3.5 Reality: there was never a swine ‘flu pandemic
The WHO declared pandemic over in Aug 2010 despite an increasing percentage of influenza patients being diagnosed with swine flu in August 2010. It was only ever a regular flu virus with higher rates of PCR testing used to give impression of more ‘cases’ in 2009/2010:
Figure 6: WHO data on global positive samples
3.6 Outcomes of government responses
The UK had a total of 457 deaths including deaths “with” and “of” swine flu. The overall death toll in England during the swine flu ‘pandemic’ winter was lower than the preceding winter. It is likely given what we know about flu seasons, that more lethal strains of ‘flu were in fact displaced in 2009 with the less harmful swine flu virus.
In Poland, Health Minister Ewa Kopacz, identified a high risk group of 2 million Poles and set aside money to purchase vaccines for them but Pharmaceutical companies wanted indemnification from liability which she rejected, saying, “It is not acceptable that governments should become hostages to interest groups and should take decisions in an atmosphere of panic resulting from alarmist announcements in the media.” In Poland, the death rate was only 0.47 per 100,000. In Sweden, 60 percent of the population was vaccinated, but the vaccine programme is only officially estimated to have saved six lives.
3.7 Recorded Vaccine Harms
In the UK alone, 240 children developed Narcolepsy (damage to the sleep centres of the brain) as a consequence of the Pandemrix Vaccine. Narcolepsy is a life-long disabling condition characterised by sudden onset of sleep or paralyzed pre-sleep states. The impact on these children’s lives was profound. It took 5 years to diagnose them all with an average 8 month delay between injection and diagnosis. In 201, the WHO were still attributing the problem to an “as yet unidentified additional factor… operating in Sweden and Finland.” The virus was blamed for causing the problem.
It took until 2013 for Public Health England to acknowledge an increased incidence of narcolepsy due to Pandemrix vaccination, estimating a risk of 1 case for every 52,000 doses. They downplayed the risk, suggesting that media coverage had exaggerated the issue and that those who had been diagnosed would have developed it later in life in the absence of vaccination. In 2020, Public Health England revised their estimate of narcolepsy caused by the vaccination to 1 in 34,500 doses. They stated, concluding that there was “strong confirmatory evidence of a causal association” that the observations were not explained merely by the vaccine having “accelerated the onset in those who were destined to develop narcolepsy later.”
3.8 Tamiflu antiviral drug
In addition to the vaccine drive, the antiviral drug Tamiflu was stockpiled by governments. Before a single case had been diagnosed in the UK the government purchased sufficient Tamiflu to treat 80% of the population. There were no independent trials and the authors of the pharmaceutical sponsored study were not even privy to all the relevant data. Tamiflu was completely ineffective in reducing pneumonia or hospital admissions and was linked to considerable side effects.
In March 2007 the Japanese authorities advised against prescribing oseltamivir (as Tamiflu was branded in Japan) to adolescents aged 10-19 years after the suicides of two 14 year olds who jumped to their deaths while taking the drug. 52 other deaths (14 in children or adolescents) have been associated with the same drug.
3.9 Reports and Inquiries to prevent a repeat of the mistakes
The Council of Europe produced a damning report on lack of transparency. Influence of the pharmaceutical industry during the ‘pandemic’ skewed objective decision-making. Pharmaceutical companies banked more than $7bn as governments stockpiled (completely ineffective and harmful) drugs and vaccines. Labour MP Paul Flynn spoke about swine flu in parliament in November 2010, saying:
“It distorted all the priorities of the health service for a year. The health service gave attention to that rather than to the other things that it should have given attention to. It also involved the use of a vaccine that had not been trialled. The people who say it was not fully trialled are those who made it—GlaxoSmithKline and the other producers. That was a major event, and we might consider, knowing what we know now, how we got into that situation.”
Paul Flynn’s report to the European Council which also pointed out the highly suspect timing of the change in the definition of a pandemic and accused the WHO of taking a “highly defensive stance… whether in terms of being unwilling to accept that a change in definition of a pandemic was made, or an unwillingness to revise its prognosis on the pandemic”. He referenced the “waste of large sums of public money, and also unjustified scares and fears.” “The general feeling of anxiety and unease in the population…can fuel the media in what becomes a cycle of fear mongering…public opinion can be manipulated in favour of particular commercial interests.”
Health journalist, Jeremy Laurance in the Lancet asked, “If it turns out that we have used a sledgehammer to crack a nut, my question is this: how did the virologists get the scale of the threat so wrong?” Dame Deidre Hine was commissioned by the government to write a report on swine flu which was highly critical of the government response to the virus.
“Use of the phrase ‘reasonable worst case’ should be reconsidered in future. It suggests that the outcome is relatively likely, whereas this is usually quite the opposite… Ministers should determine early in a pandemic how they will ensure that the response is proportionate to the perceived level of risk…Ministers and senior officials should receive training on the strengths and limitations of scientific advice as part of their induction… SAGE [should release] papers to a wider group of scientists than those engaged in SAGE, who would be bound by confidentiality but who would have greater freedom to speak to the media. It was put to me that such a group would be able to comment authoritatively on the overall government strategy and give the media greater assurance about the approach being taken, as well as being able to challenge this if necessary and reduce the chance of group-think clouding views… modellers are not ‘court astrologers’ [and models were] dependent on a number of important assumptions, particularly about the number of fatalities prevented in a severe outbreak. Based on what we now know about the relatively mild nature of this outbreak, the actual benefits were lower. This raises two questions. Were the costs of the 2009 response value for money? And should the government resource the same approach again?”
We can now know that Hine’s report was completely ignored. Instead of heeding her advice, they did exactly the same thing again in 2020, and in fact doubled down.
4. BLOCKED MEANS OF ERROR CORRECTION
| Everyone depends on trusted sources to an extent. Politicians rely on their institutions. The public rely on both them and the media and all rely on credentialed experts. People can be reluctant to admit that relied upon sources might be trustworthy as it leaves them exposed. However, the evidence is clear that for medicine there are serious problems with the functioning of institutions, media, medical journals, the medical profession and the medical regulator are not functioning properly and are impotent in their role in error correction. |
4.1 Institutional Capture
The influence of corporations on science, universities, regulators and political decision making is multifaceted and strategic, according to Legg et al. The methods employed by these industries are diverse and often covert, aimed at reshaping and distorting scientific evidence for their benefit. This manipulation can significantly impact researchers, policymakers, and practitioners who rely on scientific literature for information, as they may encounter evidence heavily skewed in favour of industry interests.
Key strategies identified by Legg et al. include:
- “Influence the conduct and publication of science to skew evidence bases in industry’s favour”
- “Influence the interpretation of science to undermine unfavourable science and create a distorted picture of the evidence base” with a strategy to “Monitor and attack scientists and organisations” and “remove individual scientists from positions of power.”
- “Influence the reach of science to create an “echo chamber” for industry’s scientific messaging” with a strategy to
- “Silence plaintiffs using secret payments”
- “Recruit, fund, and train individuals to be trusted scientific voices for industry”
- “Fund, produce and disseminate materials which package science in industry-favourable ways.”
- “Fund media outlets in order to influence what is disseminated” and “co-opt journalists through media training and conference funding.”
- “Infiltrate decision-making contexts in order to ensure industry friendly scientific stances are heard”
- “Create industry-friendly policymaking environments which shape the use of science in policy decision-making in industry’s favour”
- “Manufacture trust in industry and its scientific messaging” with a strategy to “Ensure and normalise industry’s presence in academic settings in attempts to gain trust and scientific credibility within academia.”
There are several signs that progress in science has slowed. The age at first innovation is increasing while the number of patents per capita has been decreasing. Fewer Nobel prizes are for fundamental breakthroughs. There has also been a steady decline in publications that are disruptive, i.e. prove past hypotheses were wrong.
In recent years, there has been a notable increase in financial support from the corporate sector to universities. Corporate funding often comes with certain constraints, such as limitations on the publication of research findings and the imposition of intellectual property rights, including patents, that are controlled by the sponsors. Instances have been recorded where corporate sponsors, particularly in the pharmaceutical sector, have either postponed or completely prohibited the dissemination of research outcomes.
4.2 Media Capture
Since 2019 there has been coordination of the news stories that are reported through the ‘Trusted News Initiative’. This is a cartel of media establishments who control the official narrative under the guise of stopping fake news. Organisations signed up include the BBC, Facebook, Google, YouTube, Twitter, Microsoft, Reuters, Financial Times and The Wall Street Journal among others. Any agreement to speak in unison destroys the role of the media as an error correction mechanism.
In early 2020, Ofcom threatened broadcasters should they cover anything that went against the Government narrative, “We remind all broadcasters of the significant potential harm that can be caused by material relating to the Coronavirus… Ofcom will consider any breach arising from harmful Coronavirus-related programming to be potentially serious and will consider taking appropriate regulatory action, which could include the imposition of a statutory sanction.”
Who decides what is a “potential harm”? Given how unpredictable live broadcasting can be, why would broadcasters risk inviting guests that might say something which could be a “potential harm” and which could risk their broadcasting licence?
Sarah Knapton, Science Editor at The Telegraph reported “On the day we published the story [linking jab to clots] we received a threatening phone call from a senior official at the MHRA warning that The Telegraph would be banned from future briefings and press notices if we did not soften the news.”
Twitter instigated rules that resulted in any mention of ivermectin or hydroxychloroquine would be removed from their site. Facebook removed articles about the evidence for a lab leak and even directed people to a Chinese propaganda site instead. LinkedIn removed an article defending nurses with natural immunity whose jobs were at risk because they did not want to take the vaccines and an article arguing against the politicisation of disease.
Public Relations firm Weber Shandwick worked for Moderna and Pfizer while at the same time working in CDC’s Vaccine Office. An employee described his role in the CDC saying “work focuses on boosting vaccination rates for flu, HPV, whooping cough and COVID-19.”
Groups that lobbied for vaccine mandates were paid for secretly by Pfizer. Factcheck.org was funded by a foundation with investments in Johnson and Johnson. Reuters chairman, Jim smith, responsible for Reuters fact checker was simultaneously a non-executive director for Pfizer.
4.3 The Capture of Medical Journals by Pharmaceutical Interests
A review of the problems around the medical literature pointed out that the journal editors have known of the problems for many years saying,
“In 2004, Richard Horton, editor of the Lancet, said that medical journals had become information laundering operations for the pharmaceutical industry. In 2004, the editors of PLoS Medicine stated that they will not be “part of the cycle of dependency…between journals and the pharmaceutical industry.” In 2005, Marcia Angell, former editor of the New England Journal of Medicine (NEJM), criticised the industry for becoming primarily a marketing machine and co-opting any institution that might stand in its way. In 2005, according to Richard Smith, former editor of the British Medical Journal (BMJ), medical journals are an extension of the marketing arm of pharmaceutical companies. According to Richard Horton, much of the scientific literature, perhaps half, is simply wrong.”
Much of the medical literature has been written based on modelled studies or else studies where the raw data shows a finding which is reversed after statistical “adjustments” such that the opposite conclusion is reached. The authors of other papers write comments in their introduction and discussion sections which are contradictory to their findings but allow them to present themselves as being supporters of the official narrative e.g. A report of an outbreak among fully vaccinated attendees of a Christmas party in Oslo concluded that vaccination “will continue to be a key control measure.” After demonstrating only a short period of effectiveness against Omicron one group said, “these findings highlight the need for massive rollout of vaccinations and booster vaccinations.” Papers that demonstrated the vaccine was only effective for a limited time would ensure they declared, “The results strengthen the evidence-based rationale for administration of a third vaccine dose as a booster.”
Peer reviewers have failed to notice obvious failings in methodology, analysis and interpretation on repeated occasions. Papers based on real world evidence have been poorly represented in the peer reviewed literature. Consequently credentialled scientists have taken to publishing independently but their work is then dismissed as not being peer reviewed. One paper highlighted the myocarditis risks associated with COVID-19 vaccination. After being published online in October 2021, it was abruptly and permanently withdrawn by the publishers without any explanation given to the authors.
In an article authored by Hui Jiang and Ya-Fang Mei, evidence was presented suggesting that the SARS-CoV-2 spike protein impedes DNA repair mechanisms in lymphocytes, potentially increasing cancer risk. A controversy arose when Jiang acknowledged the similarity between the spike proteins of the virus and the vaccine, suggesting a potential risk of the vaccine inducing cancerous DNA alterations. This admission sparked calls for the paper’s retraction, amidst a contentious debate over the political dynamics influencing the retraction process. Additionally, a separate study by Mark Skidmore, proposing that the vaccines may have resulted in over 200,000 fatalities, has been withdrawn by the publishing journal. The reasons cited were either minor issues that could be readily addressed or were unfounded e.g. alleged deficiencies in ethical approval for the survey underpinning the study and a lack of disclosure regarding the viewpoints of the survey’s financier.
A paper showing Ivermectin works to save lives disappeared after being provisionally accepted following three rounds of peer review with four referees (two from FDA) who all accepted the findings which were written with cautious conclusions. Four editors resigned from one journal after two papers on covid treatments were accepted by four to five peer reviewed experts after progressing through initial validation, editorial assignment, independent review, interactive review and review finalised (acceptance/rejection) and then a decision was taken not to publish.
Even preprint servers, where papers are hosted prior to peer review have created a filtering system. On 2nd February 2020, Kristian Anderson, one of the authors of the Nature cover up paper said “I’m starting to think that for outbreak research, the bioRxiv really needs to start screening submissions – it’s a slippery slope, but it’s justified at this stage.” The co-founders of two major preprint servers, medRxiv and bioRxiv defended their position saying they had a do no harm policy that they used to justify only publishing papers that supported the official narrative.
4.4 Weaponization of the Medical Profession
Around fifty medical professionals have approached me online, or even in person to thank me for speaking out, to say they agree with everything I have been saying but then they add that they feel unable to speak publicly with their concerns because of fear of losing their careers. The fear of consequences for speaking were well founded. Certain trusts in the NHS issued gagging orders with emails from chief executives banning staff from speaking to the media under any circumstances. Five carers who raised concerns about staffing levels were sacked as a result.
Two previous editors of the New England Journal of Medicine, Arnold Relman and Marcia Angell, said 20 years ago, “The medical profession is being bought by the pharmaceutical industry, not only in terms of the practice of medicine, but also in terms of teaching and research. The academic institutions of this country are allowing themselves to be the paid agents of the pharmaceutical industry. I think it’s disgraceful.”
4.5 Regulatory Capture
In 2005, the House of Commons’ health committee expressed concerns regarding the UK drug regulator that pharmaceutical funding could lead the agency to “lose sight of the need to protect and promote public health above all else as it seeks to win fee income from the companies.”
There was a unilateral decision by Dame June Raine, head of the MHRA, to change its role. In a speech given in March 2022 she described how she had attended a Downing Street meeting regarding covid testing. In response to the question about why the regulator was there, the prime minister said, “The MHRA will stop us killing people.” Raine describes how without hesitating she responded, “No, the MHRA will help keep people alive.” If Raine believed the MHRA was on a mission to save the world, was there anyone left trying to prevent harm?
Dame June Raine also saidthey “tore up the rule book” and “the covid pandemic has catalysed the transformation of the regulator from a watchdog to an enabler.” What is the point of a regulator who sees their role as enabling the pharmaceutical industry? An absence of regulation is how you ‘enable’. The point of a regulator is to act as a watchdog.
The regulator announced in February 2021 that it would aim to make a decision on every application within 150 days. This one size fits all approach shows total disregard for the importance of their role, as it leaves little room for demands from the regulator for further evidence to support efficacy or safety claims.
The CEO of Pfizer in Latin America, Carlos Murillo testified that the Pfizer contract was identical in 110 countries. The Brazilian contract With Pfizer included the following clauses,
- “Pfizer will not agree to request for local testing or request for lot release protocol or requests for registration samples” thereby tying the hands of the regulator.
- “In the event: (a) the Product does not obtain Authorization by September 30, 2021…then either Party may terminate this Agreement upon written notice to the other Party.” Putting immense pressure on the regulator.
- “Pfizer expressly disclaims any representations or warranties with respect to the Product, including, but not limited to, any representation, warranties or undertaking as to … fitness for a particular purpose.”
- Full indemnity.
- An agreement to ten years of confidentiality.
The Albanian and South African contracts are similar.
Matt Hancock announced the contractual agreement in parliament saying, “I would like to stress that the data so far on this vaccine suggests that there will be no adverse reactions, and so no liability.” The UK government signed up saying, “Willingness to accept appropriate indemnities has helped to secure access to vaccines…sooner than may have been the case otherwise.”
Given all of the above problems the medical regulator provides the last defence between the pharmaceutical industry’s commercially driven agenda and the safety of the public. The regulator has a responsibility to demand evidence from the manufacturers, both before and after any temporary authorisation and rein in any misplaced enthusiasm for a product. 55 drugs were found to be unsafe between 1971 and 2013 and withdrawn from the market by either the company or the licensing authority. Drugs like the failed vaccine Pandemrix are not included in this list because GlaxoSmithKline did not apply for renewal of its authorisation.
4.6 Pharmaceutical companies put profits before patients
The average time for a drug to be withdrawn from the market for safety concerns is 20 years. The reason for this long period is a combination of needing to accumulate harm in order to demonstrate that it exists and also systems which are not sensitive to detecting such harm. Pharmaceutical companies have a duty to put their shareholders first that is why we have regulators to protect the public.
The opioid crisis in the United States was notably exacerbated by the introduction and marketing of OxyContin as a secure and minimally habit-forming pain reliever, despite its known risks of dependency. Purdue Pharma, the drug’s manufacturer, pioneered the tactic of labelling drug-resistant pain as a “breakthrough” issue, a strategy that subtly encouraged increased consumption of the medication. In 2007, Purdue Pharma acknowledged wrongdoing and accepted guilt in a criminal case related to these practices. In April 2021, the government still referenced patients in hospital with covid as “vaccine failure”. That term stopped being used and the US term of “breakthrough infections” was adopted from the USA.
The Vioxx scandal centres on the anti-inflammatory drug Vioxx, produced by Merck and approved in 1999 for treating osteoarthritis, acute pain, and menstrual pain. Touted as a safer alternative to traditional NSAIDs due to fewer gastrointestinal side effects, Vioxx was later implicated in significantly increasing the risk of heart attacks and strokes, resulting in its market withdrawal in 2004.The manufacturers used a shorter cut-off for collecting cardiac adverse event data in the trials than for other adverse events because the heart attacks happened later.
Whistleblower Dr. David Graham estimated that Vioxx might have been responsible for 60,000 American deaths alone. This conclusion was drawn from various studies, including a study showing Vioxx users had a fourfold increase in cardiovascular risk compared to those taking naproxen. Merck, however, minimised these findings, suggesting naproxen’s protective qualities rather than Vioxx’s harmful effects. Subsequently, it was revealed that Merck might have been aware of Vioxx’s cardiovascular risks as early as 1997 and sought to downplay or suppress this information. Internal emails exposed a strategy to “neutralise” or “discredit” dissenting doctors. Despite Merck facing a nearly billion-dollar criminal fine and damages in 2011, this amount was a fraction of the $11 billion revenue from Vioxx. The incident highlighted profound flaws in drug regulation and the potential for profit even when a drug causes widespread harm.
Ex-Pfizer sales representative, John Kopchinskis said “At Pfizer I was expected to increase profits at all costs, even when sales meant endangering lives.” He was sacked two years before the drug he was raising concerns about was pulled from the market for causing heart disease and strokes. In 2009, Pfizer paid the largest criminal fine in history for “for misbranding… with the intent to defraud or mislead.”
Pfizer drew up contracts that included clauses giving them full indemnity or immunity from prosecution. India refused to sign such a clause and Pfizer walked away from a 1.4 billion person market, a sixth of the world’s population, rather than compromise. David Malpass of the World Bank explained how “Pfizer has been hesitant to go into some of the countries because they don’t have a liability shield.” Within the pharmaceutical industry alone there were 40 new billionaires thanks to covid.
The percentage return on investment within the pharmaceutical industry had been steadily declining since 1990 and was set to hit zero in 2020. In 2019 Anthony Fauci said a disaster would be needed to get the mRNA platform approved. “In order to make the transition from getting out of the tried and true egg growing [to make vaccines] –which we know gives us results which can be beneficial – we’ve done well with that – to something that has to be much better. You have to prove that this works then go through the clinical trials, phase 1, phase 2, phase 3 and then show that this particular product is going to be good over a period of years. That alone, if it works perfectly, is going to take over a decade…. We’re going to address the problem in a disruptive way and an iterative way – because you do need both.” In December 2022, the government signed a ten year contract with Moderna to produce 250 million mRNA vaccines every year in the UK.
On March 29, 2020, Dr. Tal Zaks, Moderna’s Chief Medical Officer (CMO) entered into an executive retention agreement with Moderna, under which he would receive a $1 million bonus if he stayed with the company until September 30, 2021.
Beginning in February 2020, Dr. Zaks consistently sold his shares in Moderna at approximately $1 million per week. This rate of selling was considered alarming by corporate governance experts, particularly due to Zaks’ critical role in overseeing clinical trials.
By September 2020, Forbes magazine raised questions about why Moderna insiders, especially Dr. Zaks, were selling large amounts of stock. In summer 2020, 50k shares were bought by insiders while 12m were sold. They speculated whether these insiders had concerns about the vaccine’s efficacy or safety that were not being disclosed to investors.
As of October 2020, Dr. Zaks had sold Moderna stock valued at approximately $50 million.
5. REGULATORY FAILURE
| The regulator was in a position to ensure novel products were only used in a cautious way, on as few as possible, and with extensive careful safety follow up in order to build a full picture of the effects in the real world. The MHRA not only failed to do this, but they disregarded their role in protecting public safety entirely. |
5.1 Introduction
It is somewhat difficult to separate regulatory failure from regulatory capture, as the latter will inevitably result in a degree of the former due to conflicts of interest. However, this topic is so central to the module that it requires a very distinct and clear section. One can argue about the degree of capture, but the evident regulatory failures are plain for all to see.
The prevailing embedded idea that vaccines are ‘safe and effective’ has led to a circular belief that vaccines somehow require fewer safety checks than other novel drug therapies. Even so, novel vaccines would ordinarily take a decade or more to go through safety checks. Influenza vaccines are (rightly or wrongly) exempted from this on the basis that their production involves an established technique using eggs to grow the target influenza virus. These novel covid injections were treated like influenza vaccines for regulatory purposes, despite them being based on a totally novel delivery platform that was completely unlike any previous medical product brought to market.
The Perseus Group wrote a comprehensive report which specifically addresses shortcomings in the MHRA’s assessment and monitoring of these products. It stated that for “A comprehensive independent inquiry must be launched into the MHRA’s regulatory processes and performance. The agency must undergo an overhaul of its governance and accountability processes to restore public trust.”
In 2005, the House of Commons’ health committee expressed concerns regarding the UK drug regulator in that pharmaceutical funding could lead the agency to “lose sight of the need to protect and promote public health above all else as it seeks to win fee income from the companies.”
Baroness Cumberledge reported on the failings of the MHRA in June 2020 calling it, “disjointed, siloed, unresponsive and defensive. It has failed to listen to (patients’) concerns and when, belatedly, it has decided to act it has too often moved glacially.”
In March 2022, Dame June Raine, CEO of the MHRA, announced that the role of the regulator had changed “the covid pandemic has catalysed the transformation of the regulator from a watchdog to an enabler.”
The regulator aims to make a decision on every application within 150 days. The novel drugs were originally given a “temporary authorisation” which was enabled by The Human Medicines Regulations 2012. Phase 3 trials for the vaccines are not expected to complete for several years, with the main Pfizer/BioNTech trial completing in 2026. Leaked government contracts with Pfizer included a “liability waiver even for Pfizer’s negligence and for fraud or bad faith on the part of Pfizer itself.” Under these circumstances it was especially crucial that the MHRA forensically analysed the submission. E-mails from the EMA, which are available to WELT, show that the FDA, the British MHRA and the EMA itself had already agreed on the date of approval before they could even take a look at the Pfizer-BioNTech papers.
The Department of Health and Social Care wrote to the MHRA on 17th November 2020 requesting authorisation “on a temporary basis, of its proposed supply of a vaccine manufactured by Pfizer/BioNTech collaboration… under regulation 174 of Human Medicines Regulations 2012.”
A meeting in March 2020 between regulators “noted that the vaccine manufacturer should provide a rationale supported by data to justify why certain preclinical studies, such as toxicity studies, would not need to be conducted prior to proceeding to… clinical trials.” An FOI from the MHRA said, “All the Covid vaccines and therapeutics authorisation decisions were taken by the Licensing Minister and were not delegated.”
The cutoff date for inclusion in the trial data submission was 14th November 2020. The MHRA announced they had received the Pfizer trial submission on Monday 23rd November 2020. There were just eight working days for the MHRA’s workforce of 1,400 full time equivalent staff to evaluate the data. Pfizer/BioNTech continued to submit data up until the day of authorisation, 2nd December 2020. Lord Bethell signed off on the vaccine the day before – 1st December 2020. The manufacturers were left to decide what safety testing should be done instead of the regulators demanding it.
Speed and access were prioritised over safety. The WHO released a statement joint with regulators saying, “multilateral cooperation between regulatory authorities will be critical in ensuring there is a level playing field, that COVID-19 vaccines and medicines are safe, effective and quality-assured, and that all countries may benefit from such products equitably and at the same time.”
On December 11, 2020, the U.S. FDA issued an emergency use authorization for the product in question. Subsequently, within a span of ten days, European regulatory authorities also granted similar approval. Notably, the MHRA initially imposed a batch-specific approval process. However, due to the UK’s compliance with European Union regulations at that time, this requirement was effectively circumvented following the approval by the EMA. This sequence of events led to a cascading effect in regulatory standards, whereby the adherence to the lowest acceptable standards effectively undermined the efforts of any regulator attempting to enforce more stringent criteria.
5.2 Allowing the classification of gene therapies as “vaccines”
The covid vaccines fit the Health Research Authority’s definition of gene therapy, “a product… aimed at the transfer of a prophylactic, diagnostic or therapeutic gene (i.e. a piece of nucleic acid).” However, the public’s understanding of the term “gene therapy” was quite different and avoiding using the term may have been justifiable in respect of public messaging, though not inasmuch as it influenced the regulators’ approach to licensing.
BioNTech, the company that partnered with Pfizer to make the Pfizer product, published a paragraph about mRNA technology classification in their 2019 filing to the US Securities and exchange commission. In it they said, “mRNA therapies have been classified as gene therapy medicinal products.”
Moderna, in a similar filing, said, “mRNA has been characterised as a Gene Therapy Medicinal Product… the association of our investigational medicines with gene therapies could result in increased regulatory burdens, impair the reputation of our investigational medicines, or negatively impact our platform or our business.”
The WHO produced draft regulations for mRNA products in December 2020, only weeks before temporary use authorisations were granted for Covid-19 vaccines. However, these new regulations were quickly abandoned, and the vaccines were approved using the same regulations as traditional vaccines.
The medical regulators decided that these novel products should be classified as vaccines. This was a critical decision for three reasons. Firstly, the word “vaccine” is heavily loaded. The public perception of a vaccine is that it will stop infection and will be entirely safe. Secondly, anyone who might have a concern will be smeared as an anti-vaxxer” which is a heavily emotionally laden term that causes people to close their ears to the arguments. Thirdly, despite the reputation for complete safety, the regulatory pathway for a product described as a vaccine is not as demanding.
Pfizer said genotoxicity, carcinogenicity and biodistribution studies were “not considered necessary.” Even while their trial info sheet said “Due to the urgent need for a vaccine against Covid-19, with agreement from the MHRA, some of the tests usually required for a newly manufactured vaccine have been modified, in order to make the vaccine available more quickly for assessment.”
5.3 Failing to understand where the mRNA went and how long it lasted
Critically, mRNA is a pro-drug which turns cells into factories producing the end product drug – the spike protein. No one knows how much spike protein is produced in different age groups or how much it varies between people. Even basic information about the mRNA itself was not known. Although the mRNA products were marketed with the claim the active ingredients would stay in the arm (where they would be broken down entirely) this was not the case. The manufacturers and regulators knew or ought to have known that the claims being made in this regard were false. At the least, they ought to have identified it as a reason for further study.
The mRNA in the vaccine is modified with synthetic nucleic acid to prevent it from degrading quickly in the body. It is not known how the body handles this synthetic mRNA. No human studies were conducted to determine the distribution of the vaccine in the body, the organs that would produce spike protein, the quantity of spike protein produced, and for how long it would be produced.
Animal studies were required as part of regulatory approval, and as such available to regulators in 2020. They have only become available to the public as they were released pursuant to FOI litigation in the USA – Pfizer had wanted to keep data confidential for 75 years.
The studies on where the drug might be active included only the lipid nanoparticle delivery system and not the active mRNA product. Measurement stopped after 48 hours despite signs of an increasing rate of accumulation in the ovaries, liver, adrenal gland and spleen. All organs were reached. The low levels of total product in the organs implies significant amounts were present in the blood. For any of the product to have reached these organs it must have travelled via the heart, lungs and vascular system which will therefore have had significant exposure.
Pfizer claimed the mRNA would be “nearly completely degraded in 9 days” and claimed the spike protein would be broken down as if it was a regular human protein. However, human studies published more than a year after the vaccine rollout began showed mRNA or spike protein was detectable for considerably longer periods:
- mRNA 15 days in the blood
- mRNA up to 28 days in bloodstream
- both mRNA and spike proteins were detectable in lymph nodes for up to 8 weeks
- 150 billion spike proteins circulating in the blood of 3 out of 13 participants at two weeks.
- spike protein circulating in the blood for 4 months.
- spike protein from vaccination demonstrated in a shingles skin biopsy at 3 months
In 2023 it was demonstrated that half of the vaccinated population were still producing vaccine induced spike protein from 69 days to up to 6 months after injection when the study ended. It is highly unlikely for even modified RNA to remain active for such a length of time and the authors proposed either that it was integrated into the cell’s DNA or that of bacteria in the gut which became a continuing source of spike protein production.
5.4 Allowing the use of toxic lipid nanoparticles in an mRNA platform
The mechanism by which the mRNA technology works is to cause cells to express foreign protein as if they were infected by a virus. The immune system then destroys these cells and acquires an immune memory. With viral infection the cells which are destroyed are predominantly in the respiratory tract (and quite limited in number), whereas with these injections they can be all over the body including organs, like the heart and brain, where cells are never replaced.
The MHRA’s unprecedented rapid approvals meant that they did not appear to have identified (or discounted without investigation) that some of the ingredients were novel and known to be toxic. For instance, Pfizer’s lipid ingredients ALC-0159 and ALC-0315 had not been included in any licensed drug before and had undisclosed quality control standards. ALC-0315 is a type of man-made molecule called a cationic lipid, which can be toxic because it can trigger a process that leads to inflammation and cell death. This has become a major challenge for using cationic lipids in different applications. ALC-0159 contains PEG (Polyethylene glycol) which is known to cause anaphylaxis, a life-threatening adverse effect. The lipid nanoparticle technology used in the mRNA vaccines was previously found to be toxic when multiple doses were given, in attempts to make it work for conventional gene therapy. It was believed that they would be safer when used in vaccinations as only one dose would be needed.
The mRNA vaccine platform had been developed for other vaccines but had only been tested in phase 1 preliminary safety trials. The CEO of Pfizer commented that “mRNA was a technology that had never delivered a single product until that day.”
Before the covid vaccine trial 285 people had been administered mRNA vaccines, all in the last few years and all in a clinical trial setting. A recent trial of Moderna’s platform for vaccination against Epstein Barr Virus had to be terminated after myocarditis occurred in the participants.
Severe adverse events (defined as reactions that cause hospitalisation, disability or are life threatening) occurred in between one and twelve percent in these small trials. The primary safety concerns relate to liver toxicity and inflammatory and immune reactions, but the types of lipid nanoparticles used can also cause direct cell death in a laboratory setting.
- Allowing the use of dangerous viral vectors
- The viral vector used for delivering the AstraZeneca DNA message was reported in 2007 to cause platelet activation, which can lead to blood clots.
- It was also established in 2007 that similar adenoviral vectors could result in protein production for up to two years.
5.5 Allowing the use of whole spike protein
A critical part of vaccine design is that the material the body is exposed to is pathologically inert.
The spike protein is the part of the virus with pathogenic potential. It causes vessel damage and clots as well as direct damage to the lung. Part of the sequence is identical to a region of a bacterial sequence that can bind directly to a particular type of white blood cells resulting in lethal cytokine storms. This part of the sequence was heavily mutated in the Omicron variant making it less lethal. However, even with the less lethal virus circulating, the spike protein code that was being injected still contained this dangerous sequence. Even the more recent vaccines have included the original Wuhan or wild-type spike sequence.
The manufacturers decided to use the Chinese whole spike sequence as published on 11th January 2020 rather than parts of it, i.e. peptides, which have been shown to be safer for vaccine design.
Vaccinologist Peter Hotez explained how they knew from experiments on vaccines for SARS1 that using a whole spike protein (1255 amino acids) resulted in a damaging immune response (antigen dependent enhancement) compared to using only the fraction of the spike that binds directly to cells – the receptor binding domain (~200 amino acids). Nevertheless the whole spike was chosen.
In an attempt to reduce harm, two amino acids were added to prevent the spike from fusing with proteins on the cell membrane so that it could not enter a cell and to prevent shedding of the S1 part of the protein from cells into the blood.
However, Astrazeneca did not include those mutations and part of their spike protein could break off and shed out of cells as was shown in November 2020. It is not clear what difference attempts to modify the spike to prevent cell entry made given that the spike protein message was being delivered directly into cells using the various vaccine delivery systems.
5.6 Allowing approval of one product based on data from another product
There is a saying among people who produce biologics as therapeutics that “the process is the product”. This is because slight changes in component parts or the manufacturing process can have profound, clinically meaningful impacts on the end product. In the Pfizer/BioNTech trial their product was made using only the nucleotides needed to build the DNA and mRNA and the reagents that allowed that to happen. This was process 1.
The product given to the public was made from a DNA template that was mass produced using vats of bacteria. The trial data was collected up until 14th November for submission to regulators which led to the initial approvals. However, the mass produced product was only introduced into the trial from 19th November 2020 and only 252 participants were given it in the trial. A plan was added to the protocol to compare four manufacturing sites with a control group (presumably the process 1 from the trial). The control group was dropped from the protocol on 9th February 2021. The results from this comparison were never published and the protocol was changed on 15th September 2022 so that they no longer had to compare them. Effectively there was no trial on the product given to the public.
Figure 7: Amendments to the Pfizer/BioNTech trial protocol on 9th February 2021 showing the control group (presumably the process 1 drug) being replaced
5.7 Quality of the products
A leaked presentation on 26th November 2020 by Pfizer/BioNTech to the European Medicines Agency shows there were major concerns about the mass produced product. “Comparability between clinical and commercial material has not yet been demonstrated, which raises uncertainties about consistency of product quality and hence uncertainties as regards product safety and efficacy of the commercial product. Significant differences between batches manufactured by DS Process 1 and 2 are observed for the CQA mRNA integrity. In addition, the characterisation of BNT162b2 DS is currently not found acceptable in relation to this quality attribute. This is especially important considering that the current DS and DP acceptance criteria allows for up to 50% fragmented species.” The result of identifying this problem was to increase the allowable level of fragmented mRNA to 60%. Leaked emails showed the original product had a RNA integrity of 78%.
On 26th November 2020, the EMA noted that the manufacturing sites were not compliant with Good Manufacturing Practice.
5.8 Differences between the process 1 and process 2 products
A submission to FDA said they expected these participants to have worse adverse reactions. Placebo trial participants may have had process 2 products. Adverse reactions were indeed about twice as common. “As expected, in comparison to participants randomized to BNT162b2 from Dose 1 to the unblinding date, [the rate of adverse reactions] for participants who originally received placebo and then received BNT162b2 are greater… than…for participants who originally were randomized to BNT162b2”
Figure 8: Tables from FDA submission showing the incidence ratios (IR) per 100 person years for any, related and severe adverse reactions. Table on the left shows figures for the process 1 product and on the right for process 2.
There were several indications that the product made in process 1 was quite different to the mass produced process 2 product:
- The booster trials used process 2 product and had a 5.2% rate of lymphadenopathy compared with only 0.4% for the process 1 product given for dose 1 and dose 2.
- Trial data had more male adverse reactions whereas all real world data has significantly more female reactions.
Figure 9: Periodic Safety Update Report: Dec 2020 – June 2021
Pfizer suggested a post-approval study to compare lots. In January 2021 a protocol was registered for them to test four different manufacturing lots with a “control lot” (presumably process 1). In February 2021 the control lot was removed from the comparison. There has still been no comparison of process 1 and process 2 products. The comparison between process 2 lots did show adverse reactions from the EU processing plant were twice as common 10% vs 5.5%. There should not be this huge variability between manufacturing sites. It is indicative of poor consistency in production.
5.9 DNA contamination
Moderna filed a patent in 2014 which said that the DNA template must be removed as it was a cancer risk and proposed a method for doing so. They also suggested a novel method for measuring the residual DNA which may not be detected with standard testing.
A second Moderna patent filed in 2018 said “introduced DNA can integrate into host cell genomic DNA at some frequency, resulting in alterations and/or damage to the host cell genomic DNA. Alternatively, the heterologous deoxyribonucleic acid (DNA) introduced into a cell can be inherited by daughter cells (whether or not the heterologous DNA has integrated into the chromosome) or by offspring.”
There were issues with purification and when tested the mass processed drug contained high levels of DNA (from the bacteria) which were contaminants from the process 2 manufacturing. This DNA included sequences that Pfizer had failed to alert the regulators to. The presence of a region of DNA derived from the SV40 virus that is responsible for signalling the production of a neighbouring sequence had not been disclosed. DNA is more likely to integrate into human DNA than RNA would be. Fragmented DNA, as this was, increases the chance still further as each fragment could integrate.
There are other five separate aspects to the way the product was made that would maximise the possibility of integration into human DNA. The extent of this problem has not been measured.
It is possible that contaminant toxic endotoxins from the bacterial cell wall were also present. These can cause a vast array of harmful effects from anaphylaxis to cardiovascular disease and clotting to capillary leakage syndrome.
5.10 Failure to insist on a submission for the molecule in question
Even the molecule that was used in the trial was changed half way. Because of the concerns about antigen dependent enhancement Pfizer/BioNTech started off investigating a molecule that only contained the receptor binding domain – BNT162b1 (as opposed to BNT162b2 which was the whole spike protein and what they ended up using). Up until 8th June 2020 no human had been injected with the b2 molecule. All laboratory, animal and early human work was being done on the b1 molecule.
In theory pre-clinical and early clinical studies should determine the choice of molecule. In practice, on 22nd April 2020 when only one preclinical study had completed and only four out of a further fourteen were underway, BioNTech issued a press release which said “We are pleased that the preclinical studies in Germany have been successfully completed and that we will soon begin this first human study earlier than expected.”
The first human study on the b1 molecule was published on 1st July 2020 as a preprint. It covered people who had been injected between 4th May and 19th June. Seven weeks later a preprint claimed to present the results for 72 people who had been injected with the b2 molecule over a similar time period from 4th May to 22nd June. They claimed a total of 35 days follow up for safety testing and that the level of adverse reactions for both groups was similar. Other documents show that these claims cannot have been true. The records of which participants were injected and when show that it was not until the 8th June that anyone was injected with a 10 microgram dose of the b2 molecule and on 9th the first human was given a 30 microgram dose. Prior to that date only the b1 molecule was being used. Separate documentation that tracked batches in the trial stated that the first dose was not given until 15th June 2020. In either case there was insufficient time to have 35 days follow up on 72 people.
A BioNTech protocol amendment states in a section labelled “up to June 22nd 2020” that “Most recently dosing has begun with vaccines BNT162b2… Early indications for tolerability of BNT162b2 at a 10 µg dose are very encouraging.” The only data presented in this section was on other molecules and there were four instances of the phrase, “For logistical reasons, investigation of the different vaccines may not be able to start at the same time.” There was a mention of dosing of the b2 molecule but only in 43 individuals not 72.
Despite the earliest evidence of a human being given the 2b molecule being 8th June, two days later Pfizer reported that they were already manufacturing the vaccine at risk in order to have enough supply (page 14). Unless they were manufacturing only empty lipid nanoparticles and vials to put them in, then they were making something with no evidence as to its actions in a human. By 24th July, the protocol was amended to select BNT162b2 for the major phase 3 trial and on 27th July they announced the choice of BNT162b2 for their product, only 46 days after the first person had been injected with it.
The evidence, when it finally was available, indicated that for the same doses the b2 molecule resulted in more adverse reactions than b1.
Fauci’s department, the NIAID, owned a patent on this design and Moderna also used that patent. Individuals within his department received royalties for the vaccines. The department received a $400 million “catch-up payment” in quarter 4 of 2022 alone. By the end of 2022 $1.74 billion had been given in third-party Royalties.
5.11 Failure to understand which proteins would be produced by the body
The vaccine products were all pro-drugs i.e. drugs which are not themselves the active ingredient but which are converted into the active ingredient in the body. It is imperative with such a drug design that not only is there a full understanding of how much drug is produced and where but also what exactly is produced.
There were major problems with the mRNA product which led to the production of any number of unknown proteins whose impacts are also unknown.
Smaller proteins were also being produced. The submission to the Australian regulator should have shown a clear spike with one size of RNA but the graph of the quantity of RNA plotted against the size of the RNA showed a clear hump with smaller RNA sequences being produced:
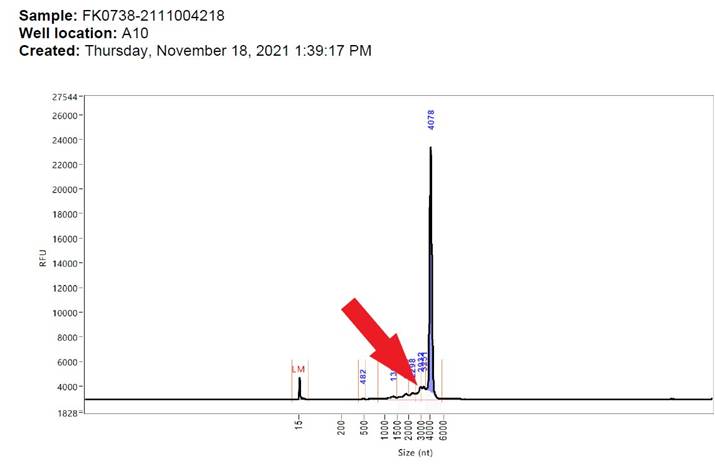
Figure 10: Mass spectrometry of RNA contents of vaccine showing amount on y-axis and size of sequences on x-axis
mRNA sequences are used to code for proteins but it is the folding of these proteins which produces a unique shape which interacts with the body. It is electrostatic charges between different protein building blocks (amino acids) which drive this folding. A shortened sequence will fold in a different way to produce a different shape with different properties.
The EMA wanted evidence of what proteins were produced, “the possibility of translated proteins other than the intended spike protein (S1S2), resulting from truncated and/or modified mRNA species should be addressed and relevant protein characterization data for predominant species should be provided.”
In the event, alternative proteins were being produced. The modification of the RNA resulted in unreliable translation of the sequence. Amino acids are coded for by three letters of code. The unreliable translation resulted from one letter in the code being skipped such that the three letter groupings became almost random and a totally new protein would be produced. The study only looked for antibodies to one of the possible alternative proteins that may have been produced and found it in a third of subjects.
a. Measuring the size of proteins produced
Testing could be done in order to understand what proteins would be produced. Instead of using the latest technology i.e. proteomics, to understand this fully an old technique from the 1970s was employed. The technique has parallels to chromatography with different sized proteins being separated as they travel across a gel. The proteins are then demonstrated by staining.
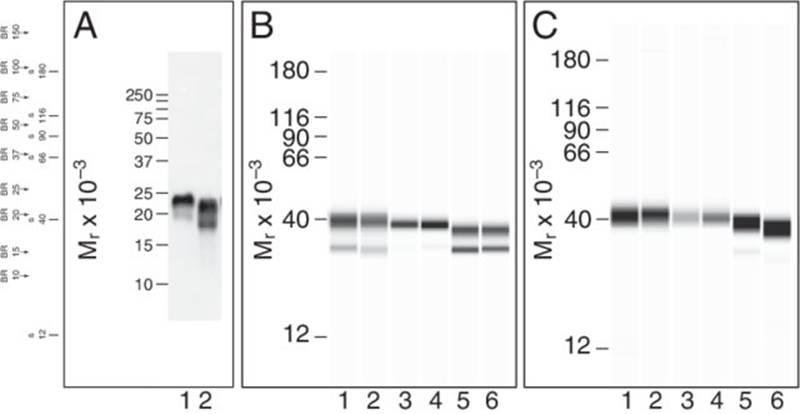
Figure 11: A conventional western blot (far left) alongside automated western blots – note variation in intensity of staining, blurring at bottom and top of each band and fainter bands beneath main band in some columns
A choice has to be made between whether to carry out general staining of all proteins present using a dye or broad spectrum antibodies or whether you want to use a specific antibody to demonstrate the presence of one particular protein. It appears the regulator accepted the latter approach and remained unaware of the extent of the risk of smaller proteins being produced.
The submitted results of this testing were not the raw results (which would show the non-uniformity as shown in figure 11 above) but a machine reading of those results (see figure 12 below). Figure 11 shows four different samples which were each used at 6 different concentrations corresponding to each column. Each band should have a unique level of intensity as it would be highly unlikely for cells to have produced exactly the same amount of protein that was then diluted to the exact same degree.
Figure 12: Western blot machine readout submitted by Pfizer to demonstrate proteins produced after vaccination (page 39 of this reference)
Image analysis has shown that the bands on the submission do not show the expected level of variation. Instead of 48 unique bands, the intensity is identical for multiple bands suggesting the image was created through copying and pasting of the bands (see figure 13 for image analysis results).
Figure 13: Image analysis of the Pfizer submission of the western blot with intensity measurements of the two rows of protein bands colour coded to show which are identical
In the same document on page 80 is another western blot. Here process 2 products were tested against a control batch called “20Y513C101”. This batch and a batch called “R427-p0202DS” were both present in the Western blot from page 39 (see figure 12 above). However, whereas the first image clearly shows two bands with a molecular weight approximating 180 and 230 kDa, in the later image the same products now have a molecular weight of 230 and 130 kDa (see figure 14 below).
Figure 14: Further Western blots submitted by Pfizer/BioNTech on page 80 comparing process 1 and process 2 products
5.12 Reducing the regulatory bar even further since original approvals
Rightly, approvals for drugs in children have to reach a higher regulatory bar for evidence of safety. Before drugs are approved for use in children, they typically undergo extensive testing in adults to establish their safety and efficacy. The data from adult studies help inform the development of Paediatric Investigation Plans (PIPs), which are required for paediatric drug approval. These plans ensure that the drugs are specifically studied and developed to meet the safety and efficacy needs of children. For vaccines there needs to be extra caution because any benefit from existing vaccine programmes is risked when an unsafe vaccine is rolled out.
Instead of raising the standard, the children’s vaccines and the boosters were subjected to even less robust approvals than the original vaccines.
a. Antibody levels as a surrogate
The government wording says, the product aims “to generate neutralising antibodies, which may contribute to protection against COVID-19.” Although antibodies correlate with protection there is no level of antibody which guarantees protection.
b. Children’s trials
To reiterate, it was always unethical to run any trials on children with these drugs as they had negligible ability to benefit even from a miracle drug. In adults Omicron is only half the threat of previous variants.
Furthermore, interfering with their natural immune response would mean that children do not develop a broad response giving them the most protection against all future variants. This would make them more vulnerable when they are older and the risk from the disease is higher.
Worse, there is evidence of a complex functional reprogramming of the innate immune response essential for protecting children from all infections.
Animal studies including on genotoxicity, reproductive toxicity and carcinogenicity were not done before these drugs were approved for injection into children.
The trials for children were never of sufficient size to measure adverse reactions in a meaningful way.
i. 12 year olds and over
The trials were too small to measure efficacy for severe covid or safety. Assumptions that there was a benefit were therefore based on the antibody levels in the blood and the fact there were 9 more cases in the placebo group in a seven day period after the second dose.
ii. 5-11 year olds
The Pfizer/BioNTech drug was given full authorisation under the name Comirnaty for children 5 years and older based on an analysis carried out by the European Medicines Agency and adopted by the MHRA. In order to prevent a single hospitalisation or a single death vast numbers of children would need to be vaccinated. The JCVI calculated this for five to eleven year olds and estimated that vaccinating every 5 to 11 year old child in the country (nearly 6 million of them) might prevent three intensive care admissions. They also caveated the potential benefits saying, “The extent of these impacts is highly uncertain.”
Again it was based on antibody levels and a tiny difference in case numbers after more than a week from the second dose for an unspecified period. On approving the drugs for this age group the MHRA commented, “These data demonstrate a favourable safety profile compared with that seen in other age groups.” No mention was made as to the massively different benefit risk ratio for different age groups.
The WHO minimum requirement for defining a vaccine as effective is that the measure of vaccine efficacy be greater than 50%. On page 144 of the Amendments to the protocol there was an amendment on 29 September 2021 which says “revised the success criterion for the efficacy hypotheses to the lower limit of 95% CI >30%, in response to regulatory feedback.”
After two doses the side effects after two doses were “injection site pain (> 80%), fatigue (> 50%), headache (> 30%), injection site redness and swelling (≥ 20%), myalgia, chills, and diarrhoea (> 10%).” In real world testing 8.8% of children “could not complete daily activities” after vaccination. The risk of experiencing such symptoms from infection only occurs if you catch the virus. These risks were for everyone who was vaccinated.
iii. Under 5 year olds
At the time of approval it was known that effectiveness lasted only 6 weeks in 5-11 year olds before the risk in the vaccinated became higher than the unvaccinated. There were only 6 covid attribute deaths in 1-4 year olds in England in all of 2020 and 2021.
Moderna
At the time of authorisation Moderna had been dropped for use in under 30 year olds in Sweden and for under 18 year olds in Denmark.
The follow-up period after the second dose for Moderna was a median of only ~70 days. This is extremely short, especially when compared to international guidelines that recommend at least one year of follow-up for vaccine trials.
The efficacy of the Moderna vaccine was estimated to be only 37% for 2-4-year-olds. This rate is below what is typically considered acceptable for vaccine efficacy.
Local and systemic side effects were common, especially after the second dose. Moderna only disclosed the severe adverse events, including a case of Type 1 diabetes, in the supplementary appendix of their study.
Pfizer
The study was approved on the basis of 4,526 participants but 2,750 of them had not completed the trial when the approvals were made.
The trial using the original protocol showed no benefit from vaccine. The protocol was altered to add a third dose before a claimed increase in antibodies to Omicron resulted.
In the meantime, many children in the placebo group had been vaccinated 6 months after their first injection (a strategy that destroys safety data) so a new placebo cohort had to be recruited to compare the third dose.
The median duration of blinded follow-up for participants aged 6-23 months after the third dose was only 35 days and for 2-4 year olds was 40 days.
The antibody levels produced after three doses against Omicron variants were far lower than against the Wuhan variant (slides 31 and 32).
There were 30% more covid cases in the vaccine arm in the three weeks after first dose, The children who had covid between the first injection and one week after the third injection were not included in the analysis. In the end 97% of the covid that occurred in the trial was ignored (table 19 of reference). The efficacy claims were based on the infections in a total of only 10 children (slide 36 of reference).
Children do not get severe covid so they defined severe illness as children who had an increased heart rate or breathing rate and then reported “Seven cases in participants 2-4 years of age met the criteria for severe COVID-19: 6 in the BNT162b2 group, of which 2 cases occurred post unblinding, and 1 in the placebo group.” Rather than showing evidence of benefit this appears to show the opposite and could indicate an antigen dependent enhancement where the immune response to infection is detrimental after vaccination and is a known risk of coronavirus vaccines. Twelve children had multiple episodes: all were vaccinated.
There were three children who had a serious fever with seizures and all were in the vaccine group.
In their own submission Pfizer concluded:
“The uncertainties associated with benefits of the Pfizer-BioNTech COVID-19 vaccine when used in children 6 months through 4 years of age include the following:
- Duration of vaccine effectiveness: the blinded, placebo-controlled evaluation period for descriptive efficacy analyses was limited, and waning of protection following a primary series has been observed in older age groups.
- Need for a booster dose: based on experience with adults, it is likely that a booster dose will be needed in addition to the three-dose primary series to increase robustness, breadth, and duration of protection
- Benefits in individuals previously infected with SARS-CoV-2: descriptive post-Dose 3 efficacy analyses do not include cases in previously infected participants
- Effectiveness in preventing post-acute sequelae of COVID-19: available data are not conclusive
- Future vaccine effectiveness as influenced by characteristics of the pandemic, including emergence of new variants
- Vaccine effectiveness against asymptomatic infection and transmission…Available data also do not indicate high-level or durable effectiveness against transmission.”
iv. Moderna Bivalent booster
First, Moderna showed that its new Omicron-specific vaccine, when used as a booster in Macaque monkeys, gave only a boost to their previous vaccine immunity but failed to invoke antibodies against the new Omicron strain.
Moderna bivalent booster was approved based solely on antibody levels in the blood, in a trial which included only 437 people. Of those given the Moderna BA1 booster there were 11 who tested positive for covid after more than 14 days from vaccination and 5 of these were symptomatic. That compared to only 5 in the control group (given a repeat of the original Moderna dose), only one of whom was symptomatic. These findings appear to have been ignored even though they were published alongside a table that the MHRA replicated in their own analysis. Almost every systemic side effect was reported more often for the BA1 booster. One in ten people who received the Moderna BA1 product had to consult with a doctor within a month. Approval was given despite a lower efficacy in preventing Covid-19 than the original vaccine and the MHRA concluded, “No new safety signals were identified.”
c. Pfizer/BioNTech BA1
The Pfizer-BioNTech BA1 product was tested on 610 people who had had three doses of the Wuhan product. They were divided into a group that received a fourth Wuhan product and a group that received the Pfizer-BioNTech BA1 product (305 in each group). The results for almost half of these people are not disclosed, nor are the reasons why the subjects were excluded from either group given, which would ordinarily be regarded as essential in evaluating the results. The table showing the rise in antibodies (table 2 of this reference) shows the results for only between 50% and 60% of the people given the product. It is worth noting that the levels of antibody after the Pfizer-BioNTech BA1 product that neutralised the original strain are almost ten times higher than the levels produced against Omicron. No data from the trials is available to the public.
Figure 15: Annotated table 2 from government report on Pfizer-BioNTech BA.1 product showing results for 50-60% of those in study
The MHRA produces safety Public Assessment reports which are said to “explain our assessment of the scientific evidence used to lead to regulatory decisions on the safety of medicines or medicines classes.” The release of the Public Assessment report for the Pfizer-BioNTech BA1 product contained no research evidence at all. It said, “MHRA decided that the benefits are greater than the risks and recommended that this medicine/these medicines can be approved for use.” and “The quality of the product is acceptable, and no new non-clinical or clinical safety concerns have been identified. The benefit/risk balance is, therefore, considered to be positive.” Again safety was only measured for conditions the manufacturer included in their survey. It was compared to previous doses and then waved through because there were “no new adverse reactions.”
d. Moderna BA.4/BA.5
The only data on this product was from testing 10 mice and measuring their antibody levels and showing they were similar to mice given BA1. All 10 contracted covid after receiving the product. 511 people were to be injected and antibody levels measured in a trial that was ongoing at the time of approval.
e. Pfizer BA.4/BA.5 booster
Pfizer BA4/5 bivalent booster was approved based largely on the data from testing the BA1 vaccine, which is a different vaccine.
The only data on this product was obtained from studying 8 mice and measuring their antibody levels, and showing they were similar to mice given BA.1.
There has been no human trial carried out by the manufacturers. The decision to approve was based entirely on extrapolating from the data used to approve previous vaccines (data which is not in the public domain for the Pfizer-BioNTech BA.1 product).
A study the MHRA did not reference has shown that a quarter of healthcare workers could not attend work after receiving the Pfizer-BioNTech BA.4/BA.5 product compared to 10% for the original product. 85% had an adverse reaction of some kind compared to 51% for the original product.
The MHRA said, “The updated booster vaccine is the second bivalent vaccine from Pfizer/BioNTech to receive MHRA approval, after it was found to meet the UK regulator’s standards of safety, quality and effectiveness. The vaccine has been approved for use as a booster dose in individuals aged 12 years and above…The MHRA’s decision is based on all available evidence on the original Pfizer/BioNTech COVID-19 vaccine and its adapted vaccines”
In November 2022, when asked to provide evidence that the post marketing authorisation conditions had been met, the response was, “the safety profile and efficacy of the products are now considered comprehensively characterised and meet the requirements for conversion to a full Marketing Authorisation and that the remaining conditions could therefore be downgraded to Risk Management Plan or Post-Authorisation Measures.”
5.13 No insistence of thorough safety testing in trials / obliteration of the Control Group
The Chief Medical Officer of Moderna,, Tal Zaks said in March 2020, “I don’t think proving this in an animal model is on the critical path to getting this to a clinical trial.”
The original AstraZeneca protocol had been for a placebo controlled trial including two groups, 1b and 2b, who would receive a saline placebo. Within a week this was changed to a meningococcal vaccine and by the 20th April version the words “placebo controlled” had been removed.
The trial was paused twice because of serious safety concerns. The first time was in July 2020 when a patient developed multiple sclerosis and the second time was in September when a participant developed transverse myelitis. A further study to look only at safety issues was cancelled at this point.
Overall at the time of first approval the interim study had reported 7 adverse events affecting the nervous system in the vaccine group compared to 4 in the placebo group (the groups were of equal sizes in this study). The vaccine group had a case of multiple sclerosis and one of transverse myelitis.
The second phase 3 trial reported 23 participants with adverse events affecting the nervous system in the vaccine group, including facial paralysis, Guillain-Barre syndrome and other rare demyelinating conditions. They reported only 3 in the placebo group (that had half as many people). Overall therefore there were four instances of demyelinating disease in the two trials from 33,608 people, or 1 in 8402, only one of the potential adverse reactions. In the meantime, the claim regarding efficacy was that 1 in 11,203 would need to be vaccinated to prevent a covid attributed death.
5.14 Assumption that all safety issues would be evident within a few days of vaccination
Because much of the harm can be caused by inflammatory or immune responses the adverse reactions may not occur immediately.
When the Pandemrix vaccine caused the lifelong disabling condition narcolepsy in more than 100 British teenagers in 2010, it took an average of 8 months from injection to diagnosis and it took three years for Public Health England to acknowledge a problem and ten years to measure it accurately.
The regulatory requirements for safety testing and the systems in place for adverse event monitoring are all designed to detect adverse events (from vaccines) that occur within a short time frame. Therefore, there is systematic lack of awareness of issues which occur after a longer period.
The AstraZeneca protocol changed over time. The original trial end date was May 2021 which included 6 months follow up and a further optional one year follow up. From September 2020, the follow up was extended to 15 months from enrolment and the end date was pushed back from May 2021 to October 2021. But this was not to enable discovery of safety issues. The new protocol said serious adverse events would be followed up “until a cutoff date of 1st July 2021 or 6 months post late vaccination visit, whichever is latest.” The 6 month follow up only applied to serious adverse events in their questionnaire (pain, redness, warmth, itch, swelling, induration, tenderness, fever, chills, joint pain, muscle ache, fatigue, headache, malaise nausea). The real concern is for serious adverse events not included in their questionnaire but reported by participants.
The original protocol called for only 28 days of follow up and the newer protocol had shorter follow up in some instances saying “Occurrence of unsolicited adverse events (AEs) for 28 days following vaccination (7 days following vaccination for groups 1c, 1d, 5a & 5b).” Seven days is inadequate follow up to assess safety.
5.15 Ignoring alerts from systems designed to spot safety problems
The WHO’s Vigiaccess reporting system contains 5,233,659 reports of any adverse event after any of the covid vaccines. Of 500,000 Germans surveyed, 1 in 500 had a Serious Adverse Event (SAE) for Pfizer that would include coincidental illness. By September 2022, the German Ministry of Health data showed 1 in 3,300 recipients had a report submitted by their doctor who had a concern the SAE was caused by the vaccine.
In Norway, doctors are obliged to report adverse events, and the Norwegian reporting system showed that doctors reported serious adverse events at a rate of 1 in 200 doses for AstraZeneca, 1 in 1862 for Moderna and 1 in 2325 for Pfizer-BioNTech. In Iceland there have been serious adverse event reports in 1 in 833 vaccinated people.
The US vaccine adverse events reporting system has been forced to release its data which shows signals of harm for 770 separate conditions two-thirds of which were a stronger signal than for myocarditis and pericarditis which has been acknowledged as a genuine adverse event since mid 2021. Examination of the above shows that the adverse events are extremely widely distributed across many symptoms and organ systems.
The fact that reports have been so varied has caused some to dismiss the high number of reports to the Yellow Card system (the UK adverse event reporting system) as being due to heightened awareness of the system. However, Dame June Raine presented data showing that the rate of reporting for other drugs had fallen in the same period of time.
The MHRA set out a plan for safety monitoring which included doing prospective surveys. None have been published.
5.16 Ignoring anomalies in trial safety data
The recorded serious adverse events showed a marked spike in the placebo group even though it was only saline. A higher rate will be expected in the first three weeks as both first and second doses are counted in this period, however it should not be as high as it is. There needs to be an explanation for this. Was the placebo really saline? Was there a bias or data manipulation that affected the recording of events?
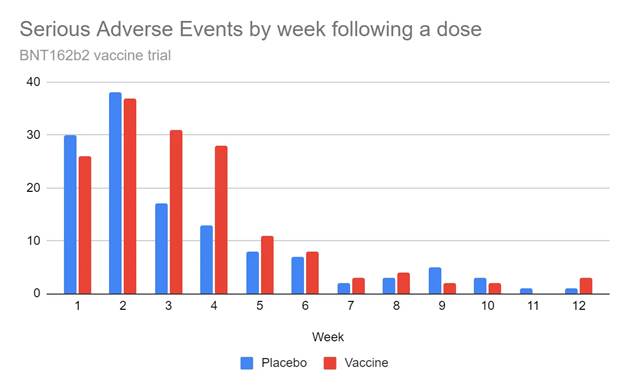
Figure 16: Number of recorded serious adverse events by week after first or second dose in placebo and vaccine group in Pfizer/BioNTech trial
There were 13 reports of palpitations among under 55 year olds in the placebo group. Palpitations have been commonly reported after vaccination and yet there were only two reports in the vaccine group. The effect of this is to obscure the marked difference in other cardiac events between the two groups with 28 in the vaccine group and 18 in the placebo group.
Figure 16: Reported cardiac adverse events in the vaccine and placebo group
Maddie de Garay was a participant in the adolescent Pfizer/BioNTech trial and suffered a severe adverse reaction. However, this was simply recorded as abdominal pain and functional disorder.
Augusto Roux was a 35 year old lawyer at the time when he became a participant in the Pfizer/BioNTech trial at the Argentinian site. He was hospitalised with pericarditis 3 days after dose 2. His trial notes incorrectly described the problem as “bilateral pneumonia” and later it was coded as covid despite him testing negative. He was excluded from safety and efficacy data that way.
When Augusto pushed to be given access to his trial records, an entry was added in the trial notes claiming he had “mental health problems.” One of the nurses who cared for him described seeing quite a number of patients who had participated in the trial. 2 days after Augusto Roux was vaccinated there were 52 vaccine participants given too large a dose. These people were unblinded a week later and 31 of them did not get a second dose. Of the 23 who did, 4 had a significant adverse event. There was a significant problem with missing data which could have distorted the safety measurements. Participant numbers are issued consecutively by machine. 301 numbers are missing from the final data with no explanation. The site in Argentina had 12% of participants but 37% of missing participant numbers. That is four times the rate of missing numbers at all other sites combined. 99 of the gaps had more than one missing number. There were 17 missing subject numbers on day Augusto Roux was vaccinated
Figure 18: Spreadsheet of participant numbers from the trial showing missing numbers in red
5.17 Allowing the destruction of the control arm ruining proper safety assessment
When a new drug or medicine enters phase 2-3 clinical trials, these normally involve keeping active treatment groups and placebo groups separate for a minimum of one year, more commonly for 2 years so that any medium to long term adverse effects can be elucidated prior to widespread use.
Premature unblinding and cross over was justified on the basis that participants might withdraw from the trial to ensure they had been vaccinated. Allowing this crossover resulted in 89% of the trial placebo group, who were disproportionately young, being vaccinated when only 35% of the US population as a whole had been. Consequently there was only 97 days follow up on average.
The decision to ‘unblind’ the trials and offer vaccination to the placebo group after only a few months has made the whole process of assessing safety and indeed efficacy extremely problematic.
5.18 Failing to withdraw the vaccines on safety grounds
There has been plenty of evidence to justify withdrawal of these products and the MHRA have failed to act. The evidence was articulated publicly earliest for the AstraZeneca vaccine and yet the MHRA failed to withdraw it instead relying on the JCVI changing its recommendations. Worse, the MHRA approved the AstraZeneca vaccine as a booster vaccination in September 2021. Somehow its use was restricted once it was known to be unsafe, but it was not the MHRA who was responsible for this.
Figure 19: Use of AstraZeneca vaccine compared to Pfizer vaccine in UK
In stark contrast the MHRA withdrew pholcodine-containing cough medicines in March 2023 “following a review which found that their benefits do not outweigh the increased risk of the very rare event of anaphylaxis to neuromuscular blocking agents (NMBAs) used in general anaesthesia.” For people who took the medicine AND then had a general anaesthesia the risk was 1 in 10,000. For covid vaccines – even if you had a known history of anaphylaxis, the advice was to give the drug “under supervision”
5.19 Batch issues
There is a phrase in the industry that “the manufacturing is the product”. The WHO hinted at this when they said, “It is considered that mRNA vaccines are to be regulated as biologicals, and like other biologicals, adequate control of the starting raw materials and manufacturing process is as important as that of the final product.”
Certain batches of vaccine have had a much higher adverse reaction and death rate than others. A Danish study showed the rates of reports per dose fell into three categories of batch with high, medium or low adverse events. The authors claim to have replicated this finding on Swedish data.
One batch of Pfizer-BioNTech resulted in the hospitalisation of 120 children in Vietnam. There are four potential reasons for this problem.
- Nucleic acids like DNA and RNA can form clusters like cotton wool balls in solution which means that it is hard to ensure each sample from a vat has the same quantity.
- The vats of mRNA vaccine contained lipid nano-particles which float and stirring risked damaging them.
- Against MHRA regulations, vaccine dilution was carried out manually in vaccine centres.
- There were concerns that ineffective cold storage would mean that for some batches the mRNA would have degraded before injection.
- In February 2021, the requirement for -80 degree freezing was disregarded
- Expiry dates were extended by a year
The Pfizer contract did not permit testing of lots. A clause was included that the purchaser should grant an exemption of “applicable laboratory or quality testing” which otherwise “would prevent Pfizer from supplying and releasing the product.”
Lot testing was carried out by the National Institute for Biological Standards and Control, an expert centre of the UK’s Medicines and Healthcare products Regulatory Agency. A paper described their methods used. It was caveated with terms such as “ordinarily,” “typically” and “usually” but did claim that they did physically test vials separately to the manufacturer’s testing.
The MHRA answered an FOI about testing lots after receiving Yellow Card reports. They responded:
“At the behest of the MHRA (DMRC) some vials were received by NIBSC for a visual inspection test. The visual inspection test itself is not invasive – it is a review against two monochrome backgrounds to observe particulate matter visible to the naked eye – the content (composition) of a vaccine is not examined. For routine independent batch testing, sampled vials must meet the specification stipulated in the licence approval for this test for the batch to be considered for certification by NIBSC. Only batches with a certificate can be marketed by the manufacturer. The visual inspection test was performed and photographs taken…example images from two vials are indicated in the two panels below, to illustrate test observations. All vials held were subsequently dispatched so that the manufacturer could use them in their own investigation.”
Figure 20: Image from MHRA demonstrating non invasive visual inspection of vials against a light and dark background
5.20 Bias in the covid trials
a. Causes of bias
It is critical that both those administering the drug and the participant are unaware of whether they are in the vaccine or placebo group as knowledge of groupings has been shown to affect results as it can bias:
- Testing in event of symptoms
- Death reporting
- Exclusions
Pfizer/BioNTech described their trial as “observer blinded” however their protocol states that the following people were not blinded
- Clinicians
- Clinical research associates
- Study manager
- Statisticians
- Laboratory staff
Whistleblower, Brook Jackson, who worked at Ventavia, a subcontractor for Pfizer-BioNTech’s trial site, claimed there was fraud involving falsified trial data, unblinding of patients and staff, and a failure to follow up on reported side effects.
All the PCR testing was carried out in one central laboratory. PCR testing is not easily replicable from site to site. Arguably this was a reason to justify centralised testing. However, having a single laboratory for all global trial testing where the laboratory staff are not blinded, gives an opportunity for bias in the testing results. The cutoff used by the central laboratory to call a positive was never disclosed and the Ct values – which would indicate how weak or strong a test result was for those participants who were positive – was also not disclosed to regulators.
b. Evidence of bias
When people had symptoms the vaccinated were less likely to be tested in the local laboratory (so less likely to be counted as “cases”) e.g. 25/169 (15%) symptomatic vaccinees were tested at site 1226 vs 61/245 (25%) placebo with a similar picture at numerous other sites. Vaccinated participants with positive local tests were less likely to have positive central tests (83% vs 57%). 87% of symptomatic placebo participants had a test result returned from the central lab before the cut off date compared to 84% for the vaccinated. There was a difference in time from death to report of death:
- Placebo: Median of 5 days before cutoff for submission and 3 days afterwards
- Vaccine: Median 18 days before cutoff for submission and 7 days afterwards
One third of deaths in the placebo were attributed to covid – demonstrating a bias. Almost all of these were not included in the efficacy results as they did not fit the criteria. Two placebo deaths were included even though they should have been excluded according to the protocol:
- A 65 year old Texan man injected with Moderna after he had had his two placebo doses. He contracted covid while immunosuppressed, was in hospital within a week of injection and died 11 days later. His death was recorded as an unvaccinated covid death in the trial results even though the protocol said anyone receiving another covid vaccine would be removed from the trial results.
- A man with HIV severe enough that he did not meet the inclusion criteria for the trial was included in the placebo group as was his death from pneumonia that was attributed to covid.
Other sudden unexpected deaths were not properly investigated with barely any autopsy results and the regulators did not insist on better investigation of deaths.
c. Failing to pay attention to secondary efficacy results
The primary endpoint was symptomatic PCR positive people but there was an important secondary measure of who developed antibodies after an infection (N antibodies as opposed to the S antibodies induced by vaccine). The regulators failed to note the significance of this result.
The claimed result based on PCR positives was 8 cases in the vaccine group and 162 in the placebo group more than a week after the second dose. The antibody results showed 75 vaccinated people had had an infection compared to 165 in the placebo group.
The antibody result is for the whole period not just the time more than one week after the second dose and yet there were only three more placebo participants with evidence of an infection suggesting a major bias in overcalling placebo PCR cases.
Using the antibody results as a measure there would be only 55% However, evidence from the Moderna trial showed that infection in the vaccinated only resulted in these post infection N antibodies 40% of the time compared with 93% of the time in the placebo group. It is likely that the presence of S antibodies from the vaccine reduced the production of N antibodies. If only half of Pfizer vaccines develop antibodies after infection in a similar way then there is no remaining evidence of efficacy.
d. Hiding waning efficacy in early trial data
Waning was noted right at the outset. Data shared with the Australian regulator in January 2021 said: “Antibodies and T cells in monkeys declined quickly over five weeks after the second dose… raising concerns over long term immunity.”
In the trial 12 people who were enrolled early on underwent frequent antibody testing. Their results were only provided up to 24th August 2020, meaning nearly 3 months of data was not presented. There was a clear fall after 28 days. These results were presented on a logarithmic scale e.g. the drop for the 30 microgram dose was to 60% of peak levels.
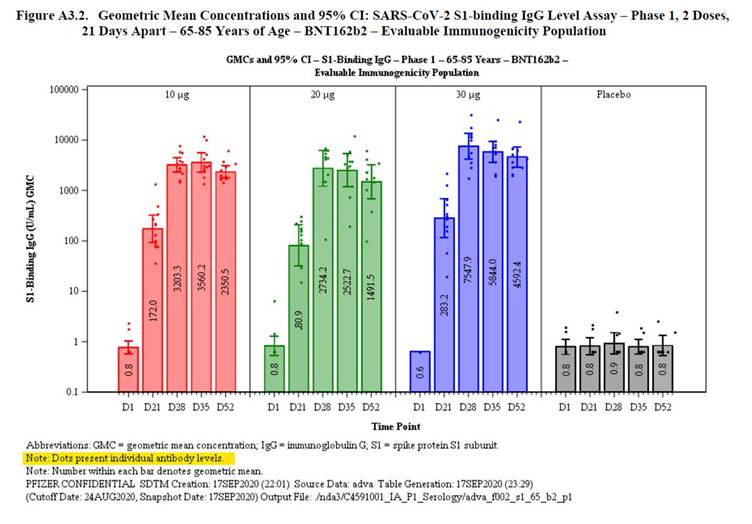
Figure 21: Antibody levels for people given different dosages by day after first dose presented on a logarithmic scale
The remaining participants also had antibody levels measured but at less frequent intervals. 1000 participants had two entries of their antibody titres on the same date after injection. Figure 22 below shows these later entries in orange and the original entries in blue. The later entries hid an apparent decline.
Figure 22: Plot of results for the 1,000 participants who had more than one entry for their antibody level measurement for the same date. Blue line shows the original entry and the orange line the later entry.
Antibody waning, after only a few weeks, was evident among the vaccinated in the real world in March 2021.
5.21 Failing to police the marketing of the products
The MHRA has a role in ensuring pharmaceutical companies and others do not breach their regulations regarding marketing of drugs as set out in the MHRA blue guide.
This guide includes the following:
- In order to perform its supervisory functions under the Regulations, the MHRA is obliged to monitor published advertisements.
- An advertisement is not limited to specific media. It includes articles published in journals, magazines and newspapers, displays on posters and notices, photographs, film, broadcast material, video recording, electronic transmissions and material posted on the internet. Point-of-sale materials, leaflets, booklets and other promotional materials that include specific product claims and which are supplied separately from the product may also be considered advertisements. Words forming part of a soundtrack or video recording are within the definition of advertisement, as is the spoken word.
- Advertisements to the general public should not contain material which refers to recommendations by scientists or healthcare professionals, or which refers to recommendations by celebrities who, because of their celebrity, could encourage consumption of products.
- Advertising which states or implies that a product is “safe” is unacceptable. All medicines have the potential for side-effects and no medicine is completely risk free as individual patients respond differently to treatment.
Figure 24: Tweets from Department of Health and Social care in December 2021 using the word safe
Figure 25: Tweets from Department of Health and Social care in October 2022 using the word safe when referencing pregnant women
- Claims that a product has a well-established safety profile are only possible once there has been extensive post-marketing experience.
Figure 26: NHS advertisement claiming full safety assessment had been carried out to same standard as other vaccines and drugs
On the day of the approval June Raine, the CEO of MHRA said “Safety is our watchword, and we are globally recognised for requiring the highest standards of safety, quality and effectiveness for any vaccine.” The JCVI also used the words “acceptably safe and effective” and those two words were repeated ad nauseam by the media and politicians.
- For written advertisements, the particulars in relation to side-effects, warnings and precautions and contra-indications, dosage and method of use and warnings should be clearly printed, legible and be placed in such a position in the advertisement to allow the reader to associate the various benefits and risks of using the product without difficulty.
- Advertising of medicines should not be directed exclusively or principally at children (under-16s). Nor should advertising material aimed at parents and carers be included in non-promotional material aimed at children.
Primary-aged children received sunflower seeds in a letter from the NHS, which was designed like a party invitation, inviting them to attend a vaccination appointment. NHS adverts directly appealed to children of that age group, encouraging them to become “superheroes.” Children were shown presentations at school of children harmed by tetanus, smallpox and polio as if these were comparable.
The UN launched its ‘Verified’ initiative in May 2020 with a stated aim “to flood digital space with facts” TeamHalo was established as part of that in October 2020 and shared videos of scientists and doctors promoting the vaccines on TikTok. A quarter of the TikTok audience is teenagers and half are under 30 years old.
Figure 27: Examples of advertisements from summer 2022 and December 2021 aimed at vaccinating children
- Caution should always be taken when medicines are used during pregnancy and that advertising should not convey messages that it is usual for pregnant women to take medicines.
- It should not include anything that could cause serious or widespread offence, create unrealistic expectations in the consumer or be misleading…A factually accurate advertisement may also be misleading due to the overall impression given.”
- An advertisement must not promote a medicine outside the therapeutic indications listed in the SPC for that medicine. This means an advertisement cannot promote a medicine for use in treating or preventing conditions or illness for which it has not been licensed.
- Advertising to the general public should not suggest that… the effects of taking it are guaranteed…Advertising should not… suggest that health can be enhanced by taking a medicine or that health could be affected by not taking the medicinal product.
- “Breach of regulation 300(1) is a criminal offence. It is also an offence for any person qualified to prescribe or supply medicines to solicit or accept any gift, pecuniary advantage, benefit in kind, hospitality or sponsorship prohibited under the Regulations. Particular care should therefore be taken when healthcare professionals are remunerated for services to ensure that there is no element of promotion.”
- Nor should an advertisement state that a product has MHRA or Department of Health and Social Care “approval”.
- The MHRA takes robust enforcement action where a significant risk to public health has been identified from advertising to the public for unlicensed or prescription only medicines.
- Any person could be viewed as promoting a medicine and proof of a commercial link to the sale of the product is not required. The MHRA will take this into account in taking any action and eventually the national courts are best placed to decide on individual cases, balancing the right to free speech against the potential for damage to public health that the law is designed to protect.
- Implications for journalists Provided they are intended to inform rather than promote medicines, articles discussing potential treatments won’t fall within the scope of the legislation on advertising medicines2 – the legal restrictions don’t prevent balanced factual reporting. But articles should not actively encourage readers to seek a particular product from their healthcare provider and must take care not to exaggerate the potential benefits. It can be hard for a healthcare provider to explain to a patient who has read about the latest ‘wonder drug’ that it is not in fact suitable for them or not yet available.
- Treatments that involve the use of unlicensed medicines may not be described as ‘clinically proven’ or similar.
- It is also recommended that advertisements should include a reminder giving information on reporting of suspected adverse reactions. For products subject to intensive surveillance by the MHRA under the additional monitoring scheme, it is good practice to include the identifying symbol (an inverted black triangle ) on all promotional material to alert prescribers to the need for special reporting in relation to adverse reactions.
- The MHRA considers that press releases should be genuinely newsworthy rather than having the intention of promoting a product… . The use of brand names should be kept to a minimum and the tone and content of the press release must be factual and not sensationalised… The MHRA also expects non-promotional items, such as press releases and risk management materials, to be submitted for review to ensure that these are not promotional.
While the 2014 edition prohibited marketing of an unlicensed drug this was amended in the November 2020 edition for public health emergencies. The US Data Safety Management Board said of an AstraZeneca press release: “The DSMB is concerned that AstraZeneca chose to use data that was already outdated and potentially misleading in their press release…[The data] they chose to release was the most favourable for the study as opposed to the most recent and most complete. Decisions like this are what erode public trust in the scientific process.”
Behavioural scientist, Patrick Fagan, pointed out how almost all the core methods were used in a single NHS text message. The message said “You have reached the top of the queue and are a priority for getting a free NHS COVID-19 vaccine. Please book yours now.” The word “reached” made people feel invested. “Top” tapped into ego and a desire for social status. “Queue” suggested popularity such that others wanted it. “Priority” suggested scarcity as well as implying VIP status appealing to ego. “Free” presents the offer as a gift appealing to human responses to reciprocate gift giving. “NHS” appealed to trusted authorities as a credible messenger. “Yours” suggests that the recipient already owns the vaccine and is claiming what is theirs. Finally, “now” conveys urgency.
Pharmaceutical companies are motivated to present data with a view to marketing their drugs. They are not (and will never be) dispassionate. Profit is the priority. This is why we have drug regulators. The regulators either failed abysmally, had conflicts of interest in their ranks that led to decisions favouring the pharmaceutical companies or failed to stand up to political pressures. This needs an investigation all of its own. Without a functioning regulator, we are in the wild west of medicine and the inevitable outcome is total breakdown in public trust, but only after a great deal of harm has been enacted on an individual level.
A complaint against Pfizer’s CEO regarding safety claims was upheld by the ABPI, the industry’s own body, but the MHRA has failed to take any enforcement action.
5.22 Other regulators
Two FDA officials resigned in August 2021. According to Politico, one former official ascribed the resignations to, “anger over the agency’s lack of autonomy in the booster planning so far. Premature and unnecessary.” They had concerns about myocarditis as well as boosters being pushed through in an unworkable timeframe. Specifically, there wouldn’t be time before 15th September for “FDA’s own analysis of the safety, effectiveness and manufacturing information.” One made clear that she believed the pressure to licence was because “states cannot require mandatory vaccination and that people hesitant to get an EUA authorised vaccine would be more inclined to get immunised when the product is licensed.“ The Comirnaty vaccine was given a full licence for over 16 year olds by 23rd August 2021.
6. PROTECTION FROM NATURAL IMMUNITY
| Any discussion of the impact of vaccination needs to be seen against what would have happened in the absence of vaccination. Natural immunity results in only ~10% being susceptible to any one variant and provides good protection from reinfection afterwards. Vaccine induced immunity was poor in comparison to post infection immunity. That does not mean that an argument could not be made for attempting to optimise immunity in vulnerable populations who were at significant risk from infection. Finally, the much reduced risk from Omicron in unvaccinated populations is of critical importance as it was missold as a benefit from vaccination. |
Only ~10% of the population was susceptible to each variant. This was evidenced by the proportion of household contacts who became ill once there was a case in the household – the secondary attack rate. Over the course of a full wave this was ~10% for each variant including the first Omicron variant.
Prior to Omicron the proportion of blood donors developing post infection antibodies was between 5-7% for each variant. Not every infection necessarily resulted in antibodies being produced. Therefore, if nothing had been done, each wave would burn out once 10% of the population had been infected. This is what happened before, during and after interventions. Because the susceptible fraction was small it would take many years for the whole population to be infected as happened with new influenza strains.
6.1 Broad Immunity
The government and WHO model was of a fully susceptible population to a “novel virus” and was based on the idea that immunity to a partly novel virus could only be achieved through exposure to that virus or vaccination. The WHO said in December 2020, “WHO supports achieving ‘herd immunity’ through vaccination, not by allowing a disease to spread through any segment of the population, as this would result in unnecessary cases and deaths.” The WHO were assuming that only immunity specific to SARS-CoV-2 could confer any protection.
The immune system’s main defence against viral infection is to kill the virally infected cells with T cells. The immune response from infection are robust and last a considerable time. T cells that kill virally infected cells were shown to “not only persist but continuously differentiate in a coordinated fashion well into convalescence into a state characteristic of long-lived, self-renewing memory.”
People who had SARS1 had T cells 17 years later that had a robust response to SARS-CoV-2. Similarly others had similar cross reactive T cells from other coronavirus infections.
Our immune systems do not recognise particular genetic sequences that are unique to particular infections. Instead, they recognise tiny parts of foreign organisms by their shapes. Rather than recognising the whole shape, different elements recognise tiny, chopped up fractions of the whole. In this way, even an apparently novel pathogen can be recognised as foreign.
Antibodies to mumps provided significant protection from SARS-CoV-2. This applied to antibodies developed after infection but was even more protective if the antibodies were acquired after MMR vaccination. Similarly influenza and cytomegalovirus infections also provided protection.
Older people have been exposed to more pathogens and have a more educated immune system. When people near the end of their lives their immune protection dies away but prior to that point older people might be expected to have better protection. Random antibody testing showed that that was the case.
Figure 28: Cumulative graph of people who have had infections by age based on antibody testing of blood donors.
6.2 Vaccine vs post infection immunity
Unlike vaccine induced immunity, natural immunity provides a memory of all the foreign proteins in the virus. Vaccine immunity focuses on only a small part of the virus. In this case it was the spike protein which is the region that mutates the most and therefore any immune response to it will quickly become outdated. Infection produced “a broader set of viral antigens of viral epitopes presented by the virus not seen in the mRNA vaccine.”
Nadhim Zahawi, then vaccine minister said “of course the virus will mutate. The more we vaccinate the more the virus will attempt to survive and mutate even further.” Children who develop this broad immune response will be better protected when they are older and at more risk.
In August 2021, an Israeli study showed that the vaccinated were 13 fold more likely to be infected than those with a previous infection in Israel. Pfizer Board Member, Scott Gottlieb, urged Twitter to censor a tweet about this study from a US government health official and succeeded in having it labelled “misleading”.
Comparing the antibody response showed, “the decay rate of antibodies in BNT162b2 vaccinees was significantly faster than that in recovered patients, suggesting that there are fundamental differences between the mechanisms of activation of the adaptive arm of the immune response following vaccine and natural infection.While natural infection involves full systemic activation, this activation may be incomplete with an mRNA vaccination, thereby affecting the capacity of the immune system to maintain an antibody reservoir over time.”
6.3 Reinfections
Of all the positive test results recorded as cases up to May 2021, only 0.4% were second positives and recorded as reinfections i.e. 99.6% of all positive results were first positives. The rate of reinfections rose to 7% with Omicron by the end of 2022 and 8% by the end of 2023.
Among healthcare workers in England prior to vaccination, those who had had a symptomatic positive PCR had a 90% lower chance of being infected. Previous infection reduced the risk of hospitalisation to that of someone ten years younger.
Healthcare workers in Oxford were followed from April to November 2020 and of 1,265 with antibodies, none developed an infection.
In the pre-Omicron era a study from Qatar demonstrated that for someone who had previously been infected, “the risk of having a severe reinfection is only approximately 1% of the risk of a previously uninfected person having a severe primary infection.” Any subsequent infection would therefore only present a negligible risk even in the vulnerable. The same authors repeated this work after Omicron and found that protection against hospitalisation was maintained at 90 percent and there were no critical or fatal covid cases in the reinfected.
There were claims that the opposite was true based on studies that relied heavily on modelling. For example, this CDC study claimed, contrary to all other evidence, that people with a prior infection were 5 times more likely to become infected than those who had been double vaccinated. The actual results from the study showed a 70% higher rate but their adjustments made this into 500%. There were other serious flaws in the study which makes even the 70% claim highly dubious. If the sample is so different to the general population that massive adjustments need to be made then effectively the study is no longer based on real world evidence. Instead it has become yet another prediction based on modelled data.
The vaccinated were more susceptible to the Delta, Beta and Gamma variants than the Alpha variant but this was not true for the unvaccinated.
A study from Iceland showed reinfections with Omicron were 42% higher in the vaccinated than the unvaccinated (despite including the single doses in the “unvaccinated” group).
6.4 Omicron
Omicron was approximately half as deadly for both the vaccinated and unvaccinated. With the first Omicron winter deaths were lower than for an average winter.This was first noted in South Africa, despite having low ‘vaccination’ rates. The first wave of Omicron resulted in lower death rates than typical for winter in Europe and USA.
It was widely believed that Omicron was indeed more transmissible. However, the transmission rate proved to be no higher when measured as the proportion of contacts infected. The reason the surges were more dramatic was because the incubation period shrank. The time to become infectious had reduced. The time until the next generation of infections also reduced and they would therefore become infectious sooner. The shortened time between infections did lead to a sharper rise in the trajectory of the wave. It was not true that people were more likely to become infected and consequently the wave fell just as sharply once all the susceptible had had an infection. A different way to explain the sharper surge was simply that there was a stronger seasonal trigger meaning more people became susceptible in a shorter time.
By 30th July 2020, there had been over 5000 variants identified out of 46,723 viruses sequenced in one study. A separate study demonstrated over 350,000 variants in under 49,000 samples. “All major clades [families of variants] in the global diversity of SARS-CoV-2 are represented in various regions of the world, and the genomic diversity of SARS-CoV-2 in circulation in different continents is fairly uniform.”
The current variants have 23 base pair mutations out of approximately 30,000 base pairs, so 0.08% of the base pairs are different from the original Wuhan sequence. If there was a significant change in shape, then protein would fail functionally and the virus would die. Small changes in shape should not affect immunity, as each individual’s immune system recognises numerous areas on each protein. The immune system does not recognise sequences but, instead, recognises the shape of the proteins that the sequences code for. Immune individuals recognised around 17 different sites on the SARS-CoV-2 virus with the population as a whole recognising over 100.
Variants can become dominant from evolutionary selection pressures or just randomly, as certain outbreaks prosper and others die away. The UK variant was said to have caused the winter surge in COVID seen across the UK. During this period, the ONS estimated that the new variant (B.1.1.7) was the predominant strain in England, but that was not the case for the devolved nations where the old variant was still predominant. In the first few days of 2021, at peak cases, the ONS estimated that the new variant was the cause of 61% of COVID cases in England; 33% in Northern Ireland; 22% in Scotland and only 5% in Wales.Despite this, and despite Wales having had their highest ever levels of disease in November and December, the decline in cases was reversed in mid-December and all devolved nations had a winter peak in line with England, but driven primarily by the old variant, not the new one.
The UK variant, B.1.1.7, was predominant in Florida in February and March 2021 and was spreading as cases dropped sharply. The fact that a variant was making up a larger proportion of cases could be due to chance alone and it is the diminishing number of total cases that is of importance to public health. A variant with increased transmissibility leads modellers to predict sharp rises in cases. Cases rising when levels of a new variant are low and then falling as the new variant becomes predominant, does not support a position of concern about the transmissibility of that variant.
7. VACCINE EFFECTIVENESS
| Claims of vaccine effectiveness have been based on trial data and real world studies in which significant modelling or adjustments were undertaken. Examination of real world data exposes the fact that many of the claims of efficacy were in fact a statistical illusion. A “vaccine” that causes the immune system to be occupied for a period, leaves people exposed to infections their immune system would normally overcome. The consequence was that the fraction who were susceptible had their cases earlier than they otherwise would have. Thereafter the illusion occurs because the “vaccinated” are protected from these earlier infections. Looking at the big picture, when it is accepted that covid was always going to come in waves affecting ~10% and not the modelled tsunami, it is clear that waves after vaccination were similar in overall impact to waves that occurred before. It was the arrival of Omicron along with changed definitions that really impacted on covid labelled hospitalisations and deaths not vaccination. |
7.1 Different vaccine platforms
a. Choice of delivery system
The AstraZeneca vaccine was a DNA vaccine using the whole unchanged spike protein sequence which was delivered into the nucleus with a viral vector. The virus chosen was unable to replicate but would be able to target cells which have the adenovirus receptor. Highest levels of the receptor are seen in respiratory, gut and liver cells but neural and heart cells also have that receptor whereas skeletal muscle cells in the arm do not. Mice biodistribution studies showed higher levels of vaccine DNA in the examined nerves than at the injection site and measurable levels in the bone marrow, liver, spleen, lymph nodes, lungs and male hearts.
The first gene therapy to use RNA delivered in lipid nanoparticles was approved by the FDA in 2018, but the first approved vaccines using this system were the covid vaccines. The patients needing such gene therapies need a working gene to be delivered to cells throughout their body, and lipid nanoparticles were therefore optimised to be able to reach every organ. However, the pharmaceutical companies found that repeated dosing led to problems with toxicity. Because of this Novartis, Merck and Roche abandoned the platform.
Katalin Karikó, vice president at BioNTech said, “I would say that mRNA is better suited for diseases where treatment for short duration is sufficiently curative, so the toxicities caused by delivery materials are less likely to occur.” Moderna and BioNTech decided to focus their technology on vaccines instead – because the prevailing paradigm was that repeated dosing is not necessary for a vaccine and the toxicity issues can therefore be avoided. The irony of this is not difficult to see.
b. Choice of molecule
Natural RNA degrades too rapidly to transport from manufacturing to administration, so synthetic mRNA, which has been designed to degrade slowly, was used in the spike-protein vaccines. No-one knows exactly how long it lasts or how much spike is produced in total. In terms of how long it is produced for in the body, studies always seem to show it still present (in a significant proportion of subjects tested) at the last time point they measure.
In terms of the amount produced:
- A widely-cited study showed that after one month it was detectable in the blood and, in one patient, in the muscle of the opposite arm after one month.
- Another study found mRNA in lymph nodes at the last time point they measured – which was 2 months after vaccination.
- One patient had spike protein from vaccination demonstrated in their shingles biopsy 3 months after their last dose.
- A large study following eight people after vaccination showed that spike protein was circulating in fatty capsules in the blood four months after vaccination.
- An Italian study showed vaccine spike present in 50% of vaccinated subjects 69 to 187 days after injection.
- An Australian study found very high levels of anti-spike antibodies – only explicable by continued spike protein production – in ALL of 29 children 6 months after their 2nd injection of the Pfizer covid vaccine.
7.2 Benefits
a. How could these novel products prevent infection?
Respiratory infections result from inhalation of viral particles which enter respiratory epithelial cells, replicate, and are then exhaled. The surface of the respiratory tract is exposed to the outside air and is protected by generalised “innate” immunity and a type of antibody unique to mucosal surfaces called IgA. The injections stimulated IgG antibodies in the blood. Such antibodies cannot stop a virus entering a cell on the surface of the respiratory tract. They could, in theory, contribute to reducing the chance of viral dissemination through the body.
Measles virus is also a respiratory virus but it replicates in the lymph nodes, so for this virus IgG antibodies from an injected vaccine does have the potential to reduce infection risk, and clinical data suggests they do. Any protection from antibodies (wherever created) cannot occur straight away as it takes time to educate the immune system. Chair of Commision on Human Medicines, Prof Sir Munir Pirmohamed said, “you have to wait until day 22 before you get partial immunity after the first dose”
A Pfizer BioNTech report to the Australian regulator said, “Antibodies and T cells in monkeys declined quickly over five weeks after the second dose… raising concerns over long term immunity.” There was therefore a very short window of time during which any potential benefit could have occurred, and any practical benefit was likely to be limited to preventing serious illness through reducing viral replication once infected and was never likely to include the ability to prevent infection. By January 2022, Albert Bourla, CEO of Pfizer admitted that “the two doses of the vaccine offer very limited protection, if any.”
b. Changed definition of a case to make vaccines appear beneficial
Over time the definition of a covid death changed from any death after a covid positive PCR, to a death within 28 days of a covid positive test in a population who were extensively tested regardless of symptoms, to only deaths where covid was included on the death certificate in an environment where doctors decided when testing was appropriate. Even then there may have been a bias towards greater testing of the unvaccinated.
Similarly, over time the definition of a covid hospitalisation changed from any person in hospital who had a positive PCR result to only those where the treating doctors believed that covid was the main cause for their admission.
In 2020, the USA had a policy of reporting only strong PCR test results as positive in the vaccinated while continuing to report weak test results as positive in the unvaccinated. The US CDC started qualifying covid deaths in the vaccinated as being “asymptomatic” or “from a cause unrelated to COVID-19.” The inquiry must investigate whether any similar policy was enacted anywhere in the UK.
US wastewater surveillance clearly shows similar levels of virus with each wave regardless of interventions. The only outlier is the first Omicron wave in December 2021 to January 2022 during the booster vaccination programme. Omicron is an “immune escape variant” meaning it has mutated to evade vaccine induced antibodies.
Figure 29: US wastewater surveillance showing levels of SARS-CoV-2 in sewage over time
7.3 Importance of what happens in first two weeks
A person sick with covid symptoms was meant to defer injection. However, it would be possible that a small number may have unknowingly been in the incubation period at the time of their vaccination and might develop symptoms subsequently. In addition, a proportion might be exposed in the early period and become infected when antibodies have not yet been produced. Overall however, because those with symptoms do not get vaccinated the rate of covid in the first two week period after injection should be lower among the vaccinated than the unvaccinated. This was not what happened.
The above hypotheses are based only on speculation whereas real world data showed that the first two weeks came with a 40 percent increased risk of covid infection. It is impossible to know how many people who were given the vaccine would dismiss covid like symptoms and not be tested; this would result in the 40% being an underestimate.
The “suspected covid” cases in the phase 3 Pfizer/BioNTech trial in the first two weeks after injection were not all tested. Even where they were tested the testing was all carried out (from 235 global sites as far away as South Africa and Argentina) in a single US laboratory and the antibody test results did not concur with the PCR test results.
The symptom tracking Zoe app study run by King’s College London was “unable to differentiate post-vaccination symptoms per se from superimposed SARS-CoV-2 infection robustly.” They showed that within a week of injection, one third of people developed symptoms which had substantial overlap with covid.
The ONS randomly tested the population with PCR and showed, “In unadjusted analyses the risk of infection increased following first vaccination, peaking at around 16 days, followed by a strong decrease to around one month… This initial increase in the number of infections following vaccinations is consistent with other studies.”
Figure 30: ONS data showing infection rates since vaccination
Public Health England showed the number of people tested each day before and after their first dose of the Pfizer/BioNTech product (BNT162b2) and the AstraZeneca product (ChAdOx-1) (see figure 31 below). Note the background rate before and after vaccination was approximately 600 per day but on the day of and after AstraZeneca vaccination it reached 800 or 1,000.
Figure 31: Number of tests in the symptomatic each day before and after vaccination with negatives coloured blue and positives yellow
Both the number of tests done and the number which were positive was far higher in the period immediately after vaccination than the period before. SAGE “observed an abundance of patients admitted to hospital within 7 days of vaccination.” Symptoms that led to hospitalisations for covid were at about 13 on days 3-5 before vaccination but around 130 immediately afterwards. This suggests a ten fold increased risk after vaccination (see figure 32 below).
One might argue that people with minor symptoms would have avoided vaccination until they were better. Equally one could argue that someone with minor covid like symptoms might have rushed to get vaccinated to improve their chances given the vaccines were said to be safe and effective. Figure 32 below shows that the number being hospitalised was increasing, not decreasing in the lead up to vaccination.
As the vaccination date approached the number of tests done in the lead up to vaccination did fall but the number of positive tests rose each day prior to vaccination, in Public Health England’s data (see figure 31 above).
Figure 32: Government data on hospitalised covid patients showing day of onset of covid symptoms compared to date of vaccination (no information was given as to how “frequency” was measured).
Given the increasing number who tested positive or were admitted each day before vaccination, that indicates that those with covid were actively seeking out injections, not avoiding them. The rate before the day of vaccination must therefore have been higher than the background rate in the unvaccinated. That would indicate that even the ten fold increased risk estimate was probably an underestimate.
Once such a huge increased risk is factored in, it is clear that the fraction (~10%) of the population who were susceptible to the circulating variant would have their infections brought forward to the period shortly after vaccination and would then be protected by natural immunity.
In this way, the period after two weeks can be used to claim vaccine efficacy with regard to infections, hospitalisations and deaths, yet as demonstrated, such efficacy is purely illusory.
Numerous researchers ignored the first two (or sometimes three) weeks after injection in their calculations. In stark contrast to these independent observations, the pharmaceutical sponsored studies all showed the vaccine group had exactly the same infection rate as the placebo group. The AstraZeneca trial even censored this period on their graphs with grey rectangles:
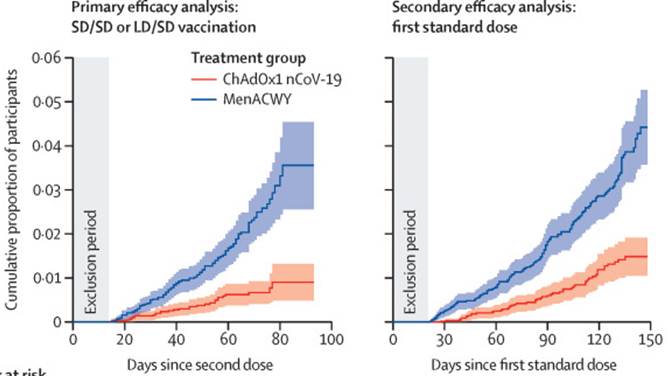
Figure 33: Cumulative covid case rate in AstraZeneca trial with first few weeks hidden with a grey box
a. Broad observations
Each covid wave globally and over time showed regional variation with differences in when rises occurred. However, the exception was the December 2020 surge where there was a synchronised rise in test positivity in every part of the UK. Even isolated islands including Isle of Wight, Anglesea and the Shetlands saw the same synchronous surge.
Surges were seen as each country began vaccine rollout starting in Israel and the United Arab Emirates. There seemed to be a critical mass of vaccination at 0.5 percent of the population per day which triggered a surge in cases. Singapore, Australia and New Zealand were the only exceptions to this rule.
Headline after headline was published reporting a massive rise in highly vaccinated countries during their rollout “despite vaccination,” first in Israel, then United Arab Emirates, Chile, Hungary and the US. The period immediately after injection also had a disproportionate covid hospitalisation and death rate as seen in data from Alberta. SAGE data also showed a higher mortality in this period in every tier of vulnerability among the hospitalised population.
Table 1: Mortality rate in hospitalised population by tier showing pre and post vaccination rates
Gibraltar was used as a test case with the claim made that they had vaccinated their entire adult population between 9th January and 18th March 2021. On 8th January Gibraltar had 12 deaths attributed to covid. The vaccines arrived by plane the next day. There were 71 new covid blamed deaths before the end of the month. More than 60 percent of all covid blamed deaths recorded on the island by the end of 2023 occurred in those few weeks in January 2021 immediately after the vaccination program started. There was minimal covid at the time in neighbouring Spain.
The government of Gibraltar reported on 27th January (stretching credulity) that:
“Of the over 11,000 who have been vaccinated, 6 persons have since died for reasons unrelated to the vaccination and there is no evidence to link these to the vaccination in any way. These 6 persons appear to have contracted covid-19 before they were vaccinated but, despite testing for covid-19 before vaccination, the infection had not been detected in them at the time they were vaccinated, but in the days immediately after. The Gibraltar Health Authority can confirm that there is no evidence at all of any causal link between these six deaths and the inoculation with the Pfizer vaccine.”
In Scotland, excess mortality rose sequentially in each age group as vaccination rolled out to them. For natural covid waves the relationship was reversed with the young being infected first before infections reached older groups.
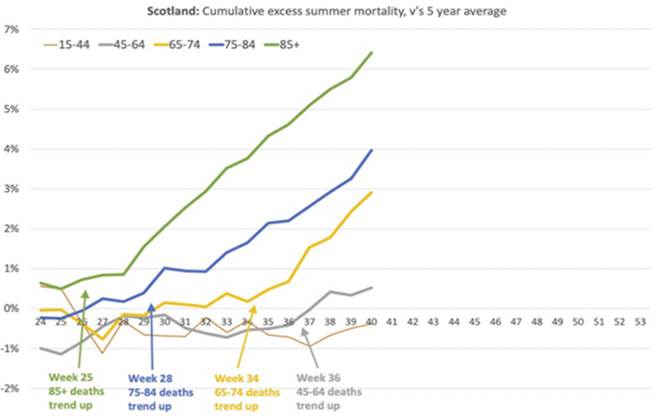
Figure 34: Scottish excess mortality by age showing upticks as vaccine rollout progressed to younger age groups
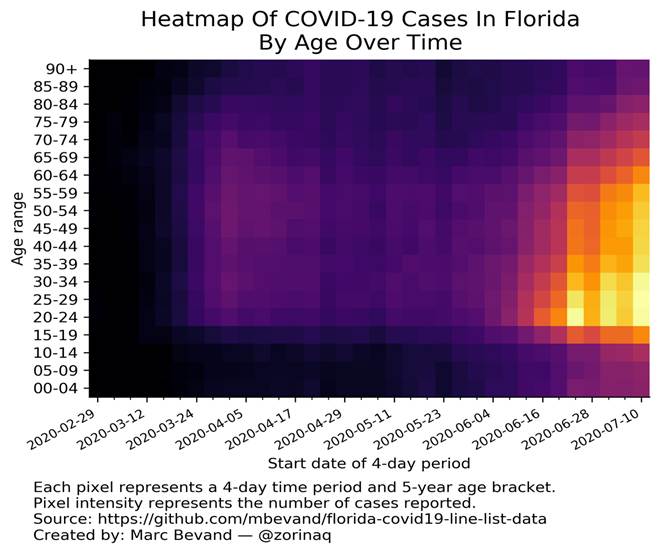
Figure 35: Heatmap showing age on the y-axis and time on the x-axis showing a covid outbreak in Florida spreading from young to old in summer 2020
As the vaccines were rolled out sequentially to children, each associated year group in the school population saw a spike which ended when rollout moved to younger pupils.
b. Impact in care homes
Government advice recommended vaccinating in care homes even during an outbreak. On 3rd Jan half of all covid outbreaks reported by PHE were in care homes which were being heavily vaccinated. 60% tested positive and over a third of the residents died at Pemberley House in Basingstoke shortly after vaccination. In contrast 6% of residents died in care homes studied by Public Health England in spring 2020. In Trecarrel Care Home in Cornwall, a quarter of the residents died shortly after vaccination. Castle Gardens care home had ten deaths after only 33 people tested positive. Relatives reported that the residents had been vaccinated prior to testing positive. Professor Boyd Robertson, chairman of NHS Highland said of another outbreak “it’s likely immunity had not had time to develop in those who’d been vaccinated.”
Multiple reports were filed in the US vaccine adverse event reporting system (“VAERS”) of elderly people who shortly after vaccination tested positive and died. In the USA, peak nursing home deaths from covid occurred in February 2021, with vaccine rollout, a full month after peak covid deaths in the community. It was admitted that only 10% of residents had been vaccinated by 10th January but by 8th February 2021 it was 93%. In that five week period there were 7,945 covid deaths of care home residents. For comparison there were 3,184 in the prior five weeks and 2,069 in the following five weeks. Some of that difference could be a seasonal effect but nevertheless the numbers were stark.
Irish care home deaths rocketed to record levels. Normally peak deaths would occur in early January. However, almost all the January deaths were seen after the vaccine was given in care homes even though they were not given until 24th January. This Irish data was not comprehensive but is nevertheless concerning. A study in 2021 showed that vaccination in Northern Irish care homes doubled the risk of being closed for an outbreak with a peak at day 28. There was little sign of protection with 44% of care homes in Northern Ireland having an outbreak in the four months from March 2020.
Public Health England reported that 10% of household contacts were infected by unvaccinated cases up to February 2021. At the time the rate was 12% for the population as a whole. It might be deduced that the vaccinated had a higher rate but they claimed it was only 6% if the first three weeks after injection were ignored. It turned out that care home residents were excluded from the study. Excluding the group who had had the most vaccines and were most at risk is misleading (putting the best light on it). Either care home residents or people within three weeks of vaccination (or both) were responsible for the much higher overall rates of spread.
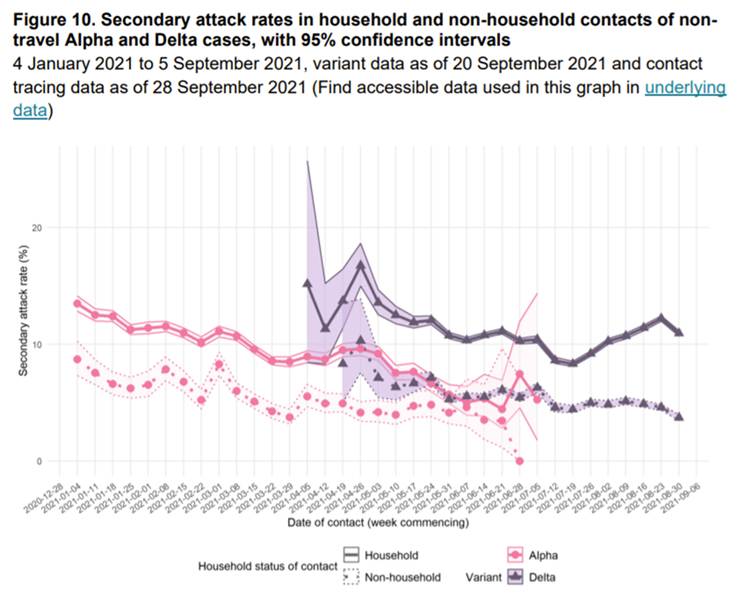
Figure 36: Real world transmission rates as measured by the proportion of contacts that become infected, the secondary attack rate.
c. Impact overall
Public Health England showed that the number of unvaccinated testing positive was very low as at week 4 and 5 of 2021. However, the vaccinated continued to have significant numbers of positive test results, such that the majority of cases were in the vaccinated. By mid-February only 25% of the population had been injected.
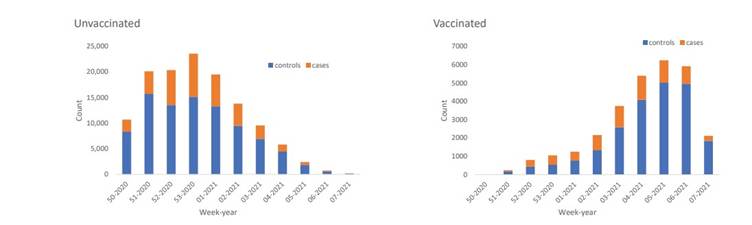
Figure 37: Weekly number of negative tests performed in England (controls in blue) and positive tests performed (cases in orange) in the unvaccinated and vaccinated. Note different sized y axis.
The hospitalisation and death rate in the first two weeks after injection was also disproportionately high. Data from Alberta shows the death rate was three times as high in this period. In those who were within 20 days of vaccination the covid mortality rate was higher than in the unvaccinated for every age group.
Table 2: Extract from Table 2 of report to SAGE comparing the percentage of who died within 20 days with the unvaccinated by vaccination priority group
Norway, which had at that point seen a total of 517 deaths with covid, reported 29 deaths of elderly people a short time after receiving the Pfizer-BioNTech vaccine. They altered their advice to say that the elderly should only be vaccinated at their doctor’s discretion.
d. Excuses for the problem
SAGE commented on the phenomenon in March 2021 saying,
“The observation that a significant number of people developing [sic] symptoms within a few days of a first dose may suggest some behaviour change following vaccination (and before immunity has developed). It is important therefore that communications around vaccination reinforce the need for safe behaviours to be maintained. It may also be the case that some infections occur during the end-to-end process of vaccination (i.e. including journeys to and from vaccination). The low number of people in the study with symptom onset in the days prior to vaccination is expected, as most people with symptoms would not attend their vaccination appointments. Many of those included in the study would have been vaccinated at a time when community prevalence was very high.”
The assumption that people with symptoms would not attend their vaccination was disproved by Public Health England (see figure 31) when they showed an increasing number with a positive test each day in the week leading up to vaccination.
In April 2021, SAGE proposed three possible reasons for the problem:
- Coincidence that can be ignored despite being above background rates: “Most vaccinated hospitalised patients were infected shortly before or around the time of vaccination.
- Natural exposure due to behavioural changes: “Elderly and vulnerable people who had been shielding, may have inadvertently been exposed and infected either through the end-to-end process of vaccination, or shortly after vaccination through behavioural changes where they wrongly assume they are immune.” Evidence showed people reduced their contacts with the elderly during the winter covid wave. Furthermore, PHE pointed out “the increase occurs within three days, before the typical incubation period,” so too soon for natural exposure at the time of vaccination.
- The admissions were for side effects of vaccination with incidental asymptomatic covid: “An additional hypothesis, that we cannot exclude in this analysis, is that some people had recent asymptomatic COVID-19 and vaccination precipitated admission. Previously asymptomatic…PCR positive patients may experience symptoms likened to COVID-19 symptoms including fever due to vaccination.” Why would such side effects require hospital admission?
Public Health England claimed, “During the first few days after vaccination (before an immune response would be anticipated), the odds of vaccinated people testing positive was higher, suggesting that vaccination was being targeted at those at higher risk of infection.” Their own data showed the elderly had the lowest infection risk. They even used the higher risk in the period immediately after vaccination as a baseline with which to claim vaccine efficacy in the subsequent weeks.
The lack of incubation period between vaccination and covid infection in these cases suggests it was not just an increase in exposure that caused the problem. Exposure coupled with a reduced immune response would explain this reduced incubation period. A care home outbreak included every genetic variant of covid present in the community because it is spread through the air. Nevertheless blame for the outbreaks was directed at human behaviour. The ONS hypothesised, “possible explanations for infections shortly after vaccination include exposure to COVID-19 at vaccination centres, change in behaviour following vaccination, or prompts to get vaccinated because of knowledge of individuals around them testing positive.”
Susan Michie, prominent member of the SAGE behavioural science group Spi-B and colleagues admitted in March 2021 in the BMJ that, “the odds of testing positive for SARS-CoV-2 appear to increase in the first week following vaccination, before protective effects have developed by about three weeks.” but still referenced the idea that “some people are letting down their guard.” The latter point relied on evidence from a survey which showed that people were meeting indoors after vaccination but provided no control data for the period before vaccination or in the unvaccinated.
Other data from the ONS showed that people had fewer contacts during the 2021 vaccine rollout with the elderly during the covid winter lockdown. The fact that there were still contacts is because frail elderly people often need help from relatives. An investigation was begun after an outbreak in Dukes Court Care home in Northamptonshire as to whether the vaccination team brought covid into the care home because of inadequate PPE. Two members of staff were charged after an outbreak in a Devon care home in which nine residents died.
The second dose only increased efficacy by 4 percent. However, medical leaders were acting as if the second dose would solve the problem. In February 2021, Professor Martin Vernon, a consultant geriatrician in Greater Manchester, said he was “deeply concerned” by infection outbreaks “within, and beyond 21 days of vaccination”. He described the decision to postpone second doses in care homes as “a mistake we may all live to regret” A letter from the BMA to Chris Whitty raised concerns that a first dose “does not produce sufficient neutralising antibodies and the potential to reduce transmission.
e. Denial of the Problem
As a consequence of people observing covid outbreaks and deaths following vaccination, the NHS stated that the vaccines “do not contain a live virus” and “you cannot catch COVID-19 from the vaccine but it is possible to have caught COVID-19 and not realise you have the symptoms until after your vaccination appointment.”
The statement that the vaccine itself did not contain the virus exposes a closed mindset about what might cause an association between vaccination and outbreaks. It has been well established that vaccination for other diseases results in a period of increased risk to other respiratory viruses. By the first week of February there were reports of outbreaks in double vaccinated care homes in Germany.
There seemed to be a total inability to even consider the possibility of a relationship between vaccination and the onset of covid infection. Public health authorities felt the need to state that “as there is no whole or live virus involved, these vaccines cannot cause disease.” The NHS stated: “You cannot catch COVID-19 from the vaccine but it is possible to have caught COVID-19 and not realise you have the symptoms until after your vaccination appointment.” This exposes the closed mindset about what might cause an association between vaccination and outbreaks.
It has been well established that vaccination for other diseases results in a period of increased susceptibility to infection. The vaccines were designed to cause the body to produce huge amounts of spike protein. The immune system then reacts by attacking and killing every cell producing this foreign protein and as such has less capacity to fight off infection in the usual way. Lymphocyte levels (the white blood cells involved in fighting off infections) fall in the first three days after Pfizer-BioNTech vaccination. The AstraZeneca trial showed a drop in neutrophils (a different type of white blood cell also involved in fighting infections) in 7 percent of the control group but 46 percent of the treated group.
The ability to prevent other viral infections was also hampered. An Israeli study of women under 61 years of age showed a rate of shingles infection fifty times higher than expected in the first two weeks after injection. The risk of Cytomegalovirus, Herpes Simplex virus and Epstein Barr virus infection also increased. These are DNA based viruses that become dormant in the body unlike SARS-CoV-2 but the principle that the immune system’s ability to keep infection at bay was hampered is demonstrated with these examples.
Government guidance repeatedly claimed, “Since inactivated vaccines cannot replicate, they cannot cause infection.” A product can cause infection without it being the source of that infection. Massively increasing the risk of infection is one way in which they can cause infection in those who are susceptible.
f. Creating an illusion of efficacy
The vaccine caused the 10% of the population who were susceptible to have their infections earlier than otherwise. By ignoring the first two weeks in every calculation a distorted view was enabled. After an infection, immunity is acquired and this was being misinterpreted as protection provided by the vaccine.
Two papers, one on healthcare workers and one on care home residents detailed outcomes for the entire wave, including the initial two weeks post-vaccination. Over the course of the full wave there was no benefit from vaccination in either paper. Vaccination had indeed just caused the cases in the susceptible to occur earlier. Two papers is too little evidence to be certain of this – but where were the other papers? Why did every other group of scientists exclude data for this period?
The overall effect of vaccination causing earlier cases can be seen when comparing covid mortality in the UK with the rest of Europe who rolled out vaccination more slowly (see figure 38). As covid was an infection, a rise in covid in the vaccinated due to immune suppression would lead to increased risk to the unvaccinated too. The area below the lines on the graph indicates how many deaths there were altogether and it is clear that the total was similar for UK and Europe, but the European deaths were just more spread out. The total deaths per million for both the UK and Europe over the whole period was similar:
Figure 38: covid deaths per million, UK / Europe
A further effect of this illusion was that the vaccine appeared to “work” at preventing infections from the variant circulating at the time of injection, however there was no protection from a new variant. A new variant would surge when a new ~10% of the population became susceptible. The lack of protection was described as “waning” when in fact it was the end of a statistical illusion. That is why the timing from vaccination to “waning” varied from 6 weeks to 6 months depending on the timing of the vaccine programme and the seasonal trigger for a new wave in different countries. If waning had been a biological phenomenon the timing would have been the same everywhere.
i. The ‘doubling’ effect of ignoring the first two weeks
Professor Martin Neil, professor of computer science and statistics, collated 25 studies where infections were wrongly classified (with respect to vaccination status) in the first two weeks after injection.
The result creates two biases. Not only is covid in the vaccinated in the first two weeks not included in the totals for the vaccinated, but it is added to the unvaccinated tally, distorting that result too.
ii. Recurring problem with further doses
After dose two the same phenomenon of extra infection in the first two weeks was observed. Figure 39 below shows the risk (odds ratio compared to the unvaccinated) was higher in the first few days after the second dose than at any time since a month after the first dose.
Table 3: Public Health England data on risk of testing positive by days after each dose compared to the unvaccinated
Public Health England again demonstrated that, although there were a consistent number of positive test results each day in the lead up to vaccination, there were two to four times as many positive test results each day in the period after vaccination with the second dose.
Figure 39: Number of negative tests done (in blue) and positive tests (in yellow) in period before and after vaccination with second dose of Pfizer/BioNTech product
In Scotland, the case rates peaked at a similar level in September 2021 regardless of vaccination status (~100 on the y-axis on figure 40). In December 2021, when boosters were rolled out, they peaked twice as high in the unvaccinated (~200), three times as high in the single dosed and triple dosed (~300) and four times as high in the double dosed (>400).The cases recorded within two weeks of booster doses were attributed to the two dose group who saw a peak that was twice as high as the unvaccinated peak.
Figure 40: Public Health Scotland data showing age adjusted covid positive test rates per 100,000 people by vaccination status
Similarly data from Iceland showed a higher case rate in the double vaccinated compared to the unvaccinated as infections in the recently boosted were misattributed.
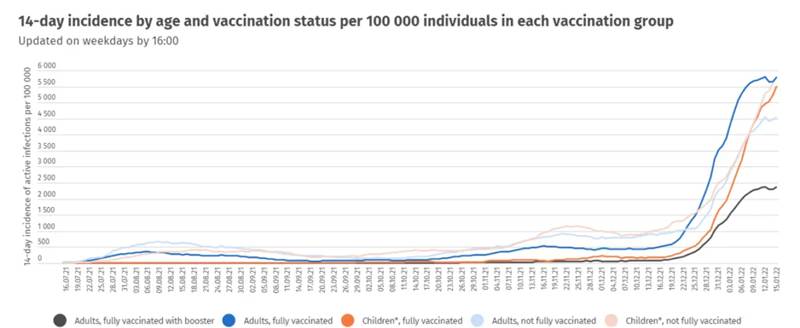
Figure 41: Icelandic government data on cases per 100,000 vaccinated or unvaccinated adults or children
The problem was most stark in Japan where each covid wave correlated almost exactly with vaccine distribution. From May 2023 both covid cases and deaths stopped coincident with them ceasing new vaccinations. The hypothesis of a link was confirmed when Japan and South Africa rolled out their vaccines much later on. Each Japanese wave of covid attributed deaths has closely tracked vaccination.
Figure 42: Vaccine doses given (pale line) superimposed on covid cases in Japan (dark line)
Note the rise or fall in cases every time there is a rise of fall in doses. There is a sharp fall at the beginning of January 2023 resulting in a dip in cases.
Figure 43: Covid attributed deaths (pale line) superimposed on covid cases in Japan (dark line)
Note the dip in cases in January 2023 also translated into a dip in subsequent deaths suggesting this was a real finding and not an artefact of less testing due to a public holiday etc.
It is clear there was a genuine problem with excess covid infections in the period immediately after vaccination. It is possible that this did indeed account for all the claims of subsequent benefit as these people had post infection protection thereafter. However, it is not possible to be certain about that conclusion based on the little data that is available and the effect may have only been to distort the data partially not completely.
7.4 False Claim: Vaccinations could defeat the virus and take us back to normality
A tweet from Pfizer said, “The ability to vaccinate at speed to gain herd immunity and stop transmission is our highest priority.” Professor Jonathan Van-Tam, Deputy Chief Medical Officer, said that once at-risk groups and those over 50 years old were vaccinated, “then we could in theory take out 99% of hospitalisations and deaths related to Covid 19.”
Only 10% were at risk of catching covid in each pre-omicron wave as evidenced by the household transmission rate and the smaller proportion of household contacts who caught covid and developed antibodies. The proportion who developed antibodies in each six months was 5-7%. These figures held true for the Delta wave indicating a similar proportion were susceptible as in the previous waves, showing the vaccines did not reduce infections.
If everyone was susceptible there would have been higher antibody levels in those who were at higher risk of exposure. Antibody studies showed that healthcare workers developed antibodies at the same rate as other members of society. Being 18-24 years old, living in the North West or London, or living in a household of 6 people had the same risk as being a patient facing healthcare worker by November 2020.
The original claim was that vaccination would lead to herd immunity and in the words of Boris Johnson “defeat this virus and get our lives back to normal.” Given that all the vaccines could do was create antibodies that circulate in the blood rather than ones that can protect the lining of the respiratory tract from infection, this was always a dubious claim. Injected measles vaccines work because the replication takes place in the lymph nodes but for SARS-CoV-2 replication happens in the airways. From July 2021 there was a series of outbreaks in heavily vaccinated populations indicating that this claim was patently false. The vaccinated still caught and spread covid.
7.5 False Claim: Vaccinations would prevent infection
In April 2021, the WHO said, “After vaccination, if the body is later exposed to those disease-causing germs, the body is immediately ready to destroy them, preventing illness.”
In section 7.2a “How could these novel products prevent infection?” above, I set out the reasons why in principle preventing infections with an injection could not work.
Before and after vaccination the same proportion of household contacts were susceptible ~10% for each wave. A similar proportion (5-7%) developed antibodies according to UKHSA. Therefore there was no protection afforded by vaccines (see table 4).
| Jan-Jun 2020: Wuhan | Jul-Dec 2020: Unnamed variant | Vaccine rollout begins | Jan-Jun 2021: Alpha | Jul-Dec 2021: Delta | |
| % of household contacts who caught covid from infected person | 11 | 9.9 | Vaccine rollout begins | 10.2 | 10.9 |
| % of blood donors who developed infection related antibodies | 5 | 5 | Vaccine rollout begins | 7 | 7 |
Table 4 Comparison of percentage of household contacts who became infected with proportion of blood donors who developed antibodies over six month periods in 2020 and 2021
A huge amount of emphasis was placed on the fact the Delta wave was flatter than the Alpha wave in the UK. This was not the case in other heavily vaccinated countries. It is more important to look at the impact of the whole wave than its intensity which could vary by region and time.
Exaggerated claims were made in terms of efficacy, particularly that the vaccines could prevent infection and hence transmission of the virus. This claim had never been tested in the trials. If the vaccines worked they should work in every location in clinical trials. One study in February 2021 showed AstraZeneca only provided a 20% reduction in risk of infection. If we are to believe that the vaccines were equally efficacious for every variant since then, why was this an exception?
AstraZeneca ran a phase 1 /2 trial in South Africa just at the beginning of the first South African covid wave. There were a total of 23 placebo “cases” and 19 vaccine “cases” with no severe cases and no hospitalisations. This vaccine failure was blamed entirely on the Beta variant circulating in South Africa at the time. If the South African cohort had been included in the efficacy analysis that led to temporary authorisation the vaccine efficacy would have been 51% – only 1% above the WHO baseline for approval of vaccines.
AstraZeneca carried out a second phase 3 trial. They claimed “The estimated vaccine efficacy for incidence of first SARS-CoV-2 RT-PCR–positive symptomatic illness occurring post first dose of trial intervention among participants in the full analysis set who were SARS-CoV-2 seronegative at baseline was 54.5%” (287 cases vs 303 but in a placebo group that was half the size). Two of the three trial sites, Peru and Chile did not see any statistically significant benefit.
The first sign that all might not be as was being portrayed was reported in May 2020 when a trial in Rhesus monkeys did not reduce infection rates or the amount of virus produced. This was ignored and human trials went on.
A study of the vaccinated and unvaccinated care home population showed a similar proportion testing positive except for the period immediately after injection when the risk was higher among the vaccinated particularly after the second dose.
Table 5: Percentage of nursing home residents testing positive in different periods after vaccination carried out in homes comparing vaccinated and unvaccinated residents
The survivorship bias from infections being brought earlier could not impact on the Delta wave. In July 2021 it was clear that any illusion of benefit at preventing cases had gone:
- Singapore had vaccinated only 60% of their population yet 75% of cases were in the vaccinated. The health ministry was reported as saying none of the eight severe cases “had been fully vaccinated” without defining that.
- The CDC reported that three quarters of people infected in an outbreak in Cape Cod were vaccinated and that the vaccinated produced the same amount of virus when infected.
- A 100 percent vaccination rate on HMS Queen Elizabeth did not prevent an outbreak which affected just over one in five people in just over two months.
- In Israel an outbreak in a hospital reported that only 3 out of 42 of the cases were unvaccinated. The Israeli Ministry of Health said the Pfizer vaccine was only 39% effective against Delta.
- Sajid Javid, said the double vaccinated UK health secretary, tested positive.
In September 2021,
- Sajid Javid was still saying people should be vaccinated to “protect yourself and your loved ones.” Duke University reported positive cases in 349 students and 15 members of staff. Of all these cases only 8 were said to be unvaccinated.
- Harvard business school moved to teaching online because of a covid outbreak despite having vaccinated 95 percent of students and 96 percent of staff.
- A paper was published online titled “Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States.” The authors looked at cases in a two week window and compared to vaccination uptake. The relationship was the wrong way round. The more vaccinated places had higher case rates. This could be because of a bias because richer countries test more and vaccinate more but the US comparison is fairer on that count. Four of the five most vaccinated counties were identified by the CDC as “high transmission counties” and a quarter of “low transmission counties” had vaccinated fewer than 20 percent of the population.
in October 2021,
- While mandating vaccination for care home workers, the British Prime Minister said, “It doesn’t protect you from catching the disease and doesn’t protect you against passing it on.”
Public Health England took the number of cases in the vaccinated and assumed that 95% of the cases had been prevented as should have resulted from the accepted claims. This resulted in a ludicrous claim that a total of 23.4 million cases had been prevented by August 2021 in England alone. That amounts to claiming that in the absence of vaccination half the population would have been infected within just a few months despite only 11 percent of household contacts being susceptible. Assuming the vaccines worked as claimed is not tenable as a hypothesis.
a. Number needed to vaccinate to prevent an infection
From a patient’s perspective the most useful measure for them to decide on benefit is the “number needed to vaccinate.” If the whole period after vaccination was included that number would be infinite. However, even based on the claims in the trial the number is higher than most people were led to believe. For Pfizer/BioNTech, after 6 months follow up 3.9% of the placebo group had been recorded as a case (more than 7 days after second dose) compared to 0.4% of the vaccine group.
That means 28 people would need to be injected in order to prevent one case over a 6 month period. A rate of 1 person protected per 28 people is a 3.5% chance that any one person will prevent an infection by being injected. Yet, the pharmaceutical companies were allowed to present this as a 90% risk reduction (because 0.4% is only a tenth of 3.9%). Both sets of figures are entirely dependent on the survivorship bias where the protection was actually afforded by natural immunity after infection.
b. Using the wrong denominator
The total hospitalisations with covid were always going to be higher in the vaccinated because the population at risk from covid were almost all vaccinated. The meaningful measure is therefore the hospitalisations as a fraction of the population.
While measuring the size of the vaccinated population is fairly accurate assuming decent recording of vaccinations, the same cannot be said for measuring the size of the unvaccinated population. Estimates of the size of the whole population vary greatly leading to even greater differences in estimates of the unvaccinated population.
Estimates for England included the low ONS estimate and the PHE / UKHSA estimate for the NHS records (NIMS – the National Immunisation Management System) which was higher.
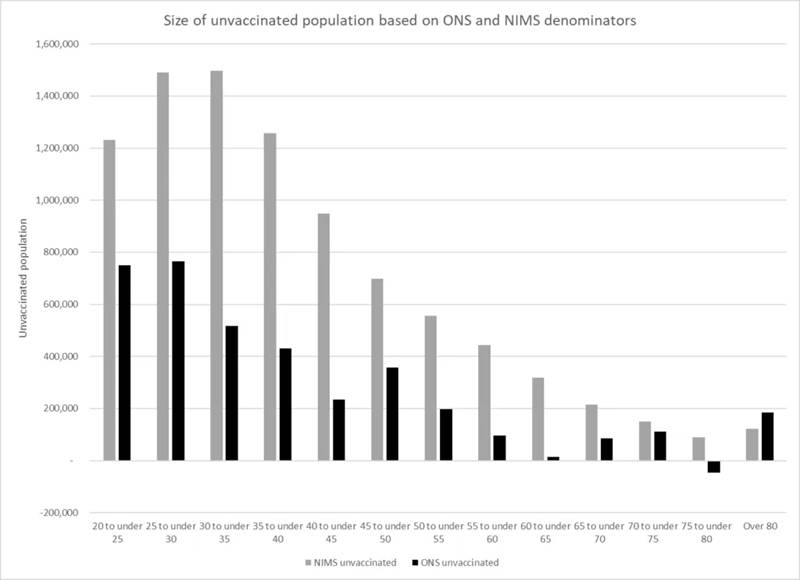
Figure 44: Estimates of size of unvaccinated population in January 2022 bases on ONS and NIMS population estimates
The ONS failed to include numerous people in their 2011 census count leading to complaints from local councils. Since that time they estimate that there was more population growth between 2001 and 2011 than between 2011 and 2021.
Even the NIMS estimate was an underestimate for the size of the population. In fact, so many people were first registered in the NIMS system when they were vaccinated that for certain age groups in multiple regions there were more people who were vaccinated than the ONS claimed existed.
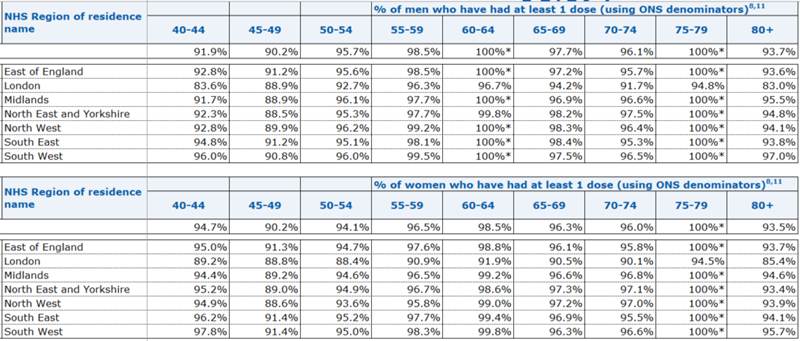
Table 6: NHS England calculations of vaccination rates using ONS denominators
Three alternative methods were proposed to estimate population sizes for assessing vaccine effectiveness each offer unique approaches.
- Estimating the Uncounted Population: This method uses data on COVID-19 test results from individuals not registered in the NIMS system (“unlinked” cases). By assuming these unlinked cases represent the unvaccinated population not counted in NIMS, the population estimate can be scaled up appropriately.
- Population Growth Estimation: This approach uses the average annual population growth rate (2.9% per year) observed in the NIMS dataset since 2011 as people are given NHS numbers. The total population is estimated based on the 2011 census estimate and this growth rate.
- Death Ratios Method: By comparing the total deaths in vaccinated and unvaccinated groups, it estimates the proportion of unvaccinated deaths. This data is then used to infer the size of the total population based on the number of vaccinated individuals.
Remarkably, despite their different methodologies, all three approaches yield similar results, suggesting a larger population size than estimated by traditional methods like ONS and NIMS, and thus, potentially accounting for the perceived differences in case, hospitalisation and death rates in the vaccinated and unvaccinated populations.
Places like Scotland (see figure 40 in section 7.3f), Ontario and Iceland (see figure 41 in section 7.3f) were reporting higher case rates in the vaccinated in early 2022. However, New York City, where it is harder to be accurate with population estimates, stood in stark contrast.New York City claimed 500 hospitalisations per 100,000 unvaccinated people in January 2022, with Omicron, whereas it had only been 112 per 100,000 at the peak in April 2020. The calculation was due to massively underestimating the size of the unvaccinated population. In the meantime, the deaths per hospitalisation was 8.9% in the vaccinated and 9.2% in the unvaccinated.
A BBC survey was commissioned in spring 2022 asking a representative sample of the population whether they were vaccinated. Over a quarter of respondents (26%) said they were unvaccinated. Taken together with the total number recorded as being vaccinated that would imply there were 2.2 million more unvaccinated adults than the NIMS estimate and case, hospitalisation and death rates were overestimated by 17%.
By 10th January 2022, Albert Bourla, CEO of Pfizer said, “we know that the two doses of the vaccine offer very limited protection, if any.” There were additional doses for sale at this point.
7.6 False Claim: Vaccinations would protect those around them
NHS adverts said “The Covid vaccine is the best way to protect yourself, friends and family from the virus.” As late as January 2023, at least eighteen months after the evidence was clear that infections were not prevented, Dr Mike Ryan, head of the WHO covid team said, “Vaccination is about protecting yourself, but it’s also an inherently altruistic act — you’re vaccinating yourself in order to be part of an immune group that will then protect those who can’t be vaccinated”
When a vaccinated person was infected there were claims that they would be less infectious to others. This could theoretically happen in two ways:
- producing less virus in an infection
- being ill for fewer days
The ONS carried out random sampling of the population by PCR before and after vaccination. If vaccination reduced the virus produced in an infection there would have been a lower proportion of strong positives after vaccination than before. In reality, the proportion of strong positives remained the same.
By July 2021, SAGE reported on this finding saying,“ONS data suggest that for those who have been vaccinated who do get infected with the delta variant, PCR cycle threshold (Ct) values are generally lower [meaning a stronger test result] than for those infected with alpha, suggesting that vaccinated people may still have a high viral load with delta infection (medium confidence). This may mean that there is limited vaccine effect against onward transmission for the delta variant.”
In March 2021, data from Israel showed slightly weaker positive test results in the vaccinated assumed to be because of less virus being present. By August 2021, Fauci admitted that the amount of virus in the infected was the same whether or not the person was vaccinated. He blamed it on the Delta variant. By August 2021, it was clear that from February 2021 until June 2021 (prior to Delta) the amount of virus from symptomatic infections in the vaccinated and unvaccinated was the same. A study from Wisconsin of tests done between June 2021 and December 2021 showed no difference in infectiousness between the vaccinated and unvaccinated.
The only other potential benefit regarding infection and transmission to others would be a reduction in the duration of infection. A UK symptom tracking research study called the ZoeApp reported the median duration of infection in the Delta wave to be 8 days compared to 5 days for Omicron in the vaccinated, but said they couldn’t show the results for the unvaccinated because they had too few in their sample. For comparison the duration for Wuhan, according to the CDC, was reported as 8 days in 2020. So there was no reduction in duration of symptoms. If there were a reduction in transmission then fewer household contacts would develop infections if the infected person was vaccinated compared to if they were unvaccinated. When this was measured there was no difference.
President of International Developed Markets at Pfizer, Janine Small said, at an EU parliament meeting when asked “Was the Pfizer covid vaccine tested on stopping the transmission of the vaccine before it entered the market?” She replied, “No… we had to really move at the speed of science to what was taking place in the market” and from that point of view we had to do everything at risk.” All that would have been needed to test transmission was to measure antibody levels in the household contacts of the handful of trial participants who caught covid. This was not done.
7.7 False Claim: They had a realistic chance of personal benefit from the injections in terms of a reduced risk from covid
In a hypothetical situation where vaccination did reduce the risk of hospitalisation and death then not everyone could have benefited. There were huge age-related effects, for example there were only 1035 deaths in hospital “attributed to covid” (which will include “deaths with”) by end-2021 in healthy under 60s in England. This is ~1% of all “covid deaths” in the whole population and incidentally it was <1% of deaths of any cause in under 60 year olds.
The JCVI admitted this was an issue when they did not recommend vaccinating 12-15 year olds saying, “The margin of benefit, based primarily on a health perspective, is considered too small to support advice on a universal programme of vaccination of otherwise healthy 12 to 15-year-old children at this time.”
If the overall mortality risk had been as high as claimed at the outset (they said 0.9% of the population who caught it would die) then the risk by age would be as presented in table 7 below. The infection fatality rates by age in the table below were calculated by Cambridge University’s biostatistics department. The risk presented in the table, when extrapolated to the whole population would work out at a 1% mortality risk from covid which is now known to be far too high. These risks therefore represent what the claimed threat was in March 2020 not the actual threat. Furthermore, these numbers don’t separate the healthy from non-healthy, and since nearly all deaths are in the latter, the actual risks for the former (especially in the non-elderly) are actually much lower.
If your risk of dying when you catch covid is only 1 in 4000 and only 10% are susceptible in any one wave, then your risk of dying during the few months of claimed vaccine efficacy would be 1 in 40,000. For a vaccine that was 100% effective, 40,000 people would have to be exposed to the drug in order to prevent one death. In all likelihood the 39,999 people needlessly exposed would have been from the healthier proportion of the population whose risk was lower still. The younger you become the more extreme the number of people who would need to be exposed in order for one to benefit.
The Omicron variant presented a lower death risk for both ‘vaccinated’ and ‘unvaccinated’ populations evident from its first wave in South Africa, despite having low ‘vaccination’ rates. The first wave of Omicron resulted in lower death rates than typical for winter in Europe and USA. The number of injections needed to cause harm is considerably higher than that as we shall see.
| Chance of dying if you catch covid | Same risk as… | |
| < 5 YRS | 1 in 270,000 | Dying this year from a fire |
| 5 TO 14 YR OLDS | 1 in 77,000 | Dying from a general anaesthetic |
| 15 TO 24 YR OLDS | 1 in 29,000 | A clover is three times more likely to have four leaves and an oyster to have a pearl. |
| 25 TO 44 YR OLDS | 1 in 4,000 | Four times less likely than the chance of finding a double yolk when you crack open an egg. |
| 45 TO 64 YR OLDS | 1 in 560 to 1 in 280 (at peak deaths) | Picking two aces in a row from a pack. During peak death, it was as likely as drawing four cards in a row from a pack and them all being Kings, Queens or Jacks. |
| 65 TO 74 YR OLDS | 1 in 120 to 1 in 43 (at peak deaths) | In summer, you would have been more likely to win after placing money on the horse with the worst odds in the grand national than to die if you caught covid. However, in December 2021 it was more likely but still only as likely as placing your money on zero in roulette and winning. |
| 75 YR OLDS AND OVER | 1 in 29 to 1 in 5 (at peak deaths) | In summer, the risk was of flipping a coin 5 times and it coming up heads every time. At peak deaths four in five survive. |
Table 7: Risk of dying with covid based on Infection Fatality Rates from the Medical Research Council’s Biostatistics Unit at Cambridge University
7.8 False Claim: Covid vaccination would reduce the risk of hospitalisation
SAGE showed in April 2021 that “mortality appears to remain high for people in high risk vaccination tiers who are admitted to hospital with symptomatic SARS-CoV-2 infection (COVID-19) despite vaccination 21 days or more previously.”
Based on the JCVI’s previous estimates of the hospitalisations to be prevented by the Vaccine, and the government’s published data on vaccine uptake for 12- to 17-year-olds, some 225 hospitalisations should have been prevented after administration of the Vaccine to that age group. Instead, Co-CIN shows that, for the 7-month period after vaccination of 12- to 17-year-olds began, hospitalisations in this age group with a Covid 19 diagnosis has increased (rising from 725 cases for the 7-month period ending 30 April 2021 to 832 cases in the 7-month period ending 31 December 2021). This amounts to a 15% increase in hospitalisations at a time when they only increased by 7% or less for younger age groups who had only had minimal vaccination. Over the same time frame the numbers needing ventilation fell in all younger age groups but increased for 12-15 year olds.
Figure 45: Hospitalisations in children before and during the period in which teenagers were vaccinated
| Jan-Jun 2020: Wuhan | Jul-Dec 2020: Unnamed variant | Vaccine rollout begins | Jan-Jun 2021: Alpha | Jul-Dec 2021: Delta | |
| % of household contacts who caught covid from infected person | 11 | 9.9 | 10.2 | 10.9 | |
| % of blood donors who developed infection related antibodies | 5 | 5 | 7 | 7 | |
| Covid labelled hospital admissions | 108,189 | 118,170 | 178,037 | 140,072 | |
| Covid intensive care admissions | 10,641 | 11,702 | 15,315 | 13,258 | |
| Covid labelled deaths | 48,628 | 32,276 | 52,494 | 17,823 | |
| Number of deaths in England above 2015-2019 average | 52,298 | 19,379 | 22,872 | 29,634 |
Table 8: Impact of vaccination in pre-Omicron era. Six month periods compared for impact on various measures.
Table 3 shows what happened in 2020-2021 before Omicron arrived. The proportion of people susceptible and the number acquiring antibodies at the end of the wave indicate that each wave affected a similar number of people before and after vaccination. Hospitalisations and intensive care admissions were higher in the post vaccination period prior to the arrival of Omicron in 2022.
a. Intensive Care admissions
Covid intensive care patients included patients who would otherwise have needed intensive care for other causes. Elective admissions to ICU were reduced during covid waves, but even allowing for that, the covid admissions clearly replaced admissions that would have occurred otherwise as only a minority of covid admissions exceeded the number of expected admissions. Since vaccination roll-out, total intensive care occupancy has remained well above expected levels despite far fewer labelled as covid admissions.
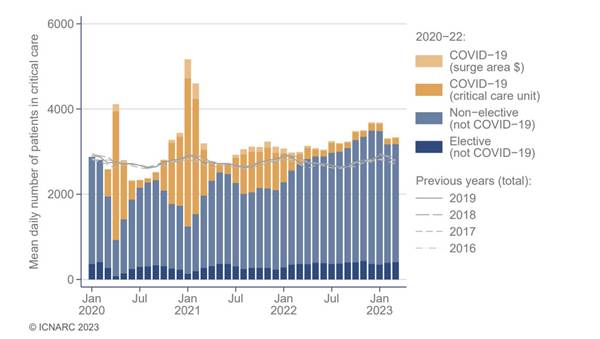
Figure 46: Average daily number of patients in intensive care by month and admission reason from 2020 onwards compared with levels in 2016-2019
b. Hospitalisations for other causes
The overall picture for hospitalisations was similar with capacity levels only exceeded after vaccination.
Studies showed that the vaccinated were hospitalised for all causes at a higher rate than the unvaccinated. The total NHS capacity available in January 2021 was exceeded from November 2021 and remained this high subsequently.
Figure 47: NHS England hospital bed occupancy by diagnosis (Pale blue = non-covid, lime green = covid, dark green = available beds and dark blue = incidental covid diagnosis). Dotted red line shows total NHS bed capacity in England in January 2021.
Public Health England data confirmed that the risk of hospitalisation for non-covid causes was higher in the vaccinated.
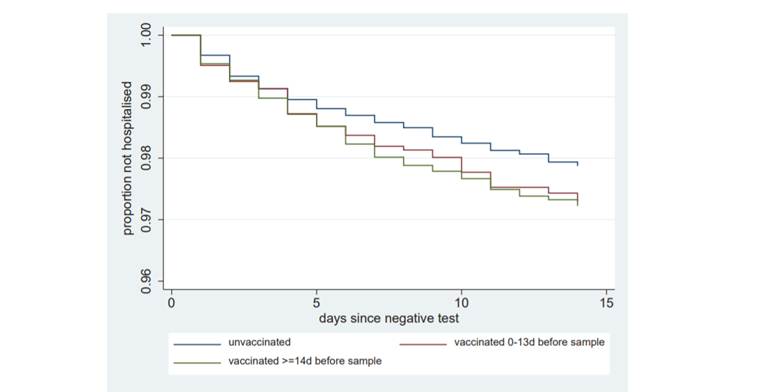
Figure 48: Public Health England study showing the risk of being hospitalised for a non-covid cause. The cohort starts with 100% not being hospitalised and with each hospitalisation the curve falls and it falls further in the vaccinated population. By two weeks, 1 in 200 more vaccinated participants had been hospitalised for a non-covid cause.
7.9 False Claim: Covid vaccination would reduce the risk of death
a. Trial Results
The claim made by AstraZeneca in a press release on 3rd February 2021, and repeated all over the media, that their product provided 100% protection against severe covid and death was based on there having been two hospitalisations for severe covid and a single death in the placebo group and none in the vaccine group.
Pfizer/BioNTech reported in their 6 month follow up paper that the number of deaths from any cause was higher in the group given a ‘vaccine’, which had 15 deaths, compared to 14 in the placebo group. Of these deaths there was only one covid pneumonia death which occurred in the ‘vaccine’ group. Two deaths in the placebo arm were attributed to covid in the absence of pneumonia. At best, therefore, injection of nearly 22,000 people prevented one death over the course of several months. The trial was global and ran from July to November 2020 including places in the Southern hemisphere, Brazil, Argentina and South Africa which had significant covid at the time and also including the autumn waves in the northern hemisphere. Therefore, the real world ability of injection to prevent covid deaths can be seen for the very low impact it could have.
A Pfizer submission to the FDA on 18th May 2021 reported 3 sudden, unexplained deaths in each group in the first two months, however, after two months there were five in the vaccine group and only one in the placebo group.
The overall mortality reported in this submission was 20 in the vaccine group, 16 in the placebo group and a further two in placebo participants who had been unblinded and injected with the vaccine. The four extra sudden, unexplained deaths therefore had an impact on the total overall mortality. The whole purpose of placebo controlled trials is to allow this type of direct comparison to be made. There is a concerning sign here that the ‘vaccines’ not only failed to prevent death but may have introduced an increased risk of death from other causes.
b. Real World results
There were fewer deaths attributed to covid in the Delta wave than in previous covid waves but there were still significant excess deaths (see table 3 above).
As with case rates and hospitalisation rates the comparison of death rates in the vaccinated and unvaccinated were distorted by use of too small a denominator for the unvaccinated population. The bias was clear to see in many studies as non-covid fatalities were also apparently reduced by the vaccine. When adjusting for the bias in non-covid deaths the claimed effect on covid deaths vanished. Such a bias was clear in the ONS death by vaccination status data.
The USA experienced a similar wave of hospitalisations with Delta, after vaccination, as its previous two waves. The fall came not with vaccination but with the arrival of Omicron.
Figure 49 a and b: Hospitalised patients (top graph) and intensive care patients (bottom graph) in the USA showing similar sized peaks before and after vaccine rollout prior to Omicron.
For Europe as a whole and for the USA, the death waves were also similar after vaccination to the previous waves and only fell with the arrival of Omicron.
Figure 50: Covid attributed deaths in USA and Europe per million people showing similar waves before and after vaccination in 2020 and 2021 prior to Omicron in 2022.
If lives were saved then why were the death curves in the USA and Europe of the same magnitude before and after vaccination? (see figure 50 above)
The ultimate test of whether vaccination worked was to compare countries and regions.
Israel and Palestine have very different demographics and healthcare but have similar environmental factors. Covid deaths tracked before vaccination and did not deviate after Israel’s extensive vaccination campaign. Covid ended in Palestine with Omicron from the beginning of 2022.
Figure 51: Covid attributed deaths in Israel and Palestine – vaccine rollout began in Israel in December 2020 and Omicron arrived in January 2022.
Similarly, Bosnia and Croatia are geographically intimate but politically distinct. Bosnia saw more covid death per million but a similar total number to Croatia before vaccination and the two have not deviated despite markedly different vaccination campaigns. Covid ended in Bosnia with Omicron in 2022.
Figure 52: Covid attributed deaths in heavily vaccinated Croatia and neighbouring low vaccination rate Bosnia – vaccine rollout began in Croatia in January 2021 and Omicron arrived in January 2022
Figure 53: All-cause mortality, Croatia and Bosnia
Similarly, within Europe, EU countries were more heavily vaccinated than Europe as a whole and no deviation was seen in death rates before and after vaccination.
Figure 54: Covid attributed deaths in heavily vaccinated EU countries and Europe which includes neighbouring low vaccination countries
Since 2022 there has been a strong correlation between high vaccination rates and mortality across Europe.
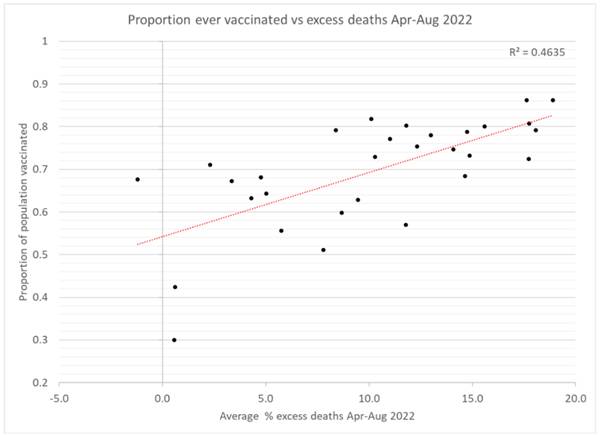
Figure 55: Correlation proportion of the population vaccinated and the percentage of excess deaths in spring and summer 2022 where each dot represents a country
This was a reversal of the relationship seen in the second half of 2021 with the Delta wave.
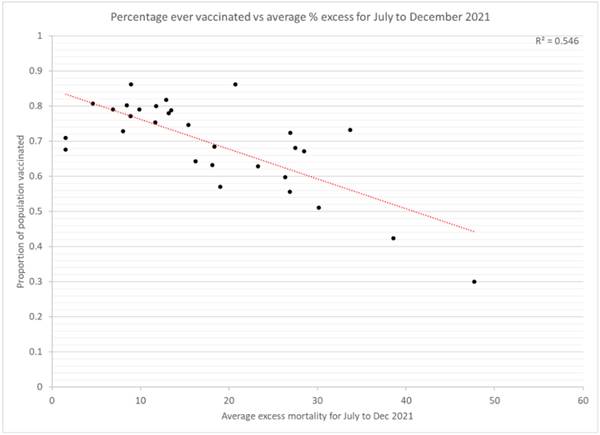
Figure 56: Correlation proportion of the population vaccinated and the percentage of excess deaths in second half of 2021 where each dot represents a country
These correlations can be deceptive and it was shown that the apparent lower excess mortality in more vaccinated areas of the United States was apparent prior to the vaccine rollout. The 2021 correlation in Europe may also all be due to other differences between countries. Several studies have shown higher mortality in more vaccinated regions including Netherlands, Germany, and the whole world.
We can further show this by looking at mortality in the first wave in places that did not have significant covid before Omicron. New Zealand reached 400 per million by October 2022 with Australia and South Korea seeing a similar rise once the 100 per million seen prior to 2022 are subtracted. That was the same order as Europe as a whole saw in the first wave despite extensive ‘vaccination’ and a less lethal variant. It was half the deaths seen in the UK in 2020, but then Omicron is only half as lethal. Where is the claimed benefit?
Figure 57: Cumulative covid deaths per million in Australia, South Korea and New Zealand in first 10 months of 2022
Figure 58: Cumulative covid deaths per million in UK, France and Europe as a whole in first 10 months of 2020
A smaller case study is the Amish community who had similar excess mortality to their states in 2020 but a third less than their vaccinated neighbours in 2021.
Almost every western country has seen excess mortality in the years after vaccine rollout despite the fact that high mortality in 2020 and early 2021 should have led to a deficit in deaths. For deaths of old age, like Alzheimer’s and Dementia, there is the expected deficit. However, there is a marked excess in deaths from cardiovascular causes. The problem is the worst in percentage terms in the younger age groups. It has not been definitively shown that these were vaccine induced deaths, however, there are indicators that this is the case.
Countries like Australia saw virtually no covid prior to vaccination and yet still had excess deaths starting in early 2021. South Australia had only 1000 cases across the whole state by December 2021 yet had a significant 67% spike in emergency cardiovascular admissions in 15-44 year olds, peaking in November 2021 before their first noticeable covid wave.
The following figure starkly illustrates the extent of the excess deaths in the UK which, if anything, are only increasing over time:
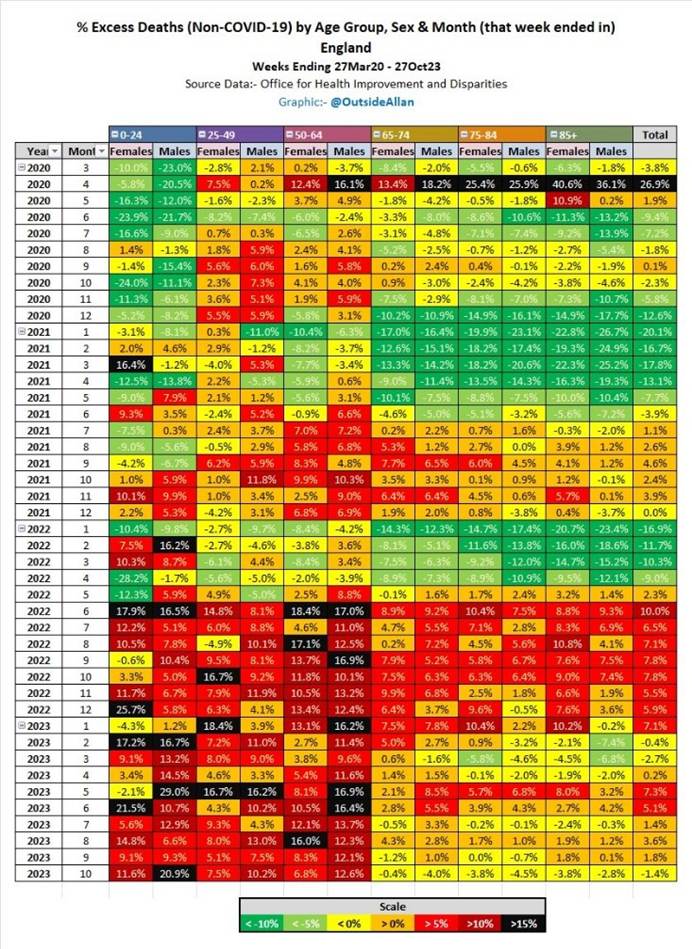
Table 9: Heatmap showing time in rows and different sex and age groups in columns demonstrating the degree of excess non-covid mortality over time
The Pfizer trial claimed there were 95% fewer symptomatic covid cases in the placebo group than the vaccine group more than two weeks after the second dose was given. That does not mean 95% of those injected could not catch covid. Looking at it another way, the same data showed that only 0.74% of the placebo group (162/21,728) had symptoms and tested positive compared to 0.04% of the vaccine group (8/21,720). That means only 0.71% of the vaccine group benefited during the two month follow-up a week after the second dose. For that period, 141 people needed to be vaccinated to prevent a single person from being symptomatic with a positive test result (21,720/(162-8)). These were almost all mild cases. Only a tiny fraction of those would be at risk of hospitalisation or death.
When this became self-evident the official line changed from ‘the covid vaccines prevent infection’ to saying they prevented hospitalisations and deaths. The placebo and the vaccine groups in the Pfizer/BioNTech trial each had three hospitalisations for covid-like illness. The claim was the trial prevented one death due to covid after injecting 22,000 people. There was huge bias in the reporting of deaths in the placebo group. By May 2021, there were fewer deaths among the placebo group and yet a third of the deaths had been described as covid deaths.
Based on the deaths per capita in the vaccinated and unvaccinated populations it is possible to calculate the number that needed to be vaccinated to prevent one death. HART did this calculation in September 2020 over the course of the Delta and early Omicron period before data was no longer published.
Table 10: Covid deaths prevented and number needed to vaccinate to prevent a covid death based on covid death rates from UKHSA data.
Even for the over 80-year-old group more than 200 needed to be injected for a single death to be prevented. For younger age groups the figures reached tens of thousands or more. UKHSA had not carried out this calculation in public but did so in October 2023 and their calculations concurred with ours.
A simple way of measuring potential benefit is to calculate how many would need to be vaccinated to prevent one death. This was calculated using UKHSA data for the whole Delta wave and most of the first Omicron wave. The data itself is not perfect as inaccuracies in estimating the size of the unvaccinated population can lead to large errors in the death rates for the unvaccinated. There are good reasons to believe that ONS and UKHSA underestimate the size of the population which would overestimate death rates in the unvaccinated making the vaccine look more effective. Using this biased data gives a number who needed to be vaccinated to prevent a single death during the Delta and most of the first Omicron wave. The number by age is given in the table.
Table 11: Table of Covid attributed deaths prevented and number needed to vaccinate to prevent a covid death based on covid death rates from UKHSA data
UKHSA carried out a calculation based on preventing a single hospitalisation over the course of a year. Their figures were based on July 2022 data. Their figures for preventing a serious hospitalisation (requiring oxygen or intensive care) are shown below.
Tables 13 a and b are UKHSA estimates of number needed to vaccinate with top table showing number to prevent any covid hospitalisation and the bottom table severe hospitalisations
The case for prevention of infection in the real world was largely based on modelled data. There were a number of ways in which such data was misrepresented. The timing of the measurements was one way.
Vaccination is a process that takes time. At the beginning of the study all participants are enrolled as unvaccinated. People move into the vaccinated cohort over time. The result is that the unvaccinated are exposed at periods of higher prevalence and for a longer time. The vaccinated are only exposed from a period later on and further down the curve. The vaccinated will therefore be less likely to catch covid and the vaccine can be made to look like it worked.
The ONS recently deployed this trick to claim a 32 fold lower mortality among the vaccinated. It was extreme data manipulation whereby they included the majority of deaths in winter prior to vaccination instead of starting from spring when a fairer comparison could have been made. The Office for Statistics Regulation has upheld a complaint about the ONS’s manipulation of data in this case.
7.10 Misleading Claim: There were fewer deaths per case after vaccination
This claim appears on the surface to be true. However, there is more than one way in which that could result. For example, the illusion of extra ‘cases’ in the presence of the same number of deaths would give the same result.
Omicron was a vaccine escape variant meaning that it evolved to avoid the narrow immune reaction induced by the vaccine. Consequently, a higher proportion of the vaccinated were infected than the unvaccinated. High case rate data resulted. When cases are increased the death per case can appear low even when the total number of deaths have not changed.
Pharmacist Walgreens in the USA continued to publish data showing the unvaccinated had the lowest positivity rate in December 2022.
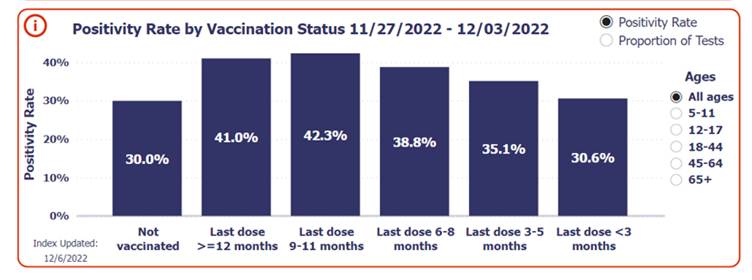
Figure 59: Percentage of tests returning positive by vaccination status from Walgreens in USA
Omicron infections were considerably milder than earlier covid infections, which explains much of the fall in the burden of infection.
However, it should be noted that a large study at the Cleveland Clinic clearly demonstrated that more injections lead to more – not fewer– infections, which would reduce any benefit in terms of covid outcomes overall, possibly to the extent of net covid-related harm depending on the magnitude of the effect.
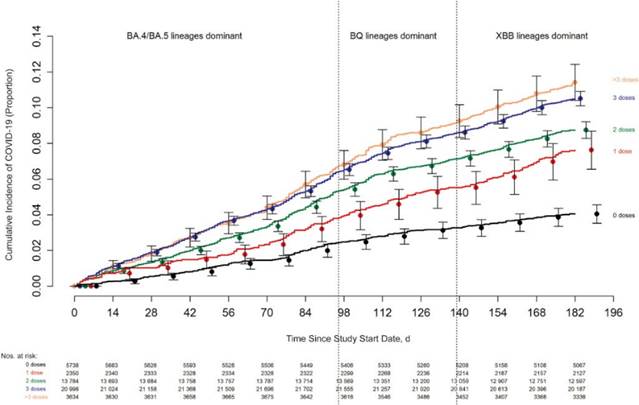
Figure 60: Cumulative cases by number of doses of vaccine given over time
The same group went on to show that this difference was not due to differences in testing rates or rates of previous infection.
Increased numbers of cases alone would give the impression of fewer deaths per case and were seen on a country level too. While deaths were similar in Palestine and Israel and in Croatia and Bosnia the cases rocketed with Omicron in the more vaccinated countries.
Figure 61: Cumulative covid positive test results in high vaccination rate Israel vs low vaccination rate Palestine
Figure 62: Cumulative covid positive test results in high vaccination rate Croatia vs low vaccination rate Bosnia
Figure 63: Cumulative covid positive test results in high vaccination rate EU vs Europe which includes lower vaccination rate Eastern European countries showing deviation with arrival of Omicron
There is in fact no data supporting the contention that vaccines prevented infection from Omicron – because they in fact did the opposite.
7.11 False Claim: 20 million lives were saved
Some people have accepted that there were harms from these novel products but then justify it in their minds saying they saved millions of lives. The evidence does not support that position.
The claims are based on fantasy modelling carried out by Imperial College which had significant coverage in the mainstream media. It supposes there would have been a huge increase in covid deaths in the absence of injections.
In reality, the global cumulative deaths (shown in graph below) increased at a steady trajectory until Omicron arrived. The less deadly Omicron caused the rate of accumulation of death to slow in a way that ‘vaccines’ had failed to.
Figure 64: Cumulative global covid attributed deaths (in black) compared to modelled estimate of what would have happened without ‘vaccines’
To reach the 20 million lives saved figure, half a million lives would need to have been saved in the UK alone. Even the most pessimistic initial claims predicted only half a million lives were at risk and there have been covid death since then which could not be prevented by vaccine.
There are a multitude of ways to show this claim was false. If you add the 500,000 lives saved claim to the 200,000 lives lost claim then that would mean more than 1% of the population would be dead even though around a third of the population are yet to have their first infection.
The MHRA itself claimed that only tens of thousands of lives were saved, and ONS and NHS have reduced this estimate further to only thousands being saved.
8. VACCINE HARMS
| Basic safety testing to understand this novel platform is still ongoing and even large well designed and executed trials will not be large enough to prove safety. Many of the proposed mechanisms of harm would explain damage to multiple organ systems. Dismissing the reported harm simply because they are diverse is therefore illogical. Although measuring harm is difficult and takes time there are multiple sources of evidence pointing to the fact that harm has been extensive. These include adverse event reporting, prospective surveys, disability claims and comparing countrywide data on ambulance calls and hospitalisations overall and for specific conditions and deaths. |
8.1 It takes time to do adequate safety testing
In February 2020, Professor Whitty said, “The rate limiting steps are late clinical trials for safety and efficacy, and then manufacturing. For a disease with a low (for the sake of argument 1%) mortality a vaccine has to be very safe so the safety studies can’t be shortcut. So important for the long run.”
In the same email exchange, Sir Patrick Vallance said, “They would then need to go through safety testing, small scale trials in people and then larger efficacy trials. So it may all work out but it is not going to be ready in weeks. All of these approaches will take many months at the very and most optimistic best.”
In the early months it was assumed that a properly researched vaccine would take at least one or two years to develop. The usual time frame is 10-15 years.
The belief that vaccines were safe had led to a circular belief that vaccines required fewer safety checks than other novel therapies. Pfizer-BioNTech’s non-clinical overview document revealed that pharmacological safety studies, genotoxicity and carcinogenicity studies were not conducted as they were “not considered necessary.” The original Human Trial Information Sheet acknowledged this fact, “Due to the urgent need for a vaccine against Covid-19, with agreement from the MHRA, some of the tests usually required for a newly manufactured vaccine have been modified, in order to make the vaccine available more quickly for assessment in this clinical trial.”
Even after “temporary authorisation” the regulator did not demand these studies and continued on to give full authorisation for 12 years and older in September 2022.
Claims re safety were always of necessity unsubstantiated, given the short duration of the trials (follow-up of only two months at the time of first authorisations). The best that could be said was around estimates of immediate side effects and an indication of how rare a condition would have to be for it not to be picked up in the trials. For example, had there been 80% more deaths in the vaccine arm of the Pfizer trial, implying 1 death for every 5,000 people injected, it still would not have reached statistical significance. Similarly any problems that only occurred in a subgroup of those in the trial would be even harder to demonstrate. There were no communications that indicated this level of uncertainty regarding safety.
In October 2020, Steven Anderson who is in charge of drug safety monitoring at the FDA made a presentation in October 2020 where he listed 22 “possible adverse events” and said they had determined the list using potential concerns raised by pharmaceutical companies, the medical literature and regulatory experience with vaccines and this particular platform. The slide was shown two and a half hours into the meeting and was only visible for one second. The list included demyelinating diseases, seizures, stroke, narcolepsy, allergies, acute myocardial infarction, myocarditis/pericarditis, autoimmune disease, deaths, pregnancy and birth outcomes, clotting issues and thrombocytopenia, arthritis and joint pain, Kawasaki disease, multisystem inflammatory syndrome in children and vaccine enhanced disease.
The main Pfizer/BioNTech trial is not due to complete until March 2026. In November 2022, Pfizer and Moderna launched trials with five year follow up to better understand the adverse reactions. This should have happened before mass vaccination, not over a year later.
On 10th January 2020, Albert Bourla, CEO of Pfizer said, “Current vaccines… don’t have the safety profile that we hoped we can achieve.”
8.2 Diverse types of harm
There were several potential mechanisms of harm that could each affect a multitude of organs and cause a multitude of conditions.
a. Lipid nano-particles
The lipid nanoparticle delivery system works by merging with cell membranes such that the exogenous lipids become incorporated as part of cell membranes. The lipids have electrostatic charge and this, along with other differences, may cause cellular disruption that could result in disease. The toxicity of these products, while well established, has not been thoroughly investigated before the decision to inject billions of people worldwide.
b. Cell death
The primary mechanism of action was to cause widespread expression of spike protein (and other unknown proteins) in cells throughout the body. The immune response to such expression is to kill the affected cells. While this would educate the immune system it will also cause organ damage where the cells have been killed. Whether this would be significant enough to result in disease will depend entirely on the number of cells affected. The extent of such cell damage in each organ has not been quantified.
c. Synthetic nucleotides
DNA codes for genes and the code is copied into mRNA before being copied again into the proteins that allow cells to function properly. mRNA molecules are made up of nucleotide building blocks. The mRNA molecules had a disproportionate amount of N1-methyl-pseudouridine compared with natural mRNA. This was deliberate as it significantly increased the longevity of the mRNA which otherwise would be destroyed within around half an hour. After the body breaks down the injected mRNA these building blocks would be incorporated into the RNA produced as a part of normal cell function. Therefore, proteins would be produced for an extended length of time. It is not known what effect that would have but cells throughout the body would have been affected in this way.
d. Small vessel damage
It is easiest to see small vessel damage by looking at the retina. A study in Taiwan showed an increased risk of retinal vessel occlusion which can cause blindness present in all ages. The risk after 12 weeks was three times as high as background rates and accounting for a whole two years the risk was double with an additional case for every 300 over 65 years olds and 1000 18-64 year olds vaccinated. Rather than present evidence on mechanisms and epidemiology for each condition I am going to focus on the bigger picture. Small vessel damage was not rare with a tripling in the first three months in the risk of occlusion of the small vessels of the eye, where such damage is easily measured.
e. Autoimmune damage
The spike protein has 80 percent genetic overlap with human proteins which seems remarkably high. There is therefore a significant risk of the immune system being trained to attack self-protein which could affect any organ in the body.
f. Endotoxin damage
Contamination of the vaccine contents by bacterial endotoxin could have resulted in a multitude of different conditions. The Comparative Toxicogenomics Database lists 9,956 conditions caused by endotoxins.
g. Contaminant DNA
The vaccine vials were also contaminated by the bacterial DNA used as a template to produce mRNA. The DNA had five attributes that would have maximised the risk of the DNA being transported to the nucleus of the cell. Viral DNA can integrate into the human genome and when it does so it can disrupt genes causing them to be switched off or activate genes, switching them on. In cell experiments the viral DNA has been shown to integrate into human DNA. This has not been shown yet for vaccine DNA nor in living people.
h. Unknown proteins
The proteins that were produced as a result of mRNA vaccination were numerous and have not been fully characterised or measured. These occurred as a result of
- truncated mRNA, whereby shorter proteins were produce that would have folded in a unique way
- Novel proteins produced as a result of slippage in the code i.e. frameshifting, such that the amino acids were each different to what was intended
8.3 Difficulties measuring harm
The assumption that an adverse event is limited to a singular condition significantly impeded the recognition of widespread harm. Regulators, by comparing reports of individual conditions, overlooked the broader spectrum of numerous reported conditions, mistakenly interpreting this as a change in reporting behaviour rather than an actual increase in adverse events.
The evidence from the original trials indicated that 1 in 800 mRNA recipients would have a serious adverse event of special interest, these are reactions that were agreed to be meaningful that were decided on prior to the trial. This result was based on the process 1 product in the Pfizer/BioNTech trial and excludes cases like Augusto Roux whose adverse event was not recorded in the data. Overall the risk of a serious adverse event of special interest was twice as high as the chance of preventing a severe covid case.
From the onset of its rollout, the adverse reaction monitoring systems exhibited significant warnings, which were attributed to heightened awareness rather than actual increases in adverse events. During this period, incident reports for other drugs did not show a similar uptick, indicating a specific issue with this drug not with an increased awareness of the reporting system.
The detection of rare side effects, such as brain clots and myocarditis, is more straightforward due to their immediate occurrence post-administration and their significant impact on the overall incidence of these rare conditions. Conversely, identifying increased incidence in common conditions requires a substantial surge in the number of cases.
Only a fraction of the complications is reported. For example, there were 43 times more cases of myocarditis and pericarditis in the real world than in the US reporting system. The US Vaccine Adverse Event Reporting System (VAERS) was so overwhelmed with reports that they had to hire 300 extra staff. Even with these extra staff there was a backlog of 94,000 uncatalogued reports by the end of 2021. For historical adverse event reports 15% were reports of serious adverse events However, for covid vaccines that rose to 25%.
Data released from the US VAERS reporting system indicates potential harm for 770 conditions. Notably, two-thirds of these conditions presented stronger safety signals than myocarditis and pericarditis, which were only recognized as genuine adverse events in mid-2021. Many UK doctors have also publicly expressed concerns about the harm caused by these novel products.
It has been difficult to measure the adverse reactions from the vaccines for three separate reasons:
- some were uncommon;
- some were slow to emerge;
- the risk was not present in every batch of vaccine.
Many studies attempted to measure the incidence of various conditions after vaccination. There is a markedly low incidence of all conditions immediately after vaccination. This is referred to as the “healthy vaccinee effect” and occurs because people self-select when to be vaccinated such that new diagnoses are rare afterwards. That means that the baseline for comparison should be the lower rate seen for other conditions after vaccination, not the overall higher rates seen in the whole population. However, the researchers and regulators have invariably chosen a higher threshold and then claim there is no signal present.
8.4 Adverse Event Reporting Systems
The MHRA did not set a safety threshold which would cause for a suspension of a drug pending investigation. Instead it judges safety in relative terms:
“For a medicine to be considered safe, the expected benefits of the medicine will be greater than the risk of suffering harmful reactions.”
There is also a major ethical issue here when the individuals at higher risk of harm are not the same ones who stand to benefit. However, the measure of risk is well known to be underestimated until time has passed to allow comprehensive collection of data. For example, Public Health England significantly increased their estimate of narcolepsy from Pandemrix ten years after the injections.
An alternative measure is to carry out a prospective study of a cohort of vaccinees recording their adverse events. The results of such a survey in Israel was hidden but a Ministry of Health meeting was secretly recorded. The data showed serious side effects that were not short term. The vaccines were shown to be the cause as demonstrated by symptoms worsening or returning after another dose.
The investigation was led by an expert outside of the Ministry of Health, Prof. Mati Berkowitz who said, “We will need to think about this medico-legally…so they won’t come afterwards with lawsuits.” The investigating team only looked at the top five most common side effects. The sixth was cardiovascular and was not reported on. Critically, the survey highlighted the same issues as the reporting systems. They then released a fabricated report to make the vaccines look safer. They took the side effects that occurred in those few months from that small sample in the study and say they were due to all the vaccines given in the country ever and included men in the denominator for menstrual side effects.
Germany carried out two surveys on post vaccine side effects including one of over half a million people. They found that “serious adverse events,” which are side effects that led to hospitalisation or life changing disability or death were seen in 1 in 142 people, for AstraZeneca and 1 in 500 for Pfizer/BioNTech. Those will include a small number of genuine coincidences. Reports filed by German doctors put the figure for serious reactions at 1 in 3,300 by September 2022.
The board of a German health insurer wrote to the German authorities saying, “The data available to our company gives us reason to assume that there is a very significant underreporting of suspected cases of vaccination side effects after corona vaccination…it is likely that 2.5-3 million people in Germany received medical treatment because of side effects of vaccination after the Corona vaccination. We see this as a significant alarm signal.” The CEO was sacked five days later.
The Norwegian reporting system showed that doctors reported serious adverse events occurred as frequently as 1 in 200 doses for AstraZeneca, 1 in 1862 for Moderna and 1 in 2325 for Pfizer-BioNTech.
8.5 Overall impact
Vaccine rollout coincided with a rise in pressures in hospitals. Whereas covid had never resulted in a reduction in the number of empty hospital beds, once the vaccine rolled out there were increasing numbers of inpatients (see Section 7.8b figure 47). From May 2021, the total NHS bed capacity available in January 2021 had been exceeded and the numbers continued to rise since then (see figure 47 in section 7.8b).
At the same time as there were reports of an accident and emergency crisis in the UK, hospitals were overwhelmed in the USA. Covid had never overwhelmed total hospital bed capacity anywhere. In late 2021, the ‘vaccinated’ were attending the emergency department five times more frequently than the ‘unvaccinated’. All ambulance calls for life threatening conditions increased by 25 percent, an extra 500 calls every day from June 2021.
Figure 65: Ambulance calls for life threatening conditions showing stepwise rise with vaccine rollout
As well as immediate effects from the vaccine there may be effects that take longer to emerge. This can be true for autoimmune conditions and was true for the 8 month lag in narcolepsy diagnoses from Pandemrix vaccine. It can also be true with regard to pathologies which develop over time. Heart attacks can be caused by direct damage to the electrical circuitry of the heart, e.g. from inflammation or scarring because of myocarditis, or else can be due to slow narrowing of the vessel walls supplying the heart muscle due to inflammation. There continues to be an unprecedented increase in cardiac arrest calls and large numbers of cardiac deaths even now (see section 8.11).
Attempts to show the vaccine is safe have used a random period several weeks after vaccination as a control to compare to the period immediately after vaccination. The impression of there being no risk can thus be given when in fact the risk has not yet dissipated.
The numbers waiting for NHS care on waiting lists is disproportionate to the numbers whose care was delayed.
Figure 66: Numbers on an NHS waiting list showing dip during lockdown as people did not present followed by a massive surge after the vaccine rollout
The MHRA Yellow Card system, like every international vaccine safety system showed signs of serious problems from January 2021 but these have been ignored. In adults, 11.1% of reports for the covid vaccines were for serious adverse reactions compared to 5.5% for non-covid vaccines. This was statistically significant.
A very basic analysis just compares reporting for one vaccine to another. If it is assumed that the AstraZeneca vaccine is completely harmless it can be used as a control to see how much extra reporting there was in each age group for certain conditions for the other vaccine types. This showed clear signals such as high cardiac adverse reactions in young men but it also showed severe blood disorders, particularly in females and reproductive adverse events for Pfizer but not Moderna.
The fourth dose resulted in nearly a quarter of healthcare workers being unable to work the next day.
8.6 Disability Data
The Pfizer and Moderna clinical trial data shows a higher rate of serious adverse reactions from vaccine (12.5 per 10,000) than any reduction in serious events from covid (2.3 and 6.4 per 10,000 for Pfizer and Moderna respectively).
As well as sickness needing immediate care, there was a notable rise in people who were not working because of long term sickness which was not seen in 2020 but began in spring 2021 when the ‘vaccine’ was rolled out to the working aged population.
The Governor of the Bank of England commented on the drop in the labour force to the parliamentary treasury committee in May 2022, “Since the end of 2019, we’ve seen a fall in the size of the labour market of around 450,000. It’s a very big fall by historical standards. It reflects a 3% increase in the number of economically inactive people. The persistence & scale in this drop has been a surprise to us. We’ve seen an increase in long-term sickness in that number of about 320,000 people. The scale & persistence of the fall in the labour force has been very unusual…the notable difference this time we have got this long term sickness element which is quite large. I have to be honest we don’t know much really about what’s behind that. We’ve discussed it with health experts. We’ve asked, “is it long covid?” The estimated total number of people not working because of long covid was only 80,000.
Figure 67a and 67b: The rate of economically inactive working-aged people due to long-term sickness in England, females top graph and males bottom graph
The rise was also evident in the USA disability data.

Figure 68: USA data showing rise in people over 16 years of age with a disability
8.7 Broad categories of harm
It is a general rule of thumb that the first indications of a drug safety problem will underestimate the size of the problem due to poor measuring of the extent of illness.
It is easy to notice a higher rate of a rare condition. However, when there is a rise in a condition that is already common, like strokes or heart attacks, the extra diagnoses can be lost in the noise. It takes more work to identify the problem e.g. by looking only at younger age groups where the underlying risk is much lower. Such work has barely begun.
Within the first year indications of three types of harm were recognised: risks to the heart, the blood and the nervous system. The full extent of these acknowledged issues are yet to be measured.
Heart risks
For a long time the myocarditis risk was thought to be confined to mRNA vaccines and young males. However, further investigation suggests myocarditis in more age groups and in females too (see section 8.10). Concerns extend to potential heart scarring and related rhythm disorders. It has also been hypothesised that the underlying pathology may not be inflammation but abnormal protein deposition causing a condition called amyloidosis. Furthermore, other cardiac issues appear to show an association with vaccine rollout.
Blood Clots
First concerns were raised linked to the AstraZeneca vaccine where rare instances of brain clots were noted associated with vaccine-induced antiplatelet antibodies. There were recommendations that AstraZeneca should be reserved for older age groups from April 2021. Denmark ceased giving AstraZeneca in April 2021 after giving 150,000 doses. The UK had given 9.7 million doses at that point and went on to give 39 million more (to all ages).
Many clinicians raised concerns about what they were seeing in their practice. In particular, post operative clotting disorders, odd clotting conditions like portal vein thrombosis and clotting of the artery of the gut, both of which are normally incredibly rare, seemed to become more common after vaccine rollout, including in those given mRNA products. Because these are so rare it should be possible to measure any increase but such studies have not yet been published.
One of the pathological outcomes from spike protein expression is that it causes cells to fuse with each other which can lead to clot formation. When spike is introduced to blood with or without cells in a laboratory setting, it binds directly to the main component of blood clots, fibrinogen, producing abnormal clots. Therefore, other clots might also be caused by any of the vaccines. Where a type of clotting occurs more commonly as a background rate, proving there has been a rise is harder. Israeli data shows a clear rise in pulmonary embolism with mRNA rollout and an FDA paper showed an increased risk of pulmonary embolism but this finding was denied because of how the data was analysed. Regulatory bodies have acknowledged related risks, such as abnormal menstruation, having repeatedly denied such a link before despite receiving 30,000 reports from individuals with problems.
Neurological/Autoimmune Reactions
One AstraZeneca trial was suspended because of neurological adverse reactions. The Government acknowledged vaccine-related Guillain-Barre syndrome (where the immune system attacks the nervous system leading to life threatening or disabling weakness or paralysis) in relation to AstraZeneca. Although the government recognised a problem in 2021, they continued to advise that people who had had post vaccination Guillain Barre syndrome should receive further doses.
Many patients complained of a series of new conditions and a clear pattern emerged of the types of harm with many patients having multiple of these new conditions. These included tremors, POTS, postural tachycardia syndrome (a disabling condition where standing or sitting-up leads to a racing heart beat as blood flow to the heart and brain fails to be maintained) and various autoimmune conditions.
However, an important study spanning six neurological departments in the USA demonstrated that these patients have an underlying mechanism for their neurological symptoms. The study only described the presentation of 23 patients, 92% female, all of whom developed symptoms within days of vaccination (half within minutes or hours of their dose). Those with prior conditions or risk factors for neurological problems or other causes for small nerve damage were excluded. None had had symptomatic covid. They all had abnormal sensations (esp burning) in face or limbs and 60% had blood pressure drops on standing, heat intolerance and palpitations. Half of those tested had damage to the autonomic nervous system preventing normal sweating or leading to POTs syndrome.
These doctors thoroughly investigated these patients and found skin biopsies demonstrated nerve abnormalities. When there has been an immune reaction, where antibodies have bound a target leading to the triggering of immune cascades, a marker is left behind at the site called “C4d”. This marker was identified at a higher rate in the blood vessel walls of the patients than controls. Some of those with normal skin biopsies had demonstrable abnormalities of the nerves elsewhere e.g. those that control blood pressure and heart rates. Two out of the five tested showed protein within the cerebrospinal fluid in keeping with raised antibody levels and indicating inflammation.
These doctors successfully treated their patients with corticosteroids or immunoglobulins which indicates an underlying autoimmune pathology.
Seizures in Children
The Pfizer/BioNTech trial data showed a clear risk of seizures with three cases in the vaccinated and none in the placebo group.
A US CDC study claimed there was no risk of seizures in children under 5 years of age. The study looked only at the first three weeks after vaccination compared risks only to the same vaccinated children in a later period rather than to an unvaccinated or historical control.
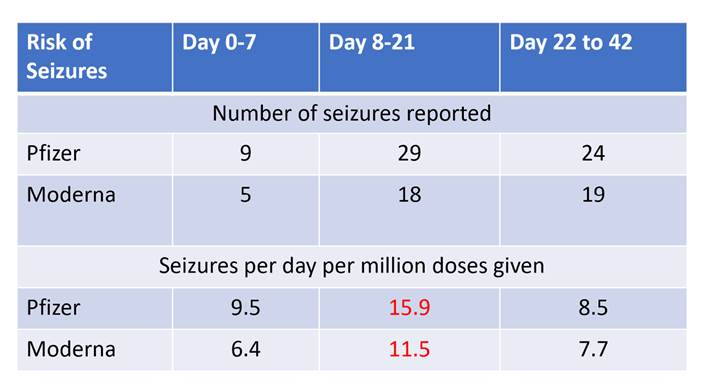
Table 14: CDC data on seizures in children after vaccination
A separate study looked only at the first seven days after injection thereby also avoiding the danger period.
The similarities between long COVID and vaccine injury symptoms suggest a shared mechanism involving the immune system’s response to foreign proteins
When assessing these impacts many people have compared vaccine harms to alleged risks from the virus. However, given that lack of efficacy at preventing infection the risk from the virus has not been shown to be prevented by vaccination. Rather they are additive, or potentially synergistic.
8.8 Myocarditis and other cardiovascular issues
The government advice on this issue is nothing short of reckless. The general theme is not to worry if symptoms are ‘mild’, no need to investigate and if it all settles you can just postpone the 2nd dose from 8 weeks to 12 weeks. This advice is both dangerous and based on no known scientific evidence.
There are multiple potential mechanisms of harm to the heart and more than one may be relevant:
- The immune system can be misdirected to attack heart molecules – this is known as ‘molecular mimicry’.
- Lipid nanoparticles can cause heart damage directly through their proinflammatory effect.
- Expression of a foreign protein leads to immune attack and cell death which would result in heart inflammation i.e. myocarditis
- Spike protein may harm myocytes directly.
- The fact that numerous different proteins were produced as a result of these injections means that there may be a multitude of potential mechanisms. Without details about what these proteins all were it is impossible to know what their role may have been.
- An increase in inflammation can contribute to the narrowing of coronary arteries from atherosclerotic plaques that can lead to a diminished blood supply to the muscle of the heart resulting in either angina, while the muscle struggles to stay alive or a myocardial infarction where the muscle dies.
There is now evidence that these products circulated throughout the body which means there would have been extensive exposure to the circulatory system including the heart.
a. First indicators of myocarditis / pericarditis
Vaccine-induced myocarditis was first reported from the US in April 2021 and from Israel in June 2021 with cases being noted in young males after the second dose of mRNA vaccine. Cases occurred at a median of 2-3 days post immunisation and presented with chest pain and raised cardiac enzymes. The incidence of the condition is unclear as it has depended on voluntary reporting systems ranging from 1 in 10,000 in the US to 1/3000 in Hong Kong for the 16-19s age group. But a prospective study from Thailand from two large secondary schools, found an extremely concerning 29% with cardiac symptoms and 1 in 43 with subclinical myocarditis, based on bloods taken at 3 and 7 days post second vaccination. Similarly, 17% of high school students in Taiwan had cardiac symptoms and 1 in 35 had subclinical myocarditis in Switzerland. Similar studies should have been carried out in the UK.
In early 2021, healthcare professionals from various institutions, including those in Israel and within the U.S. military, observed a series of myocarditis cases post-vaccination. Myocarditis, an inflammation of the heart muscle, was detected shortly after the administration of COVID-19 vaccines. Despite these observations, the information was not immediately disclosed to the public.
In February 2021, a safety alert regarding these incidents was entered into the Vaccine Adverse Event Reporting System (VAERS), but it did not receive adequate analysis at that time. Subsequent months saw the passing of a 22-year-old woman in Israel in March and a 35-year-old Israeli man in April, both post-vaccination. Despite over a hundred domestic reports in VAERS and international alerts, including a significant number of cases in Israel, the U.S. Centers for Disease Control and Prevention (CDC) and the UK’s Medicines and Healthcare products Regulatory Agency (MHRA) did not formally acknowledge the issue until May 2021.
Furthermore, in April 2021, a leaked report from the Israeli Health Ministry documented 62 cases of myocarditis following vaccination. It said, “There is specific concern regarding the frequency of the occurrence observed in men under 30 in the days immediately after the second shot.” Despite this, organisations such as the MHRA, CDC and the American Academy of Pediatrics reassured the public in June 2021 about the mild nature of most cases, leading to continued vaccination recommendations.
Additional concerns were raised by Brown University epidemiologist Dr Andrew Bostom and myself in a June 2021 publication, where we emphasised the risks of myocarditis, particularly in young individuals. We cited cases, including a 16-year-old with post-vaccination myopericarditis. He developed scarring of the heart and his troponin levels — a silent marker heralding potential heart cell damage even without overt symptoms – were high enough to predict a tenfold increased risk of mortality. We called for urgent research to measure troponin levels in the vaccinated and declared “the FDA’s intention to only continue monitoring is a dereliction of duty.”
In July 2021, Pfizer updated their trial consent forms for entry into clinical trials to include myocarditis and pericarditis as potential risks, but did not widely publicise this information.
By September 2021, Hong Kong had vaccinated 65% of adolescents and decided not to give them second doses due to myocarditis concerns. However, the vaccine continued to be administered globally, and by July 2022, cases of myocarditis in children as young as eight were reported.
b. How common was it?
Table 15 below summarises the evidence for the incidence of myocarditis in different age groups and populations. The data is presented as the number of cases per million doses for the period studied (which differed between different studies).
Table 15: Estimates of rates of myocarditis in the vaccinated and unvaccinated with and without infection
One measure of cardiac injury is a blood test for a cardiac enzyme called Troponin. Pfizer was compelled by the FDA to carry out research to measure the extent of subclinical myocarditis in August 2021. They were asked to provide an interim report in October 2023. The study began in November 2022 but the end date keeps being extended and it is now due to finish in November 2029.
Independent scientists in Thailand carried out this work on adolescent males showing 29% had symptoms, 18% had ECG changes before and after the vaccination and 3% showed a rise in blood Troponin levels. The study was then repeated on working age people (median age 37 years) at a Swiss University which showed similar results including in females. A smaller study of adolescents in Taiwan also replicated these findings.
Table 16: Rates of cardiac symptoms, ECG changes and raised troponin levels among different population groups
A team in Hong Kong published in August 2021 that intravenous injection of mice with the Pfizer product resulted in myocarditis and pericarditis in 38% of the mice. Intramuscular injection was not seen to have an effect, but a 3% effect would have been too small to see in the small numbers of mice they used.
Figure 69: Mouse hearts at post mortem. Left heart is normal and right heart shows pericarditis after intravenous injection
c. Cases of Myocarditis in the Adverse Event Reporting
The WHO’s Vigiaccess reporting system reports on all covid vaccines included 28,929 reports of myocarditis and 23,599 reports of pericarditis (with potential duplication).
VAERS – the US vaccine adverse events reporting system reports 17,380 myocarditis cases. Half of these had an onset within one week of injection. These included 442 deaths,142 of whom died within a week of injection. For comparison for all other vaccines there were 788 cases of myocarditis up to 2019 for all other vaccines.
Note that a huge underreporting factor is suspected for VAERS for a variety of reasons. Moreover, VAERs has been criticised recently (BMJ) for running a hidden system containing follow-up information.
d. Cardiovascular Adverse Events in Post-marketing Surveillance
Pfizer’s cumulative safety report of all AEs received up till end of Feb 2021 reported 1441 “cardiovascular adverse events of special interest” of which 946 were serious. Half of these occurred within 24 hours of dosing.
Table 17: Post marketing reports of adverse events after Pfizer/BioNTech vaccination
e. The Consequences of Myocarditis
Patients are advised not to engage in vigorous exercise for the rest of their lives. Scarring of the heart results in a lifelong increased risk of arrhythmia and sudden cardiac death. Implantable defibrillators are recommended for some. A dilated cardiomyopathy can result after myocarditis, leading to heart failure and death
The government has stated that myocarditis is very rare and is usually mild with recovery after a few days. This is not born out by the facts. In a US cohort of 63 children admitted to hospital with chest pain all made a quick clinical recovery but nevertheless 85% of them had abnormalities on cardiac MRI scans. Although in the majority of these, there has been an improvement in severity and as yet no reported deaths, nevertheless the long-term effect on cardiac function is entirely unknown. A survey of post vaccine myocarditis patients (median age 17) showed 23% still had abnormal ECGs and nearly 46% had abnormal MRI when followed up after 90 or more days. 20% could not perform “usual daily activities.” There was bias as 38% did not respond, but it is naive to think this is a mild problem that can be dismissed. A separate study showed 58% of covid vaccine induced myocarditis confirmed by MRI was not resolved at one year.
f. Outcome data for viral myocarditis
Data available to date gives no reassurance that post-vaccine myocarditis will be any milder than post-viral. 3-4% of those with acute post-viral myocarditis require heart transplantation. The overall mortality rate for viral myocarditis after one year was 20% and after five years 44% to 56%.
g. Outcome data for post vaccine myocarditis thus far
After inflammation the body heals with a scar which in the heart causes two problems. The heart functions by contraction and a scarred area cannot contract, instead it will bulge out, reducing the efficiency of each pump cycle. Ultimately this can result in heart failure. Secondly, the heart has a delicate electrical system and a scar can cause a short circuit leading to a potentially fatal arrhythmia. Late gadolinium enhancement is a marker of scarring in the heart seen on cardiac MRI. LGE seen in several studies confirm likely permanent damage is not at all rare after vaccine-induced myocarditis:
- Hong Kong study of 40 children
- USA study of 63 cases
- London 5 adolescents
- Japanese retrospective look at PET scans done for other reasons (mainly looking for cancer) – found a significant increase in cardiac metabolic activity (indicative of inflammation) compared to unvaccinated patients:
Figure 70: Pet Scans examining cardiac metabolic activity
h. Post-mortem evidence
The UK has only been carrying out limited post-mortem work for many years with coroners reluctant to authorise taking of tissue samples since the introduction of the Human Tissue Act which has criminal penalties. Proper examination of heart tissue at post-mortem requires the taking of tissue samples and can require specialised dissection skills which only a few pathologists have. A few publications from post-mortems include:
- Spike protein was shown in heart cells at postmortem in a person who died of myocarditis who had not had covid.
- Two adolescents both died of myocarditis within days of Pfizer injection shown at post mortem
- Study of 12 patients dying within 30 days of vaccination – 24 ventricles in total. Testing for vaccine RNA was negative in the 17 ventricles without myocardial injury but positive in 4 of the 7 with myocardial injury.
- A 55 year old died 4 months after his injection with evidence of myocarditis. He also had thrombus blocking the coronary artery without evidence of rupture of an underlying plaque as well as microthrombi in smaller vessels. Further investigation revealed inflammation of the vessel walls along with spike protein in the absence of other viral proteins indicating it was vaccine derived.
i. Did covid cause myocarditis?
There are cases of myocarditis following covid as with other viral infections. Prior to vaccines, post viral myocarditis did occur but only at the same rate as before – ie SARS-CoV-2 was causing myocarditis at the same rate as viruses that it had replaced as it had in the past. An Israeli study demonstrated no increase in myocarditis from covid prior to vaccine rollout. The incidence of myocarditis (and pericarditis) rises from spring 2021 not before as was seen in Israeli and German hospital databases and in a study from 40 hospitals in the USA (e.g. see figure 71 below from US study). After vaccination, myocarditis after infection became much more common than it had been before vaccination.
One possible explanation for that would be myocarditis being caused by “molecular mimicry” where there is overlap in a foreign protein resulting in the immune system being misdirected and attacking similar proteins in the heart. This is a known aetiology of myocarditis from other causes. With this mechanism a vaccine could prime the immune system such that a viral infection would trigger myocarditis.
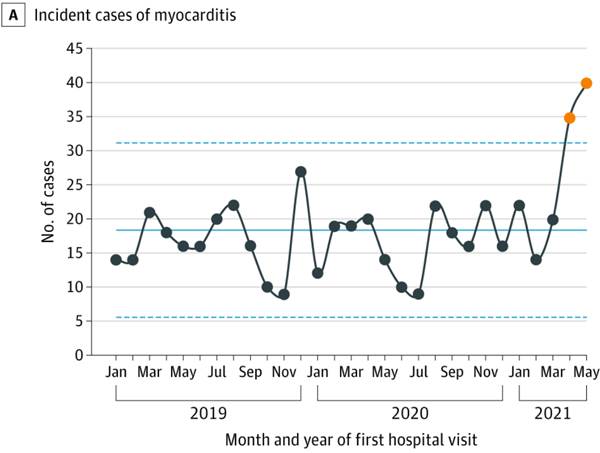
Figure 71: Incidence of myocarditis from 40 US hospitals over time
Moreover, if the vaccine increases risk of infection (as it appears to) this would counteract any protection anyway, especially given that there is no evidence that the vaccine actually protects anyone from myocarditis post-infection, nor any credible mechanism why it should.
UKHSA (and previously PHE) use Google Search data as a tool for tracking public health. Figure 72 shows how closely searches for myocarditis tracked vaccine doses.
Figure 72: Google search results for “myocarditis” as a percentage of maximum searches in that time period, plotted against vaccine doses given to under 50 year olds
Despite the clear evidence that the increased incidence occurred with vaccines there have been attempts to blame the virus as was seen with Pandemrix. Such studies have either failed to control for the fact that in spring 2020, there was a bias with only the sickest people tested for covid such that they cannot be compared to a healthy control group. Other studies report on an increased risk after covid but fail to demonstrate whether the unvaccinated were at any increased risk. As myocarditis is potentially and immune mediated illness, priming of the immune system with vaccination could lead to a problem after exposure to the virus such that restimulation with viral spike causes the immune system to attack the heart such that restimulation with viral spike causes the immune system to attack the heart.
j. Cardiac Arrests
From spring 2021 there was a stepwise 25% rise in calls to ambulances for life threatening emergencies including cardiac arrest which has not returned to baseline.
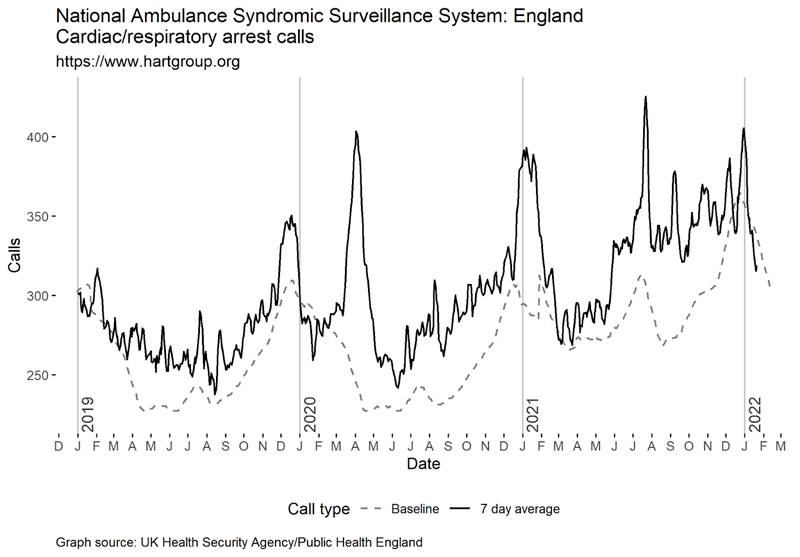
Figure 73 PHE / UKHSA data collated by HART on ambulance calls for cardiac/respiratory arrest showing covid/lockdown waves with further stepwise increase from spring 2021. Note the claimed rise in the baseline expectations at this time point.
k. Sudden deaths data in trial
Although there were a similar number of sudden or unexpected deaths within two months in the trial data, there were 5 in the vaccinated group after that period compared to only 1 in the placebo group.
l. Unexplained excess deaths
Since the vaccine rollout there has been a stepwise increase in mortality with two periods where deaths returned to baseline because of fewer than expected respiratory deaths in winter. The deaths are disproportionately in the young and are predominantly from cardiovascular causes (see section 8.10). This needs further investigation as a matter of urgency, as these products continue to be administered to younger populations.
m. Atherosclerosis
The most common kind of cardiac death is from narrowing of the coronary arteries due to atherosclerotic disease. Systemic inflammation increases the risk of cardiac disease.
In a study involving over 500 middle-aged patients who were regularly monitored, a predictive scoring model using inflammatory markers linked with heart attack risk indicated that the mRNA vaccine potentially elevated the likelihood of a coronary event within five years from a pre-vaccine rate of 11% to 25% within 2–10 weeks following mRNA vaccination. A notable early critique of this study’s conclusions pointed out the absence of a control group. Despite this, if the results hold any degree of accuracy, it suggests a significant increase in the progression of coronary artery disease and, more critically, the risk of heart attacks, occurring just months after receiving the vaccine.
Dr Aseem Malhotra alleges that an individual working for a British Heart Foundation research team told him that they had been asked to sign non-disclosure agreements after their team noted a significant increased risk of coronary vascular inflammation after vaccination.
HART sent an open letter to the British Heart Foundation and Charity Commission in January 2023 to ask them to investigate but, despite chasing, have had no response from either.
Studies claiming covid leads to heart disease almost always include spring 2020 positive covid cases. These cases are biased as testing was not readily available. People with a high likelihood of heart disease e.g. the hospitalised, were much more likely to be tested than people who were otherwise healthy. Comparing this group to the population as a whole is not reasonable. Comparing the risk of a myocardial infarction to people who had just had another cause of pneumonia showed that there was no reduced risk with covid.
In Israel, there was a 25 percent rise in ambulance calls for cardiac arrests or coronary heart disease among 16 to 39 year olds. The rise was correlated to vaccination and not covid waves.
Scotland changed their data definitions in July 2021. This meant that the significance of a rise in out of hours chest pain consultations to GPs in 15-44 yr olds could not be assessed, even though the same change in definition did not affect other age groups. Scottish ambulance calls for cardiac problems in 15-44 year olds saw a similar rise as in other age groups.
Figure 74: Public Health Scotland Data showing ambulance calls for cardiovascular issues
8.9 Australia and Singapore: accidental ‘control’ groups
In order to understand whether vaccines could have caused this rise it is helpful to look at places that had had minimal covid before their national vaccine roll-out.
South Australia normally sees around 1,300 cardiac presentations per month for 15-44 year olds. This rose sharply in August 2021 with vaccine rollout, peaking at 2,172 in December. The whole state had seen only 1000 covid cases by 15th December. Australia had had minimal covid prior to the rollout of the ‘vaccines’ and have opposite seasons and can act as a control group.
By May 2021, there was an ambulance crisis even though there were fewer than 100 covid patients in all hospitals in Australia. By October, despite it being springtime in Australia headlines reported on ambulances unable to drop off patients in hospitals that were at full capacity. In Oct 2021, Mark McGowan, Premier of Western Australia, said he could not explain the overwhelmed hospitals, “Our hospitals are under enormous pressure. This has been something no-one has ever seen before. Why it is, is hard to know.” In April 2022, Yvette D’ath Queensland health minister said she could not explain the rise in the most urgent ambulance calls (“code ones”): “I don’t think anyone can explain why we saw a 40% jump in code ones… We just had a lot of heart attacks and chest pains and trouble breathing, respiratory issues. Sometimes you can’t explain why those things happen but unfortunately they do.”
Western Australia and South Australia had almost no covid before Omicron. Up to mid-December 2021, Western and Southern Australia had had around 1000 cases each.
Despite having fewer than 1000 covid cases prior to December 2021, South Australia saw 25,800 extra ambulance calls (mostly cardiac) in the year from July 2020 to June 2021 compared to previous years. There was a year-on-year increase from 2018 to 2019 and 2019 to 2020 but the rise in 2021 was about double the increase seen in the preceding two years. There was a clear rise in attendances for particular conditions which correlated with the ‘vaccine’ rollout.
A Freedom of Information request showed that South Australia normally sees around 1,300 cardiac presentations per month for 15-44 year olds. This rose sharply in August 2021 with ‘vaccine’ rollout, peaking at 2,172 in December, before covid hit. This was not due to covid – the whole state had seen only 1000 covid cases by 15th December.
Queensland doctors called the problem a “ticking time bomb” in April 2021and described a “flood of patients.” By April 2022, Yvette D’ath Queensland health minister said about the most urgent ambulance calls (“code ones”), “I don’t think anyone can explain why we saw a 40% jump in code ones… We just had a lot of heart attacks and chest pains and trouble breathing, respiratory issues. Sometimes you can’t explain why those things happen but unfortunately they do.”
A similar control group is Singapore which also had minimal covid prior to Omicron but saw an excess of cardiovascular deaths from 2021, although data has been annualised.
A paper from Singapore which was written by those responsible for their vaccine programme claimed that covid was to blame. They compared people who tested positive from September to November 2021 with those who tested negative from April 2020 to December 2022. There is no need for this difference given the vast majority would be in the latter category. They said, “COVID-19 survivors did not exhibit higher risk of all inflammatory heart disease” indicating that covid was not linked to myocarditis and pericarditis. They also claimed an increased risk of heart failure and non-ischaemic cardiomyopathy (which would include post myocarditis problems) in those post covid. However, more than half of the people they included as “unvaccinated” had in fact been vaccinated making any interpretation about differences between groups meaningless.
Monthly mortality data shows a clear rise in the gradient of non-covid deaths after the vaccine rollout, with only a small fraction of the increase attributable to covid (see figure 75).
Figure 75: Monthly deaths in Singapore before and after January 2021 with covid deaths shown in green.
Australia also saw a rise in deaths before any significant covid and it has just got worse since. Note the government chose to plot covid infections rather than covid deaths on this chart. Apart from a quiet winter season in 2021, there was an excess mortality (red line) above the 2015-2019 baseline (orange line) which was more marked from February 2021. Note the marked increase in the “normal” baseline in the more recent graph used for 2022 and 2023.
Figure 76a and 76b: Australian total deaths in red plotted against average and range from previous years in 2021 (top graph) and 2022 and 2023 (bottom graph)
8.10 Deaths
The first reports that led to authorisation had one more covid death in the placebo group of the AstraZeneca and none in the Pfizer-BioNTech trial. The Moderna trial claimed that of seven deaths in December 2020 there were zero covid deaths but two months later said there had only been five deaths and one of the placebo deaths now was due to covid.
The publications at 6 months reported one more covid death in the placebo group of the Pfizer/BioNTech trial, two more in the AstraZeneca group (where the placebo was half the size) and Moderna had one more covid death in the placebo group For a whole 6 months of apparent protection you would need to vaccinate 20,000 people to prevent a single death with Pfizer/BioNTech, 15,000 for Moderna and 5,000 for AstraZeneca.
There was nothing notable about all cause deaths in the AstraZeneca and Moderna trials.
It’s worth drawing attention to an anomaly with the deaths in the Pfizer/BioNTech trial. After the data submission cut off it took a median of 3 days for a death in the placebo group to be reported compared to 7 days for a death in the vaccination group. Prior to the cutoff it took a median of 5 days to report a placebo death but for those in the vaccination group the median delay was a full 18 days. That is highly suggestive of a significant bias in what was meant to be a blinded trial. One of those who died in the vaccine group was a 60 year old who was injected on 10th September. He lived alone but someone alerted the police to the fact he was not answering his phone and they found his cold body on 13th September. The death was not filed in the trial reports until 22nd November a week after the cut-off for inclusion in the publication which led to approval. Despite the two month window the filing states, “Autopsy results were not available at the time of this report.”
A 65 year old Texan man in the placebo group was injected with Moderna after he had had his two placebo doses. He contracted covid in the danger window, was in hospital within a week of injection and died 11 days later. His death was recorded as an unvaccinated covid death in the trial results even though the protocol said anyone receiving another covid vaccine would be removed from the trial results.
A further death occurred in another placebo recipient that was attributed to covid pneumonia. However, this participant had HIV that was severe enough that they did not meet the inclusion criteria for the trial.
Pfizer hid at least two sudden cardiac deaths of two trial vaccine recipients. One died on 19th Oct the other on 7th Nov 2020. Both deaths were reported on the day to the trial site well before the 14th November cutoff for inclusion in the submission. They were not disclosed then nor at the 10th December FDA meeting which violated legal requirements.
If we exclude the sudden cardiac deaths there were 12 deaths in each group in the trial a third of which were described as due to covid in the placebo group (even though most did not fit the criteria for that description). However there were eight sudden cardiac deaths in the vaccine group compared to only four in the placebo group.
The number of overall deaths in the Pfizer/BioNTech trial was higher in the group given a vaccine, which had 15 deaths at 6 months, compared to 14 in the placebo group. There were 5 cases of cardiac or respiratory arrest in the group that received the Pfizer/BioNTech vaccine, compared to 2 in the placebo group.
If there was a small risk of increased death due to the vaccine in the period shortly after vaccination then this would be hard to detect in age groups where there were high numbers of background deaths. However, in younger age groups, where there are fewer deaths normally, a signal might be noted (see section 8.10c).
There were large numbers of reported deaths where doctors felt the vaccine was a likely cause. Of the death reports in VAERS in 2021, there were 60% more males which suggests these were not random coincidental deaths which would be as likely in females. Rather, it suggests that the spike induced pathology that caused more males to die of covid also causes more male deaths when injected.
The second half of 2021 saw a large number of footballers and other athletes collapse while playing, with significant numbers dying. There is always a risk that this measurement may have been distorted by how readily such news was being shared. However, an analysis of all collapses and deaths in 2021 alone showed a clear discrepancy in the first and second half of the year. Eleven footballers died in the first half of the year compared to 38 in the second and six had to stop playing compared to 58 respectively. This cannot be explained by fewer games being played in the spring of 2021 since by that point the football game schedule had returned to near pre-pandemic levels. A database recording the reasons footballers missed games showed a doubling in heart-related injuries to footballers stopping them playing in 2021. No such rise was seen in 2020 from covid.
a. Problems with systems for highlighting increased deaths
Relying solely on death certification as a measure of deaths caused by vaccination could lead to circular logic. Until the MHRA announced in April 2021 that rare brain clots could be caused by vaccination, there were no death certificates with a mention of vaccination. Doctors wait for a connection to be reported before including vaccination as a cause on death certificates. If the MHRA also waits for individual doctors to certify deaths before deducing a connection, then the link will never be made. Therefore, additional methods of surveillance should be employed to accurately capture the true number of vaccine-related deaths.
The MHRA has a process for handling Coroners Regulation 28 “Reports To Prevent Future Deaths” which it receives. However, MHRA does not have a process for obtaining copies of Regulation 28 reports where a medicine was cited as the cause of death but where MHRA was not a primary or copy addressee. This lack of proactive investigation and information gathering suggests that MHRA’s safety surveillance process may be incomplete.
The Chief Coroner collects Regulation 28 “Reports to Prevent Future Deaths (RPFDs)” that have included covid vaccination as the cause of death. However, it is the responsibility of individual Coroners to address RPFDs relating to medicines to MHRA, UKHSA or the Dept of Health. The MHRA has not obtained any copies of Regulation 28 reports citing the covid vaccines despite at least two reports having been issued to date, even though the MHRA is, ultimately, responsible for licensing their use.
b. Investigating Deaths
The Royal College of Pathologists conducted a centralised audit of Covid-19 deaths to better understand the pathology, despite the Coronavirus Act severely limiting the number of post-mortems. However, there has been no similar work carried out for deaths following vaccination. I have been contacted many times by people wanting a private post mortem where they have had concerns about a cause of death that has not been investigated. The coroners system does not appear to be receptive to concerns about an unnatural cause of death expressed by relatives only by their doctors. The ONS reported that the current leading cause of death is “Signs, symptoms and ill defined conditions.” As a pathologist, this description strikes me as people whose deaths did not have adequate investigation and where the certifier was not sure of the underlying cause. These people should have had a post mortem.
In contrast, other countries have reported on post-mortems after post vaccination deaths. In Germany, a study of 35 autopsies found 5 deaths caused by the vaccine. A contribution from vaccination could not be excluded in a further 20 deaths. Post-mortem studies have also shown inflammation of the coronary arteries after vaccination, causing death 4 months after the last dose. Furthermore, a separate post-mortem study found vaccine derived spike protein in the heart muscle of a subject who had myocarditis before they died, in the absence of Covid-19 infection. In addition, two US teenagers had died from myocarditis induced by vaccination.
Despite this evidence, the MHRA appears to have made no attempt to obtain post-mortem information, and there are few if any pathology laboratories in the UK that are performing the specialist stains for spike protein used in Germany and the US.
Mr James Royle, Consultant Surgeon told me,
“Because we now understand the pathologic mechanisms that make the Wuhan spike so harmful, I have become very concerned about unprecedented rates of reported possible adverse reactions and deaths following vaccination. This cannot be dismissed simply by the unprecedented number of people vaccinated globally in these campaigns; the rate of adverse reactions is dramatically higher compared to all previous vaccines. I have completed over 20 Yellow Cards for patients of mine, or those I’ve been aware of in my department, who have developed significant (sometimes life-threatening), unprovoked and unusual patterns of venous thrombosis, that I believe could have been related to their recent Covid vaccination. I saw three sequential obvious patterns or waves:
1. Thromboses – pulmonary and abdominal (often multiple, same patient), multiple atypical ischaemic bowel cases
2. Septic- nasty appendicitis in middle age and upwards, gangrenous /perforated cholecystitis, increase in wound collections and infections,
3. Turbo cancers (young age, aggressive unusual recurrences and stage 4 presentations).
Note this is not a lock-down effect as it’s too delayed and in my speciality our referrals didn’t drop during covid. In fact they increased as GPs had no other access route and both diagnoses and operations stayed stable or increased.”
Professor Angus Dalgleish, Consultant Oncologist, is also concerned about aggressive cancers he is seeing in his practice. Overall cancer mortality figures are only slightly above normal levels and much of this could be an effect of lockdown. However, a significant number of unusually aggressive cancers in young people could be hidden in that data. Scotland has seen a rise in cancers of the liver and intrahepatic bile ducts but it is unclear why.
c. Excess Mortality
Any potentially deadly reaction from the vaccine roll-out would be more likely to result in death in the already frail than in the fit and young. However, because the background death rate is much smaller for the young, an increase would be easier to notice among the young. For 15-19 year old males in total there were approximately 100 extra deaths in this age group over the course of the rollout. In females there was no signal.
Deaths that are referred to the coroner are not included in the public health or ONS weekly data and it can take months to years for them to be registered in the data. This is a serious oversight as these are the deaths that are most likely to be preventable.
The ONS reported on the cause of death for those deaths that were registered within this age group. They summarised each death as a single code which is likely to mean that important information will have been lost. There was a 43% rise in suicides over 2019 levels. Four of the 12-15 year olds in the Pfizer children’s trial were hospitalised for suicidal ideation in the vaccine group a rate of 1 in 250 compared to none in the placebo group. There are numerous reports of post vaccine suicidal ideation among children in the US VAERS system.
d. Lack of Deficit
In Spring 2020, there were significant deaths among the old and vulnerable and that would mean that fewer than normal deaths should have been expected in 2021 onwards. It is impossible to say for certain how many should have been expected in these circumstances.
To discuss excess deaths effectively, it’s vital to first comprehend their determination. Essentially, this involves estimating the expected number of deaths. The Organisation for Economic Co-operation and Development (OECD) typically references the 2015-2019 period as a standard for comparison. Similarly, the Government’s Office for Health Improvement and Disparities employs a model based on the same period, adjusted for demographic ageing. I have used this data in my analysis.
However, there is a notable issue with the approach taken by the Office for National Statistics (ONS). Contrary to standard practices, the ONS has incorporated the 2021 mortality data into its baseline for expected deaths. This inclusion is problematic given the atypical nature of deaths in that year. Such a methodology could lead to an understatement of excess deaths by inflating the expected death count.
It is harder to accurately predict what expected deaths should be in winter periods as it is heavily dependent on how many frail there are in the community and which respiratory viruses are circulating. After many deaths, a quiet winter for deaths in the elderly in 2021/22 meant that there appeared to be fewer deaths than expected but this hides a continuing excess of deaths in the young and of cardiac deaths.
Figure 77: All cause excess mortality for all age groups calculated by the Office of Health Improvement and Disparities
England saw a stepwise rise in cardiac deaths after ‘vaccine’ rollout separate from covid waves. This included deaths attributed to ischaemic heart disease. Expected levels are harder to predict in the first months of the year where there is wide annual variation and a mild winter season for viral deaths and low numbers of remaining frail elderly (who account for most deaths) meant the stepwise increase was not evident for a short period. Heart failure deaths show a similar pattern.
Figure 78: UKHSA data showing deaths mentioning ischaemic heart disease, turquoise bars show total excess deaths, pale grey bars above the purple dotted line indicate non-covid excess deaths
Figure 79: UKHSA data showing deaths mentioning heart failure
Here are deaths in the 50-64 year old age group:
Figure 80: UKHSA excess deaths for 50-64 year olds
e. Reasons for excess deaths
The only official statement regarding these excess deaths has come from the CMO, Dr Chris Whitty, in early December, who suggested that the excess deaths were due to heart disease and cancer cases being missed because of the prior Covid-19 lockdowns. This is not supported by independent analysis. For example, there has been no reduction in prescriptions of heart drugs such as statins.
Australia also saw a rise in excess deaths in 2021 before any significant covid deaths. A similar control group is Singapore which also had minimal covid prior to Omicron but saw an excess of cardiovascular deaths from 2021.
A vaccine that caused disease and death could do so both in the immediate period or later on. At an individual level attributing cause with a temporal association is much easier but a latter effect can be evident if viewed at a population wide level. Of the deaths reported as potentially due to ‘vaccination’ in VAERS in 2021, there were 60% more males. This suggests these were not random but caused by spike induced pathology that also caused more males to die of covid.
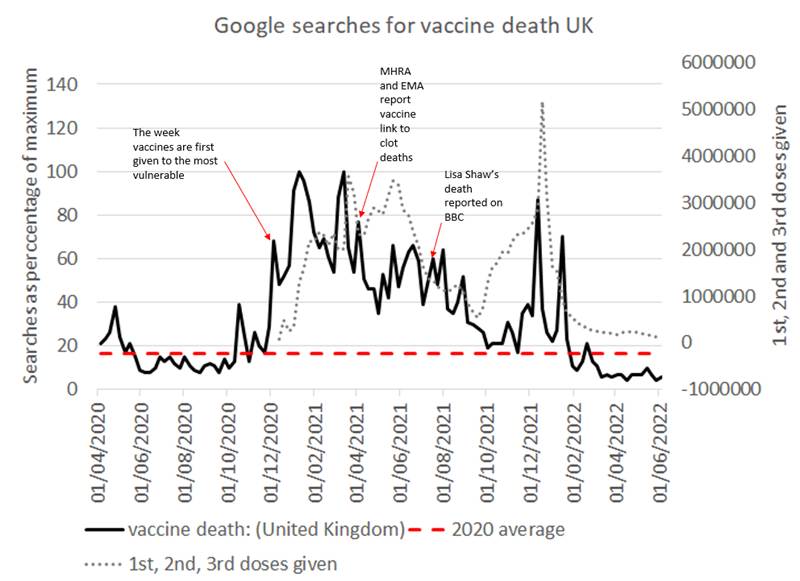
Figure 81: Google search results for “vaccine death” as a percentage of maximum searches in that time period, plotted against vaccine doses given
Finally there have been several studies demonstrating a correlation between ‘vaccination’ rates and covid mortality in 2022 comparing geographical regions. This is particularly damning given the marked socioeconomic differences between the ‘vaccinated’ and ‘unvaccinated’ populations which meant their pre-‘vaccination’ mortality rate was higher.
Given that:
- the timing of the rise in life threatening ambulance calls, increased disabilities and excess mortality which all rose in synchrony from spring 2021;
- the unprecedented reporting of harm thought to be cause by the covid vaccines in the surveillance systems and prospective surveys;
- the similar problems seen in Australia and Singapore prior to any significant covid;
we can reasonably hypothesise that the covid vaccines must be the prime suspect for the rise in excess mortality.
8.11 Immune impacts Original Antigenic Sin and Immune switching
We now have evidence that the more doses given the higher the covid rates. Repeated injections have been shown to switch the immune response into the same mode used to prevent an immune response to food such that the spike protein is ignored entirely increasing the risk of infection.
Figure 82: Covid case rates over time by number of doses given
The immune system is complex and interfering with it can have unexpected outcomes. Firstly, there is a body of work showing that the first time the immune system is introduced to a foreign antigen it will always resort to using the same strategy to attack it when it encounters it again in future regardless of whether the antigen has since mutated. This is known as “original-antigenic sin.” The consequence of it is that everyone who was vaccinated before being infected uses the same strategy to attack the virus which will act as a drive for the virus to mutate to evade this strategy.
Secondly, there have now been a number of papers showing that repeated dosing results in the immune response permanently switching to a “tolerance” response (producing IgG4 antibodies) similar to how our immune system ignores foreign food material. Newborn blood in babies with vaccinated mums has even been shown to have IgG4 antibodies.
Either or both of these factors may have contributed to there being higher case rates among the vaccinated than the unvaccinated since the arrival of Omicron. Lower vaccination rates in East Germany resulted in a clear demarcation of the border when looking at a map of Omicron case rates. Similarly French speaking Belgium had lower vaccination rates than the northern Flemish who had much higher case rates with Omicron.
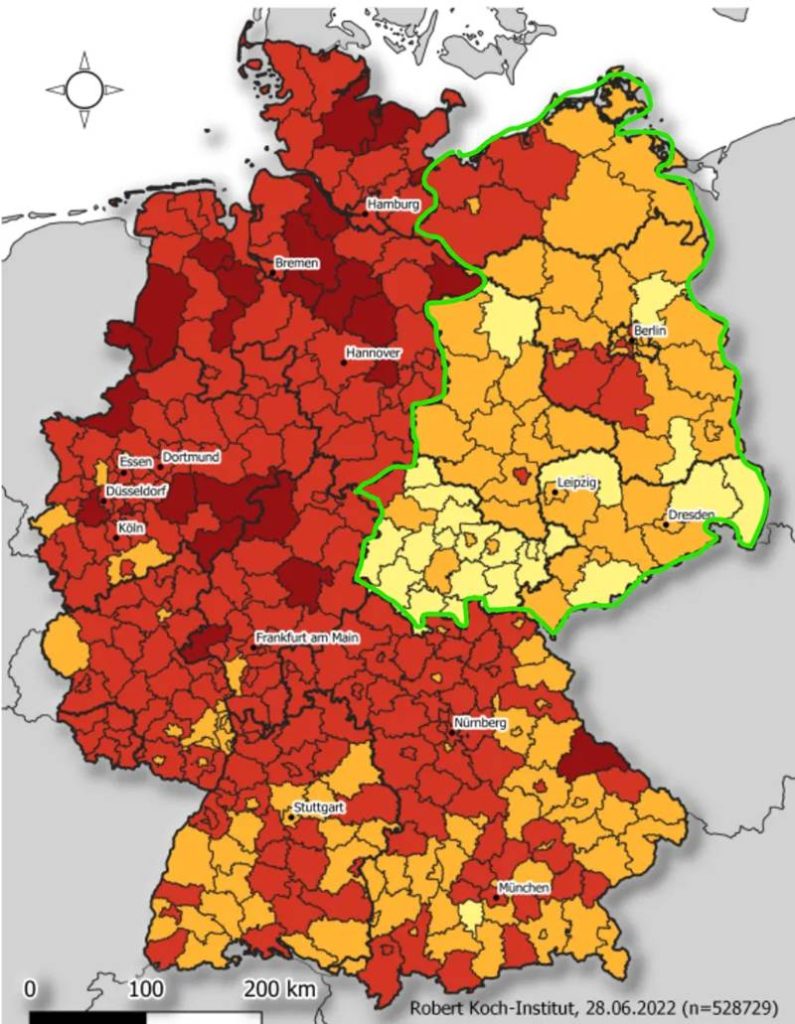
Figure 83: Map of case rates from Omicron in Germany in June 2022
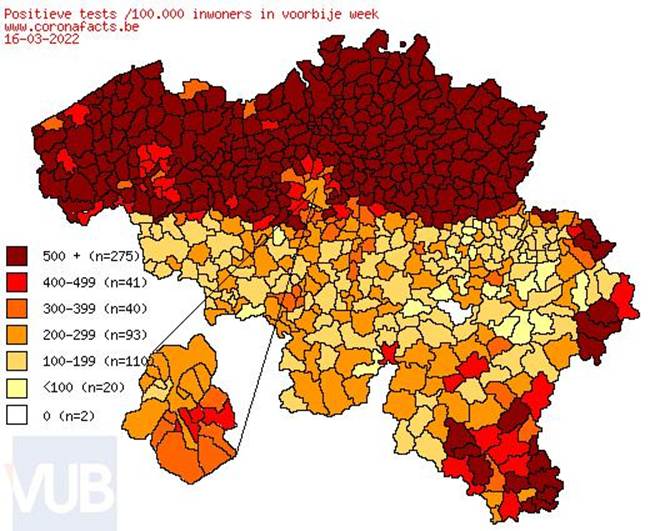
Figure 84: Belgian case rates from Omicron in March 2022
8.12 Fertility
Women had concerns around the impact on fertility given the known accumulation of the lipid nanoparticles in the ovaries of the rat biodistribution study. Government and NHS advice was that “there is no evidence that the vaccines cause infertility” which is not the same as saying they do not cause a problem. Not only were these concerns dismissed out of hand, women wanting fertility treatment in Scotland were refused treatment if they had not had three doses of vaccine.
8.13 Long Covid, or ‘Long-Vaccine’?
Long covid exists but has been potentially exaggerated, distorting public perception of the risk. Post-viral syndromes pre-covid have long been known to cause debilitating effects in some people. Pneumonia patients were often told to expect a six-month recovery period, without a specific label like “long pneumonia.”
Studies on long covid have failed to provide a specific case definition. Instead, a wide range of symptomatology has been included as long covid and the symptoms associated with it have changed over time. These studies have faced issues with sample bias and methodology, possibly leading to overestimation. The risks from long covid after 12 weeks have been exaggerated, and it is, in fact, very rare. Self-diagnosing long COVID led to nearly 2 million people in the UK describing themselves as having long covid by May 2022. More scientific attempts to measure the problem arrived at much smaller numbers.
A Nature paper found 1 in 217 patients experienced fatigue more than 12 weeks after having covid, compared to 1 in 416 patients who did not have covid. There was a small difference in “long covid symptoms” reported more than 12 weeks after a positive test with 5.4% in those recorded as having had covid compared to 4.3% of the control group but they did not control for how frequently the two groups visited their doctor. The authors then compared how frequent particular symptoms were in the covid group and the control group. They did find a six fold higher rate of loss of smell and four fold higher rate of hair loss. These symptoms with large differences between the covid and control group may well have been due to covid. However, they also attributed symptoms with smaller discrepancies between the groups as due to covid including sneezing, ejaculation difficulty and reduced libido. Every single symptom studied in the study was more common in the test positive group. This is highly suggestive of bias either in the sampling or introduced with the many adjustments carried out to the data. The result was a claim that long covid increases the risk of both constipation and diarrhoea and of urinary retention as well as urinary incontinence. When the claim is that a disease causes every symptom it is far more likely to be due to bias selecting a less well population than a real finding.
Exaggeration of the extent of the problem with long covid does not help those who are truly debilitated because of covid, as minor symptoms are sometimes equated with disabling ones in an attempt to exaggerate the extent of the problem.
The Zoe App study found only 1 in 230 covid patients had symptoms after 12 weeks, with 99.6% recovered. The Zoe App study showed a change in long covid symptom types from predominantly respiratory symptoms in those who caught covid prior to vaccination to neurological symptoms after vaccination. 98% of long covid after Delta was seen in the vaccinated.
A French study found a higher incidence of various symptoms among those who believed they had long covid. One way of testing the accuracy of the diagnosis is to see whether the presence of any particular symptom can be used to accurately predict who would test positive for covid antibodies. Only anosmia (loss of sense of smell) had a significant relationship to a positive antibody result. People with other symptoms were as likely to test positive as negative for covid antibodies. People with anxiety, depression, loneliness or stress before covid infection were more likely to report long covid.
Long-term sickness in working-aged people did not rise significantly in the UK or the US throughout 2020. The rate of economically inactive working-aged people due to long-term sickness had been rising among women since the beginning of 2019, plateaued with the arrival of SARS-COV-2 and started to rise again from February 2021. For men, levels remained stable until March 2020, with a more extensive rise from May 2021. A similar rise in disabilities is evident in US data (see section 8.7). The cause of these rises in 2021 has not been determined. The lack of rise in long-term sickness until spring 2021 suggests that long covid from the first year of circulation did not exceed levels of post-viral illness seen in previous years.
The Zoe App study did not find any reduction in the duration or prevalence of long covid symptoms in vaccinated individuals. The Zoe App study did not analyse the role of vaccination in long covid development. The rise in long term sickness absence from spring 2021 coincides with the rollout of covid vaccines to the working-aged population, suggesting a possible connection to vaccine side effects. It is crucial to investigate the relationship between long covid, vaccine side effects, and other factors to ensure accurate understanding and appropriate public health measures.
UKHSA (and previously PHE) use Google Search data as a tool for tracking public health. Google search data from the UK shows a strong correlation between vaccine doses and searches for “vaccine side effects” and specific adverse events, such as “myocarditis,” “pericarditis,” and “vaccine death.” Searches for “long covid” increased with the rollout of the third vaccine dose. There is a tight correlation between Google searches for ‘long covid’ and third vaccine doses given, which is stronger than the correlation between searches for ‘long covid’ and covid case numbers.
Figure 85: Google search results for “long covid” as a percentage of maximum searches in that time period, plotted against vaccine doses given
A Swedish study on long covid study took 580,000 people and compared long covid from those infected in spring 2020 (when only the very sick were diagnosed with covid because of minimal community testing) and compared the rates of long covid with people who were vaccinated and infected with the milder Omicron variant. Using this distorted methodology they claimed vaccines prevented long covid.
An Indian study showed a doubling of the risk of long covid after two doses of vaccine.
The pre-Omicron, pre-vaccine rate of long covid symptoms was 14.5% at 4 weeks and fell to 2.2% at 12 weeks according to the King’s College ZoeApp researchers. They excluded people who were already unhealthy prior to their infection.
An Australian study done pre-vaccine estimated a 5% rate of long covid at 12 weeks. They did not account for people who were symptomatic before having covid and remarked, “Those with more comorbidities were also less likely to recover than those with fewer.” However, in an Australian population, exposed to the milder Omicron variant, where 94% had had three or more doses the rate of long covid, the rate was 18% at 12 weeks. Even when only counting those with no pre-existing health issues the figure was still 16%. Although the research was carried out by survey, they did not ask people their vaccination status. Instead they relied on links to “vaccination information collected as part of the initial COVID-19 disease notification and case investigation process.” This allowed for miscategorization and a false conclusion that the unvaccinated were at higher risk.
Ultimately it is the total disability data (see section 8.6) that allows conclusions to be drawn. Yes there were people with a post viral condition after covid which occurred at the same rate as previous post viral conditions and did not impact overall on numbers in the working aged population able to work. After vaccination these numbers rocketed. Even if the problem occurred after infection, it is still a problem with the vaccine if the same person would not have had long covid if they had not been vaccinated.
9. TREATMENTS
| Basic principles of ethical treatment and of how evidence should be prioritised in different situations was disregarded. Usual care was altered with detrimental impact. Treatments with a known safety record were discredited by using toxic doses in trials and through smear campaigns. In the meantime, the standard of evidence required for profit making drugs was far lower than for generic medicines. |
9.1 Principles
When assessing the potential value of a medical intervention, it is crucial to weigh the benefits against any known or potential unknown risks. In situations where there is a substantial possibility for benefits, such as when a patient is already ill, the acceptable risk threshold may be higher, particularly if their condition is life-threatening. In these cases, the required evidence of benefit can be lower. On the other hand, when a patient has minimal chance of benefit, the tolerable risk level is significantly lower, and the proof of a drug’s safety and efficacy must be correspondingly stronger. This principle was inverted for covid.
For example, an over 80-year-old with symptomatic covid had a mortality rate of 5%, for someone with severe disease it would be higher, add in co-morbidities and the risk could be doubled. In such circumstances, there should be no hesitation in prescribing a drug with an established safety record that might reduce mortality.
This was the approach taken with MERS. Taking of existing drugs Anthony Fauci said, “We don’t have to start designing new drugs…. If I were a physician in a hospital and someone were dying, rather than do nothing, you can see if these work.”
Although SARS-CoV-2 had some novel features it was still a coronavirus and still caused an acute respiratory tract infection. There was a body of knowledge for how to treat acute respiratory tract infections and pneumonias that was disregarded. There was also evidence that certain treatments had been efficacious for SARS1 but this was also disregarded.
One strategy would have been to start with a baseline of standard viral pneumonia treatment and then investigate what did or did not work within that regime or in addition to it. Instead, the baseline was to not treat at all.
Demanding proof of benefits in randomised clinical trials ensures safety and efficacy but it disregards the urgency of emergency situations, leading to delays or prevention of a rational response to emerging evidence.
9.2 Changes to Protocols
It is imperative that doctors have the freedom to do what they believe is best for the patient in front of them. Medicine has for several decades been increasingly controlled through creating protocol-driven guidelines which restrict what doctors can offer to patients. Although doctors have the ability to deviate from guidelines, they must be able to provide evidence to defend their decision to do so and it is far easier for them to simply follow the guidelines. The guidelines often do not have named authors and are not open to debate or discussion. The consequence is medicine being practised by nameless bureaucrats, or politicians including those with no medical qualifications, who have had no contact with the individual patient.
Doctors were given protocols that excluded usual therapies for viral pneumonia and only included treatments where there was evidence of benefit demonstrated in randomised clinical trials. Having this high standard ensures that patients are not inadvertently being harmed and that money is not wasted on ineffective drugs. However, the time frame for gathering such evidence is not compatible with providing the best treatment for patients who are dying while waiting for a protocol change. The standard of evidence required to make a recommendation should be dramatically reduced in an emergency allowing for advice to change as more evidence emerges. The default of not treating is not good for patients.
Discussion of treatment of Covid-19 is meaningless without considering the typical clinical course of the disease. In early-stage infections, symptoms are similar to many other upper respiratory tract infections, and may resolve without interventions. There are then two distinct phases of illness: the viraemic phase, where virus enters the blood and is still replicating and the later inflammatory phase associated with lung inflammation.
The official response fixated on finding a ‘magic bullet’ to cure all stages of the illness. This approach overlooked the complexity of the disease and the demonstrated efficacy of multi-drug therapies, including antivirals and vitamins.
With a disproportionate emphasis on treating advanced, hospitalised cases, the importance of early intervention was underestimated, causing the adopted strategy to fall short of its aims.
Early-stage viraemic infections are treatable with many antiviral agents. The Sequential Multi-Drug Therapy approach of McCullough advocated use of dual antivirals, depending on availability in the locale, along with multiple vitamins (especially large doses of Vitamins C and D3 and zinc).
In those patients later developing inflammatory reactions (typically from Day 8 of symptoms onwards) with lung inflammation leading to reduced blood oxygen saturation, the primary clinical need is to control inflammation. Virus levels are low by this stage. In early 2020, the only treatment offered in most Western countries was supportive care plus low-flow medical oxygen or in severe cases the use of mechanical ventilation. The obvious use of corticosteroids in the inflammatory stages (which are used for other pneumonia and reduce inflammation) was considered controversial until the reporting of the dexamethasone arm of the RECOVERY trial made them a standard of care. Prior to this the FLCCC group of US intensive care specialists had been using methylprednisolone (a corticosteroid) in significantly larger equivalent doses (in their “MATH+” protocol) for much longer. Later Dr Shankara Chetty in South Africa developed his “Eighth Day” therapy in open air clinics requiring intervention only if symptoms had not resolved by Day 8, when prompt treatment with antihistamines and antileukotrienes effectively removed, in his experience, any need for medical oxygen.
Contrasted with these widespread empirical reports of success by clinicians often working in crisis situations, the response of the NHS and DHSC paralleled many Western medical bureaucracies in denying that any treatments existed, in defiance of the empirical evidence. In particular the utility of repurposed medicines of well-known safety profiles was denied, or even the utility of anti-inflammatory medications to control inflammation.
9.3 Finding a treatment
The other aspect of the official response was the futile search for a single “magic bullet” when all of the empirically successful treatments involved use of multiple medications, and for a single treatment that would work at all stages of a complex clinical course varying from a mild cold to hypoxic respiratory failure. Although almost self-evidently absurd, this strategy continued without abatement. There are no grounds for supposing that any single drug could successfully treat both a mild viral infection and severe covid pneumonia. There was continued emphasis on late-stage hospitalised disease, when successful clinicians emphasised prompt treatment of the mild viraemic phase, with the objective of preventing hospitalisation in the first place.
9.4 Antibiotics
New healthcare protocols in spring 2020 resulted in significant alterations to the standard treatment approach for pneumonia. Previously, antibiotics were administered to patients presenting with pneumonia regardless of the exact cause. These could combat possible secondary or incipient bacterial infections and may have direct anti-inflammatory effects too. Covid protocols resulted in patients being told to self-care unless they needed urgent hospital admission and a positive test often precluded the use of antibiotics, except in vulnerable individuals. Effectively, standard treatment was withdrawn.
Prior to spring 2020, a patient presenting in the community with pneumonia would have been treated with antibiotics. The doctor may never know the underlying cause but in a viral pneumonia, although any antibiotics will not kill the virus they may help treat an incipient or prevent a secondary bacterial infection, and may have direct anti-inflammatory effects too. The change from normal practice for treating community acquired pneumonias was driven entirely by NHS protocols. Instead of seeing patients face to face and treating as a community pneumonia, the protocol gave a choice between “self isolate / self care” and “urgent hospital admission.” The NHS protocol referred to NICE guidelines which changed the usual routine of offering antibiotics depending on the severity of illness to saying that a positive test result would mean antibiotics should not be given except in the vulnerable.
Covid patients with more than one bacterial infection had only a 20 percent survival whereas those with only a viral infection had an 80 percent survival.
9.5 Morphine and Midazolam
The use of end-of-life medications, such as morphine and midazolam, has also drawn attention and criticism. Both these drugs reduce the respiratory drive. During an acute respiratory infection that respiratory drive can be lifesaving, even if it is distressing to the patient and those around them. A number of relatives have distressing stories of patients dying after being given midazolam and morphine. These drugs do not reduce the time to death in palliative care situations. However, it is not clear that this finding can be extrapolated to their use in acute respiratory tract infections where respiratory drive is an essential indicator of survival.
Protocols recommended giving these drugs to those with moderate to severe breathlessness, regardless of concerns about respiratory depression. It’s speculated that fear-induced messaging during the pandemic, giving a false impression of the chance of survival in the elderly, might have led to a low threshold for placing patients on end-of-life care, potentially hastening their demise.
A group of consultants, including in palliative care, wrote an open letter in the BMJ in May 2020 criticising the use of end of life pathways for patients who were more likely than not to survive if there were no such intervention. They said, “uncritical use of NG163 may create unintended risks for people with suspected or actual COVID-19 infection.”
NICE guidelines issued on 3rd April 2020, say,
- “Consider an opioid and benzodiazepine combination for patients with COVID-19 who:
- are at the end of life and
- have moderate to severe breathlessness and
- are distressed.”
- “Sedation and opioid use should not be withheld because of a fear of causing respiratory depression. Dosages may need to be adjusted because some patients dying of COVID-19 may need higher doses to achieve symptom relief. Others may need lower doses because of their size or frailty”
- “When managing key symptoms of COVID-19 in the last hours and days of life, follow the relevant parts of NICE guidelines on care of dying adults in the last days of life. This includes pharmacological interventions and anticipatory prescribing. Note that symptoms can change, and patients can deteriorate rapidly in a few hours or less.”
Furthermore, some have argued that the rise in midazolam usage is exactly what you would expect when a large number of people are in respiratory distress during a covid wave. Guidelines were issued in March from the Association for Palliative Medicine that recommended Midazolam with a range up to three times the usual dose for patients in severe respiratory distress. However, subsequent analysis of doses needed by patients dying of COVID-19 has shown that they did not require higher doses than those used for other respiratory conditions. Dosages of Midazolam were in fact given at a dosage level similar to pre-covid levels in some areas, rather than at these higher dosages.
There is an argument that these drugs were prescribed to more patients because of increasing demand for end-of-life care, because of covid. There was a marked increase in prescribing for midazolam and morphine in the lead up to the first lockdown. Doctors were making sure their patients, some of whom were frail and might need palliative care during the lockdown, had the drugs at hand in case they were needed. It is not clear how many of these prescriptions were given to the patients.
However, a significant increase in midazolam prescriptions was observed during the first covid wave in London, but not during the second, despite a larger wave. The reason for this disparity is unclear, but suggests it was not needed for covid treatment.
Figure 86: Prescriptions given for Midazolam by region. The blue line at the bottom is London
There are two situations where Midazolam may have been overprescribed. Firstly, during lockdown in care homes there was significant understaffing and using Midazolam could have been a tempting way to stop dementia patients from wandering and being difficult to care for. Secondly, Midazolam does work well to reduce respiratory distress. A patient who is struggling for breath can apparently be cured of that symptom using this drug and this would also reduce the distress of the neighbouring patients and staff as well as making the staff feel like they had helped. However, when battling an acute respiratory tract infection, effortful breathing can be exactly what is needed to ensure that respiration is inadequate. Dampening that response could be detrimental, including in patients who were not necessarily destined to die, as recoveries from infection, especially when aggressively treated, can often be rapid and unexpected.
It is unclear how many patients had face-to-face reviews with a doctor prior to the medications being given nor how many of the patients may have had reversible causes of deterioration (unrelated to covid) who did not get to hospital or were not seen by a doctor. Multiple witnesses at the Scottish Covid Inquiry have testified that they believe their loved ones died from inappropriate end of life medications and their deaths were attributed to covid.
The potential misuse of midazolam and the impact on patients who might have had reversible causes of deterioration warrant urgent investigation. Given the discrepancies in prescription practices and the serious accusations from multiple relatives and whistleblowers, there is a need to rationally ascertain the facts and see if lessons need to be learnt.
9.6 Hydroxychloroquine
Hydroxychloroquine is a well-established safe drug used to treat autoimmune conditions and for centuries as an antimalarial safe enough for use even in pregnancy. The effect of chloroquine on SARS-1 infection (including potential prophylaxis) in animal studies was known since 2005 in the peer-reviewed literature. The researchers described how, “concentrations of 10 μM completely abolished SARS-CoV infection.” They concluded, “These inhibitory effects are observed when the cells are treated with the drug either before or after exposure to the virus, suggesting both prophylactic and therapeutic advantage.”
The safety profile had been established over decades of pharmacovigilance. Nevertheless the use of either form of the drug in covid treatment was declared controversial, with warnings from the DHSC that HCQ should only be used in the context of clinical trials. NICE does not even mention it.
Very early reports (March 2020) from the IHU (University Hospital) Méditerranée Infection in Marseille demonstrated successful treatment of early-stage infections with a hydroxychloroquine-azithromycin combination, later expanded into reported case series covering many thousands of patients. With the addition of zinc supplements, known since 2010 to poison the RdRp enzyme (or “replicase”) of a wide class of RNA viruses, Dr Vladimir Zelenko reported his “triple therapy” of hydroxychloroquine-azithromycin-zinc in open letters from mid-March 2020, later (summer 2020) publishing his case series with an external control group.
Hydroxychloroquine was issued as a prophylactic to health-care workers in India from March 2020 onwards. All these widespread empirical reports came in the “first wave” of infections in Spring 2020.
In late March 2020, Donald Trump enthusiastically suggested hydroxychloroquine was “one of the biggest game changers in the history of medicine,” after which its use became heavily politicised with opponents determined to find evidence he was wrong. This created a negative bias in reporting on the drug from then onwards.
One of the most highly influential research papers of the Covid-19 pandemic was published in the Lancet in May 2020 effectively ending many active clinical trials and changing national and international policies, when the claimed results from a 96,000 patient database apparently showed that hydroxychloroquine actually increased mortality and heart arrhythmias. Notoriously however, this paper was retracted after only a fortnight when the results were shown to be fabricated. The number of deaths that supposedly occurred in just five Australian hospitals was greater than the number of deaths that existed in the entire country at the time. The Guardian exposed how the paper was written by a company called Sugrisphere whose chief executive was investigated for three counts of medical malpractice. It was established as a publisher of medical textbooks in 2008 and claimed to have 11 employees all recruited within the preceding two months which “appear to include a sci-fi writer and adult content model.” Nevertheless, the policy shifts triggered by the publication of an obvious fraud were not reversed. There does not seem to have been an investigation into the funders of Sugrisphere nor prosecutions for the fraud.
On the basis of this fraudulent study the MHRA instructed the PRINCIPLE trial to pause recruiting for the hydroxychloroquine arm of their trial on 27th May 2020. The WHO also paused their SOLIDARITY trial.
A study from Brazil, used not hydroxychloroquine but its close cousin chloroquine. Chloroquine is used to treat people dying from malaria at a maximum dose of 1.75g over the full course for a 70kg man. Half the people in this study were given 12g of the drug and the other half were given a “low dose” of 2.7g. These doses were given to sick people, one third of whom fitted the criteria for having a 33% 30 day mortality rate. In addition, “Most patients (89.6%) in our study were also receiving oseltamivir for suspected influenza infection, which also increases QTc interval and could have adverse cardiac effects.” Oseltamivir is also known as Tamiflu and is manufactured by Gilead, the manufacturers of Remdesivir. The mortality rate in the treatment group was twice as high as the control group.
Patients were being treated with hydroxychloroquine at reasonable doses in Switzerland but on publication of the Lancet paper hydroxychloroquine treatment was suspended. Deaths had been hovering around 5% of the disproportionately hospitalised cases since April but thirteen days after hydroxychloroquine was suspended they jumped to over 12%. Once the fraud was exposed, usage restarted and deaths fell again to around 5% after a further 13 day lag.
In June 2020, the UK, the Oxford “RECOVERY” trial reported apparently poor results from the hydroxychloroquine arm of that platform trial. However, the trial dealt only with hospitalised patients already in the inflammatory stage of the illness (median time from symptoms 9 days), was confined to the use of hydroxychloroquine as a monotherapy, when all empirical reports of success used the drug in combinations, and the dosing schedule for the drug involved extremely high doses (approaching 50% of reported lethal doses in the first 24 hours of treatment). The dosing schedule has been harshly criticised in exchanges in the New England Journal of Medicine and elsewhere and essentially remains unexplained. The important points in the UK context are that a trial widely reported as having shown “hydroxychloroquine doesn’t work” showed nothing of the kind, involving highly toxic doses advocated nowhere by any clinicians using the drug with success, delayed treatment until well past the viraemic stage, and neglect of all prior empirical reports of effective combinations, in particular with the critical adjunct of zinc supplements.
On 16th June 2020 the MHRA instructed clinical trials on hydroxychloroquine to stop recruitment. They referenced only two trials in their decision making, the RECOVERY trial and a US trial of only 821 asymptomatic people who had been exposed to a contact in which there were only 16 laboratory confirmed covid cases spread across the treatment and placebo groups. A quarter of them were not enrolled until 4 days after exposure and yet there was no mention of excluding those who developed symptoms before starting on hydroxychloroquine prophylaxis.
By summer 2020, advocates such as Prof Harvey Risch of Yale were pointing out that early outpatient treatment was key to the control of the pandemic crisis, and concentrated on hydroxychloroquine combinations. The evidence to support these claims was clear by mid-2020, along with the Sequential Multi-Drug Therapy approach of McCullough (which used hydroxychloroquine as one of the leading candidate antivirals).
A meta-analysis of 30 randomised controlled trials showed a 29% improvement in either recovery time or hospitalisations or deaths. When focused on early treatment the figure rose to 49%. When removing the late treatment trials, there was only one trial out of thirteen that did not show a benefit. Papers published in the USA showed a bias towards negative results.
One US study sponsored by Anthony Fauci’s department, NIAID, set out to recruit 2,000 patients in an early treatment trial testing hydroxychloroquine and the antibiotic azithromycin with 24 weeks follow up. Only 20 people were enrolled and only 16 were given either drug or placebo and none were followed up beyond day 20.
The significant points regarding hydroxychloroquine are that combination therapies are essential, especially including zinc, toxic doses are absolutely not necessary, but efficacy cannot be expected if treatment is delayed until the florid hospitalised stage of disease is reached.
As late as January 2024, a claim was made that hydroxychloroquine use had resulted in the death of 17,000 people with covid. The study referenced a meta-analysis based largely on the toxic doses given in the RECOVERY trial which was written by authors dependent on grants from Gilead and Pfizer as well as other pharmaceutical companies and claimed an 11% increased mortality rate. The trials studied when the data was combined had 14% deaths in the hydroxychloroquine group and 17% in the control group yet after weighting they claimed an 11% higher mortality in the hydroxychloroquine group. The 17,000 figure was reached using modelling. The authors said “We calculated the number of deaths in hospitalised patients by multiplying the number of hospitalised patients receiving HCQ by the mortality rate of each country.” These papers are both entirely dependent on the errors in the RECOVERY trial for their conclusions.
9.7 Remdesivir
Remdesivir was an antiviral drug owned by Gilead Sciences, looking for a virus it could treat. Fauci was responsible for spending $34 million of US taxpayers’ money to develop remdesivir as a treatment for Ebola. A 2019 Ebola trial in Africa ended early because monoclonal antibody treatments were so much better than remdesivir. Notably, the people who died from Ebola died within 10 days but those on Remdesivir saw a second wave of deaths after this period and were still dying up to 22 days later.
Seeking a new market for a failed product, Remdesivir was then tested for covid, consistent with the bureaucratic desire for the “single magic bullet”. As with hydroxychloroquine, the importance of disease stage was ignored, not least because it cannot be given orally, and requires intravenous infusion in a hospital setting. However, there remains no reason to suppose that any antiviral would be effective in the inflammatory disease stages after the virus levels plummet.
Fauci then invested a further $36 million of government money to test it for covid, announcing the trial before a ‘pandemic’ was declared. The starting point of the trial was biased with the placebo group having older patients. They were also sicker. Before treatment began, 24 percent of the remdesivir group were on invasive ventilation compared to 30 percent of the placebo group. The original aim was to recruit 394 people to measure a reduction in covid severity, hospitalisation and death but the goalposts were shifted during the trial with the final endpoint being shorter hospital stays. They repeatedly increased the number of people ending up with 1062 participants at which point they managed to claim a reduction in length of hospital stay from 15 days to 11 days. Worryingly, more of the remdesivir patients had to be readmitted after discharge. A higher readmission rate suggests that there may have been a bias between the groups that would have affected the measure of length of hospital stay. This was a flawed trial.
A Lancet paper, published on 29th April 2020, showed that Remdesivir did not reduce hospitalisations or deaths and caused injury to every fourteenth person who took it.
On 29th April 2020, Dr Fauci declared remdesivir the standard of care for COVID-19 via a press conference, meaning any doctor not giving it would need a good case to defend that position.
A comment in the BMJ said on 26th May 2020 “the early adoption of Remdesivir was a triumph of hope, and probably marketing, over data.”
On 26th May 2020, it was announced that NHS patients would soon be treated with Remdesivir. It was made available until 3rd July 2020 through the “Early Access to Medicines Scheme” which allowed for “promising new unlicensed medicines and medicines used outside their licence, to UK patients that have a high unmet clinical need. The medicinal products included in the scheme are those that are intended to treat, diagnose or prevent seriously debilitating or life-threatening conditions where there are no adequate treatment options.”
On 3rd July 2020, an EMA Conditional Marketing Authorisation allowed for “an interim clinical commissioning policy [to be] put in place to define routine access to remdesivir in the treatment of COVID-19 across the UK.” It was recommended for hospitalised covid patients over the age of 12.
In July 2020, the Australian patient information leaflet noted that rats and monkeys given Remdesivir “severe renal toxicity occurred after short treatment durations.”
On 8th October 2020 the EU signed a $1.2bn procurement agreement with Gilead for 6 months supply of Remdesivir.
The WHO Solidarity trial, which was ten times larger than Fauci’s trial, published interim results on 15th October 2020 and showed no reduction in ventilation, death or length of stay after which they issued a recommendation against its use.
Because of this concern the EU proposed several safety trials in 2022. These showed “a spectrum of degenerative, necrotic and regenerative changes” in kidneys of rats given 3mg/kg/day and “adverse kidney changes…observed at ≥ 5 mg/kg/day, with mortality noted in 1 animal administered 20 mg/kg/day.” The human dosing schedule (including for children under 40kg) is to give 5mg/kg/day for the first day and then 2.5mg/kg/day. The EMA concluded “the available clinical data do not suggest a confirmed renal safety signal” and prescribing continues.
In an individual patient, kidney failure can be thought to be due to covid itself hiding the impact of the drug.
The manufacturer, Gilead, ran a phase 3 trial in covid patients who had renal impairment and recruited 163 to receive the drug. They reported that, “The study closed prematurely due to feasibility issues and was underpowered to assess for efficacy because of lower-than-expected enrollment.”
Later clinical trials (such as the French DISCOVERY trial in February 2022) concluded “no clinical benefit”.
In early 2024, the NHS was still recommending the use of remdesivir in hospitalised over 12 year olds quoting only the Fauci paper to support that decision.
It cost $10 to manufacture but Gilead charged over $2,300 per treatment. In 2021 the manufacturer, Gilead made $5.6 billion in Remdesivir sales, up from $2.8 billion in 2020 and $3.9 billion in 2022. The cost per Quality Adjusted Life Year was calculated at $1,847,000 for mild covid and $298,200 for moderate or severe covid. For comparison the National Institute for Clinical Excellence said in 2012 “interventions with an incremental cost-effectiveness ratio of less than £20,000 per QALY gained are considered to be cost effective.” In 2020 the government said, “the cost per QALY threshold by NICE for England and Wales is between £20,000 and £30,000.” The cost of Remdesivir is ten times the upper end for what is considered cost effective treatment in the NHS even if the results of the trials are believed.
The continued use in the NHS of an ineffective, toxic drug of very high cost constitutes a serious failure of clinical management and regulatory control. With a mechanism of action that could only be expected to be effective in early stage disease on an outpatient basis, its use in late stage disease in the hospital context is unlikely to result in a favourable risk benefit ratio.
The Inquiry might seek data on the number of deaths involving renal failure over the last ten years and the proportion of those people who were treated with Remdesivir.
9.8 Budesonide
Budesonide is a steroid in widespread use by asthmatics and has been associated with lower hospitalisation rates, as demonstrated again by practising clinicians in crisis situations.
The STOIC trial in Oxford demonstrated a 90% reduction in hospitalizations for patients given Budesonide within 7 days of symptom onset. The PRINCIPLE trial, also in Oxford, included Budesonide but was limited to high-risk patients who had been sick for up to 14 days; the results were less dramatic, showing a shorter illness and slight reduction in hospitalisation.
The NHS added Budesonide to the drugs GPs could prescribe for high-risk patients in June 2021 but excluded hospitalised patients; it was removed in December 2021, with the recommendation that it should only be used in a trial, without apparent grounds.
9.9 Ivermectin
Ivermectin is a semi-synthetic derivative of a bacterial fermentation product from Streptomyces Avermitilis discovered by Prof Satoshi Ōmura in soil samples from a Japanese golf course. Its anti-parasitic properties were discovered and developed in collaboration with Merck. The drug has been used in literally billions of doses in WHO-sponsored mass treatment of entire healthy populations for the elimination of onchocerciasis (“river blindness” caused by infestations of the parasite Onchocerca volvulus) in the topics. The 2015 Nobel Prize was awarded to Ōmura and Campbell for its success in onchocerciasis and other neglected tropical diseases such as lymphatic filariasis (elephantiasis). Merck (absurdly) claimed serious concerns over safety when it was proposed as a treatment for covid.
Initially a veterinary product, it was licensed for human use in the early 1980’s and has a wholly exceptional safety profile in the WHO Vigiaccess database. The safety profile in particular has been endorsed by none other than Prof Chris Whitty, in a 2010 paper on its use in humans to kill malarial mosquitoes, noting its demonstrated safety at up to 10 times the approved parasitic dosage. Anti-parasitic doses are up to 200 micrograms per kg of body weight, corresponding to 15 mg for a typical 75 kg adult. In Covid-19, doses up to 3 times this for several days continuously have been used.
Ivermectin’s anti-viral properties against a wide range of RNA and some DNA viruses were noted well before Covid-19. The possible use in Covid-19 was triggered by an April 2020 paper from Monash University, demonstrating specific action against SARS-CoV-2 in vitro in a cell culture of African Green Monkey kidney cells. This prompted many urgent clinical trials, largely physician-driven, and in developing countries. Mechanisms of action remain controversial, not least because of the large number of candidate mechanisms, some with specific in vitro or in silico support. These include inhibition of infection by competitive binding to the viral spike protein, inhibiting replication by interfering with viral non-structural proteins such as the RdRp (replicase) or chymotrypsin-like proteases, and host-directed mechanisms inhibiting nuclear import of viral proteins which in infection inhibit interferon signalling, part of the normal immune function which is enabled to operate once more with treatment by ivermectin. Direct anti-inflammatory effects are also reported, and recently a direct in vitro demonstration of inhibiting and reversing the known thrombogenic properties of the viral spike protein has been published. This explains the dramatic effect of rapid recoveries in blood oxygen levels seen in late-stage hypoxic Covid-19 patients, by several groups independently.
Ivermectin is possibly unique among repurposed drugs for Covid-19 in that it has demonstrated efficacy at multiple disease stages, from prophylaxis (where the data is very consistent and shows a more than 85% reduction in infections, culminating in a recent double-blind RCT published in summary form by Medincell) through to late-stage inflammatory illness. It is therefore closest to the “bureaucrat’s ideal” of a single medicine for a single disease, although no clinician would advocate its sole use except possibly as a prophylactic.
Ivermectin was noted and advocated by August 2020 by Prof Thomas Borody in Sydney, a leading gastroenterologist who developed the first triple therapy for cure of bleeding peptic ulcers caused by Helicobacter pylori. Professor Borody announced his “triple therapy” of ivermectin, doxycycline and zinc for Covid-19 in August 2020 and advocated its use in Australia. By November 2020, Dr. Pierre Kory of the FLCCC made now-famous testimony to the US Senate appealing for urgent consideration of ivermectin. The FLCCC group circulated a paper scheduled for publication in Frontiers in Pharmacology. After successful peer review and acceptance this paper was withdrawn by the journal and eventually published elsewhere. A courtesy copy is known to have been passed to Sir Jeremy Farrar (former head of the Wellcome Trust and member of SAGE) on 18 November 2020, who forwarded it to Professor Peter Horby of Oxford (also a member of SAGE), without outcome.
Dr. Tess Lawrie of the Evidence-Based Medicine Consultancy Ltd in Bath responded to the Kory testimony and paper by conducting an urgent meta-analysis of the data and reports in Kory’s narrative review article. These were circulated to the Prime Minister, the Secretary of State and various Government agencies in the UK and overseas. The latest version of the meta-analysis was published in June 2021 and has become one of the most-read scientific publications of recent years, reaching #9 out of over 23 million research papers tracked by the data science company Altmetric, since its inception. In publications of a similar age, it is number two out of over 440,000 publications. No Government department has responded to it, despite it being widely circulated via Members of Parliament, and based on an all-British author team with no conflicts of interest. Based on the meta-analysis of data as at Spring 2021 the cumulative evidence suggested a significant reduction in COVID-19 mortality, based wholly upon randomised controlled trials (RCTs). The other significant finding is the efficacy in prophylaxis.
The World Health Organization (WHO) and other health institutions have shown resistance to accepting ivermectin as a treatment option. The WHO’s own meta-analysis reported a 75% reduction in mortality risk and yet they failed to recommend the use of a very safe drug that has been on the WHO Essential Medicines list for decades.
Pierre Kory pointed out that the studies that swung these reviews against Ivermectin, had authors who all had conflicts of interests, did not give the drug until very late in the illness, underdosed and one trial even changed the point at which outcomes were measured from 14 days to 28 days after symptom onset, at which point people were all either dead or well regardless of which treatment they had had. In the UK a NICE review of ivermectin in November 2021 violated its own terms of reference (which regard meta-analyses of RCTs as the priority for drug evaluations) in deliberately disregarding the Bryant et al. meta-analysis without comment.
Dr Andrew Hill, initially a collaborator with Dr Tess Lawrie, expressed great enthusiasm for the use of ivermectin in treating COVID-19. He was asked to conduct a review of ivermectin for the WHO and pre-empted the proposed systematic review by publishing a preprint of his review. Although the review showcased significant success in numerous clinical trials, it recommended further trials before they were “ready for review by regulatory authorities.” A film documents the interview between Hill and Lawrie, in which Hill confesses that his sponsor (Unitaid) influences the paper’s conclusions. A stylistic analysis of various text versions suggests the involvement of two unnamed contributors.
Internationally, country-scale case studies have demonstrated the success of ivermectin treatment in Peru, with striking results when policies changed abruptly. The Delta wave in India displayed stark differences in COVID-19 death data between Uttar Pradesh, which used ivermectin, and Kerala and Tamil Nadu, which did not. The success of ivermectin in the elimination of Covid-19 from the state of Uttar Pradesh has been widely suppressed, although it is clear that the mass distribution of “Covid Kits” containing the ivermectin-doxycycline-zinc combination advocated by Prof Borody was instrumental in that success.
The fundamental obstacle to ivermectin use in the UK is supply. Ivermectin is licensed for human oral use by the FDA in the USA, but has never been licensed by the MHRA in the UK, and there is no UK manufacturer. All ivermectin is imported, and can be sold at huge markups, although the production cost is negligible and the prices in India are the equivalent of a few pence per pill. Unlike hydroxychloroquine, therefore, clinicians are not easily able to prescribe ivermectin although they would have the freedom to use hydroxychloroquine off-label.
The effectiveness of ivermectin as a prophylactic has been clear from the early reports and confirmed in the latest ones. SIAVE was a double-blind RCT of oral ivermectin prophylaxis in contacts of confirmed cases. Contacts were given daily oral ivermectin or placebo and the ivermectin group had 72% fewer recorded positive test results. The clear efficacy is therefore a direct threat to the market and policy for vaccines. Whilst it is now admitted that the Covid-19 “vaccines” do not protect against infection, prophylaxis with ivermectin does. The results in randomised trials showed by Autumn 2020 that ivermectin was an effective prophylactic in contacts of confirmed cases, but the authors faced grave resistance to publication, only achieved in February 2021. There is obviously intense hostility, both commercial and political, to reports that a repurposed drug of negligible cost and unparalleled safety achieves what the covid vaccines are now admitted not to have done.
The PRINCIPLE trial still has not published its results on Ivermectin. Results for other medications were published within a year but Ivermectin has been part of the trial since June 2021 with no results.
9.10 Paxlovid
Paxlovid, a Pfizer treatment, was approved in December 2021 for use in high-risk groups. Pfizer themselves reported a rebound of symptoms in a subset of patients at a similar rate to placebo. At first rebound was “rare,” at less than 1 percent, then 5.4 percent, then 10 percent. However, later evidence revealed it to be far more common than Pfizer’s claim, with a quarter of people experiencing rebound symptoms after Paxlovid treatment. The proposed solution was to study Paxlovid for effectiveness in treating rebound infections, rather than declaring it a failed drug that extends infection time.
9.11 Vitamin D
Vitamin D can improve immunity and suppress the inflammatory cytokine response, particularly important for covid, while low vitamin D levels predispose us to increased risk of respiratory tract infections and pneumonia. Systematic reviews and meta-analyses (both looking at the totality of the evidence) show that vitamin D supplementation reduced the risk of acute respiratory infection.
How does this translate to covid? A small number of studies found no difference, but no fewer than 20 studies showed that adults and children with low vitamin D levels were more likely to test positive for covid and several studies showed that they had more severe symptoms, a longer hospital stay, admission to intensive care or the high dependency unit and increased inflammation, blood clotting and acute respiratory distress syndrome (ARDS) with need for mechanical ventilation; a Spanish study found that over 82% of hospitalised covid patients had vitamin D deficiency. A meta-analysis of 23 studies containing 11,901 participants found that in patients with vitamin D deficiency, the risk of being infected with covid was 3.3 times higher and the risk of developing severe covid was around 5 times higher compared to those with more healthy vitamin D levels. A further 17 studies confirmed that in vitamin D-deficient individuals the risk of death was higher; a meta-analysis found that death could theoretically be avoided at vitamin D levels of 125 nmol/l. This is hardly surprising as we know that patients with severe covid have depleted numbers of critical immune cells and their function is exhausted.
It has been claimed that the above observations are due to coincidental correlations such that people with vitamin D deficiency are the same people with risk factors for covid.
In order to fairly test whether Vitamin D treatment has a benefit it is imperative that a sufficient dose is given early in the course of the illness when an enhanced immune response has an opportunity to protect against viral attack.
Two large UK studies found that use of vitamin D supplements was associated with a significantly lower risk of covid infection, while a Spanish study found that achieving blood levels of 75 nmol/l reduced infection incidence, severity and death. A meta-analysis found a consistently lower mortality rate among those given high dose oral vitamin D (60,000 to 80,000 IU a day). Covid patients given vitamin D to bring blood levels up to 75 nmol/l had a more than 50% decreased rate of death and a shortened hospital stay. Vitamin D-deficient patients given 280,000 IUs vitamin D over 7 weeks suffered significantly fewer deaths, while 200,000 IUs administered over two consecutive days significantly reduced transfer to intensive care and/or death. Vitamin D is now included in several successful covid treatment protocols including the French National Academy of Medicine.
Meta-analyses carried out by NICE have failed to distinguish between trials giving low and high doses and between patients who have normal vitamin D levels or insufficient levels at the outset of the trial. They included trials where only a single dose was given, where the doses were as low as 1,000 IU and where treatment was not begun before hospitalisation.
It appears from these covid studies that a minimum level should be 75 nmol/l, with a meta-analysis showing that death could theoretically be avoided at vitamin D levels of 125 nmol/l. Yet some doctors still believe that 50 nmol/l is sufficient. Indeed this lower level is necessary to prevent certain bone and muscle conditions, but it is inadequate for immune support. Many experts agree that for immunity, and particularly for severe covid prevention, a level of 100-150 nmol/l is necessary.
A double blind randomised controlled trial of a daily dose of 4,000 IU of Vitamin D was carried out in 2020 on healthcare workers and showed a 70% reduction in covid infections.
A study showed that in the UK over 61% had vitamin D levels below 50 nmol/l, i.e. an inadequate level even for prevention of those bone and muscle conditions, never mind the immune system. A large study showed that the UK had among the lowest mean vitamin D levels in Europe. Deficiency among people with dark skin is worse.
On 21st September 2020, Matt Hancock claimed that a British trial using Vitamin D had shown no impact. Officials later claimed this was a “slip of the tongue” as no such trial had taken place.
Vitamin D was not included as part of the PRINCIPLE or RECOVERY trials. One UK Vitamin D trial was not published, even as a preprint, until March 2022. It used a dose of 800 IU, was not double-blinded and showed that this level of Vitamin D does not prevent infection, but does not show whether Vitamin D can improve outcome after infection.
Three weeks later, on 15th October 2020, Matt Hancock said, “we will be increasing the public messaging around vitamin D to make sure that people get the message that vitamin D can help with your broad health and that there is no downside to taking it – and therefore people should consider that.” In November 2020, the government issued guidance that people should take 400 IU of vitamin D a day. This dose is considerably lower than the doses used in the studies to prevent covid and less than half the doses recommended to prevent osteoporosis.
10. UNEXPLAINABLE TIMELINES
| The attention given to what at first was a small cluster of pneumonia cases in China was out of proportion. A series of other events occurred earlier than any reasonable person would deem plausible. |
10.1 Previous outbreaks of unusual pneumonia did not lead to a similar response:
There was an outbreak where 111 people in China were diagnosed with pneumonia with 85 intensive care admissions and 30 deaths in June 2013. In Iran in 2015, there were 112 deaths and more than 1190 cases of H1N1 influenza resulting in the death of a nurse.
Neither of these events led to any reaction from other countries. What catapulted the entire world to the 2020 response? To say it was ‘out of proportion’ given the evident threat would be a mild understatement.
10.2 Premature response in early 2020:
The timeline of events in early 2020 is extremely suspicious.
- On 31st December 2019 the WHO were informed that there was a “cluster of cases of pneumonia” in China.
- On 31st December 2019, vaccine company Inovio, “began designing the INO-4800 vaccine on December 31, the day of the outbreak, after receiving a $9 million grant from Coalition for Epidemic Preparedness Innovations (Cepi), an initiative backed by Bill Gates.”
- On 5th January there were only 44 cases reported by the WHO.
- On 10th January 2020, the same day that the first sequence was first released, TIB Molbio shipped the first PCR test kits to Hong Kong, a day before anyone had been reported to have died from covid.
- The first death was announced from covid on 12th January 2020.
- On 12th January 2020, 4 more SARS-CoV-2 sequences were released. N.b., it is not possible to work up a test protocol in a single day.
- On 13th January 2020, the WHO accepted the Corman-Drosten PCR test protocol as the gold standard and published it. They commented on positive results from other coronaviruses saying, “Detection of these relatively distant members of the SARS-related CoV clade suggests that all Asian viruses are likely to be detected.”
- The Corman-Drosten protocol was submitted for publication in the journal EuroSurveillance on 21st January 2020 and went through the entire peer review, editorial review and typesetting process and was published within 24 hours.
10.3 Choice of vaccine molecule
- Laboratory and animal studies to choose which product to use BNT162 a/b/c and then BNT162b1/b2/b3 were ongoing until November 2020.
- On 9th June 2020, the first human was injected with BNT162b2, the molecule that was used.
- The next day, on 10th June 2020, Pfizer reported that they were already manufacturing the vaccine at risk in order to have enough supply (page 14). The supply needed to be of BNT162b2.
10.4 Timeline issues regarding Swine Flu
- The Pandemrix vaccine was “granted a marketing authorisation valid throughout the European Union for Pandemrix on 20 May 2008” by the European Commission.
- Also in 2008, the government advertised for suppliers of antiviral drugs.
- £10m was spent in 2008 to establish a National Flu Line for the distribution of antiviral medication for delivery in early 2009.
- The first report of a viral infection occurred on 18th March 2009.
11. FURTHER INVESTIGATIONS REQUIRED
- The Inquiry should insist that data that has been prevented from being made public is released. For example:
- Case rates, hospitalisation rates and death rates by vaccination status which was published by UKHSA only up until March 2022
- Case rates by number of doses given published by Public Health Scotland only up until early 2022.
- The full death by vaccination status data held by ONS up until end 2023 containing all relevant deaths not the fraction released to the public in August 2023.
- The data on positive PCR results including the Ct values to indicate the strength of the positive test and the symptom status of those tested before and after vaccination as held by the ONS from their surveillance reporting.
- The inquiry should also ask the NHS or UKHSA for data on late stage cancer presentations by age and vaccination status.
- There is considerable data on the Pfizer/BioNTech trial in the public domain thanks to the demands of a Texan court and despite objections from Pfizer and the FDA. Attempts to examine the equivalent data for the AstraZeneca trial have been rejected. However, the inquiry could seek exposure. Most importantly data on which patients developed covid like symptoms and when is critical. Only 40% of Moderna trial participants developed nucleocapsid antibodies after infection. Therefore, more information needs to be sought, in particular, how many antibody tests were done in the symptomatic and asymptomatic, placebo and vaccine groups and what was the timing of these tests and which of these patients had tested positive by PCR, and how weak were these positive results?
- The Inquiry should ask to see the full submissions from the pharmaceutical companies submitted to ensure compliance with the MHRA’s requirements for temporary use authorisation.
- The Inquiry should investigate how much vaccine was made before 26th November 2020, when the EMA noted that the manufacturing sites were not compliant with Good Manufacturing Practice.
- In order to properly quantify any deaths caused in the period shortly after vaccination, data could be sought of the date of death and date of each dose given for those who died. This can be anonymised by randomly adding or subtracting one, two or no days from each date. This is particularly important for investigating the deaths in young males. The ONS refused to share this data at Judicial review despite admitting that it was a statistically significant increase. The Government Legal Department stated on 12th January 2021, “the ONS recognises that more work could be undertaken to examine the mortality rates of young people in 2021, and intends to do so once more reliable data are available.” The Public Inquiry should seek this information.
- A selection of hospitals could be asked to carry out an audit of covid deaths. How many had respiratory symptoms? Did this proportion change over time and with vaccination? Were doctors recognising spike-type pathology in their patients but was it due to vaccination not infection? How many were diagnosed after admission and how many of those developed respiratory symptoms?
- Care home managers could be asked to report on what instructions they were given regarding access to healthcare, use of end-of-life medication and how deaths of their residents were diagnosed. In particular they could be asked how many died in March, April and May 2020 and in December 2020, January 2021 and February 2021 and how long after vaccination where applicable.
- The Public Inquiry could seek to investigate further deaths that have been given only a vague cause on the death certificate and request that a post mortem be carried out on all unexpected deaths in the young for a period.
- Deaths that have been referred to the coroner for investigation are not included in any reported data until after inquest. This is a major failing in terms of public health data collection as these are deaths that are most likely to be preventable. The inquiry could seek data from coroners as to the number of referrals for young people over time.
STATEMENT OF TRUTH
I believe that the facts stated in this witness statement are true. I understand that proceedings may be brought against anyone who makes, or causes to be made, a false statement in a document verified by a statement of truth without an honest belief of its truth.
Dr Clare Craig
January 2024

{kind=link}